You might also like
- Body Measurement Scale - 5599 Instruction ManualDocument11 pagesBody Measurement Scale - 5599 Instruction ManualRensek56No ratings yet
- Energy Expenditure LabDocument6 pagesEnergy Expenditure Labapi-311106200No ratings yet
- Urm Carestation 600 SeriesDocument264 pagesUrm Carestation 600 SeriesDenis Sined50% (2)
- Professional Nursing Practice Concepts and Perspectives 7th Edition Blais Test BankDocument26 pagesProfessional Nursing Practice Concepts and Perspectives 7th Edition Blais Test BankDebraWhitecxgn100% (49)
- Horn WebinarDocument53 pagesHorn WebinarGerr McGregorNo ratings yet
- Cardiovascular Fitness & ExerciseDocument33 pagesCardiovascular Fitness & Exercisewaqar aliNo ratings yet
- Nutricion Salud Metabolica Performnce Fisico y Obesidad SarcopenicaDocument15 pagesNutricion Salud Metabolica Performnce Fisico y Obesidad SarcopenicaMayra de CáceresNo ratings yet
- Health RecordDocument3 pagesHealth Recordpravat DashNo ratings yet
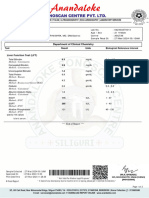
- Department of Chemical Pathology: Alpha Fetoprotein (AFP)Document1 pageDepartment of Chemical Pathology: Alpha Fetoprotein (AFP)Rashad AliNo ratings yet
- Revised JHS Map10 RSG WK4Document8 pagesRevised JHS Map10 RSG WK4Jerick SubadNo ratings yet
- Diferences in Strength Performance Between Novice and Elite PowerliftersDocument10 pagesDiferences in Strength Performance Between Novice and Elite PowerliftersEd Mac ChuNo ratings yet
- TDEE Calculator - ChallengeDocument7 pagesTDEE Calculator - Challenge2gasx23No ratings yet
- Biggest Loser Guidelines 4Document7 pagesBiggest Loser Guidelines 4Kuma TamersNo ratings yet
- Tutorial 516Document6 pagesTutorial 516corinna.ongaigui.gsbmNo ratings yet
- DEXA Scan (Sample)Document5 pagesDEXA Scan (Sample)Ashwin KNo ratings yet
- Body Fat Monitor HBF-306: Instruction ManualDocument20 pagesBody Fat Monitor HBF-306: Instruction Manual윤여평No ratings yet
- InBody260 CatalogDocument10 pagesInBody260 CatalogShubham TonkNo ratings yet
- InBody E Book PDFDocument48 pagesInBody E Book PDFu2197977No ratings yet
- Lecture5 - PA, Exercise, Fitness, and PA Domains - BBDocument45 pagesLecture5 - PA, Exercise, Fitness, and PA Domains - BBNaeema MosaNo ratings yet
- 乐心K102191Document7 pages乐心K102191Levi LeungNo ratings yet
- 2 - Energy Water PDFDocument11 pages2 - Energy Water PDFMelvin B. TarkporNo ratings yet
- B16 Pascual, Bien Oscar Magno-11-Mapanagutan-Activity 2 Score CardDocument3 pagesB16 Pascual, Bien Oscar Magno-11-Mapanagutan-Activity 2 Score CardBien PascualNo ratings yet
- MOP UP Round Allotment Result MD MS Course DME PG 2023Document35 pagesMOP UP Round Allotment Result MD MS Course DME PG 2023Falguni ChaturvediNo ratings yet
- Cole - Superior Capsular Reconstruction 5-14-19Document10 pagesCole - Superior Capsular Reconstruction 5-14-19JLavNo ratings yet
- Pre-Interpretation AssessmentDocument20 pagesPre-Interpretation Assessmentapi-637092426No ratings yet
- Writing Pre-InterpretationDocument20 pagesWriting Pre-Interpretationapi-639699202No ratings yet
- Color HandoutsDocument23 pagesColor HandoutsAndreea SlabuNo ratings yet
- Cindy Dianne Quiapo - Exercise No. 4Document9 pagesCindy Dianne Quiapo - Exercise No. 4Cindy Dianne QuiapoNo ratings yet
- Scale500 User Manual 2021Document147 pagesScale500 User Manual 2021Mamad mamsNo ratings yet
- Modification of Pronated Foot Posture After A Program of Therapeutic ExercisesDocument8 pagesModification of Pronated Foot Posture After A Program of Therapeutic ExercisesOguz GücinNo ratings yet
- Progress Tracker - Muscle BuildDocument62 pagesProgress Tracker - Muscle BuildBettina SebdenicsNo ratings yet
- We Are What We Repeatedly Do. Excellence, Then Is Not An Act, But A Haibt.Document8 pagesWe Are What We Repeatedly Do. Excellence, Then Is Not An Act, But A Haibt.tuan leNo ratings yet
- University of Santo Tomas Institute of Physical Education and AthleticsDocument3 pagesUniversity of Santo Tomas Institute of Physical Education and AthleticsJacob CasugboNo ratings yet
- Dietary Computation: Body Mass Index (BMI) Determination: NCM 105A Nutrition and Diet Therapy LaboratoryDocument4 pagesDietary Computation: Body Mass Index (BMI) Determination: NCM 105A Nutrition and Diet Therapy LaboratoryKryzza LeizellNo ratings yet
- BiaDocument7 pagesBiaDian WijayantiNo ratings yet
- Analysis of Body Composition Among Intercollegiate Male Volleyball PlayersDocument3 pagesAnalysis of Body Composition Among Intercollegiate Male Volleyball PlayersMunirajsNo ratings yet
- Successful and Unsuccessful Weight-Loss Maintainers - Strategies To Counteract Metabolic Compensation Following Weight LossDocument11 pagesSuccessful and Unsuccessful Weight-Loss Maintainers - Strategies To Counteract Metabolic Compensation Following Weight LossDouglas MarinNo ratings yet
- SyllDocument25 pagesSyllShivamNo ratings yet
- Periodic Health Examination Form 2 2020Document2 pagesPeriodic Health Examination Form 2 2020ohorateuuNo ratings yet
- Pon Vidyashram Group of Cbse Schools (Affiliated To CBSE - New Delhi)Document4 pagesPon Vidyashram Group of Cbse Schools (Affiliated To CBSE - New Delhi)RAMESH KUMARNo ratings yet
- V Alue B Ased M Edicine: Sudigdo SastroasmoroDocument20 pagesV Alue B Ased M Edicine: Sudigdo SastroasmoroLaode Maly RayNo ratings yet
- Allotment Result MOP UP Round MD MS Course DME PG Counselling 2023Document38 pagesAllotment Result MOP UP Round MD MS Course DME PG Counselling 2023vishalyadav5656No ratings yet
- Final Division Mass Training On PFTDocument20 pagesFinal Division Mass Training On PFTMarlyn Rico - TugahanNo ratings yet
- PSS Mentoring Checklist - Version 2.1 - 24.03.2021 - Laz + RLDocument6 pagesPSS Mentoring Checklist - Version 2.1 - 24.03.2021 - Laz + RLdaudjordienyirendaNo ratings yet
- Using Metabolic Equivalents in Clinical PracticeDocument6 pagesUsing Metabolic Equivalents in Clinical Practicejose luis sepulveda ortizNo ratings yet
- For The Student Learning Activity4Document1 pageFor The Student Learning Activity4jovan teopizNo ratings yet
- Lab ReportDocument2 pagesLab Report881Aritra PalNo ratings yet
- Inbody 12 - 07 - 21Document1 pageInbody 12 - 07 - 21Mahdi GuenifiNo ratings yet
- Ergo - Total ExpermentsDocument37 pagesErgo - Total ExpermentsJay PandiaNo ratings yet
- Ape Blank FormDocument1 pageApe Blank FormArlene Bermudez PascualNo ratings yet
- Medical For Athletes 1Document2 pagesMedical For Athletes 1arminaNo ratings yet
- Screenshttttt PDFDocument1 pageScreenshttttt PDF曾琳No ratings yet
- Medical For Athletes All Events DELGADODocument2 pagesMedical For Athletes All Events DELGADOmarie cristine caserNo ratings yet
- In Body R20Document6 pagesIn Body R20r4ph43l_20No ratings yet
- Notes:: GPST3 Full-TimeDocument1 pageNotes:: GPST3 Full-TimeHas MasNo ratings yet
- 2023 Weight Journal & Exercise LogDocument12 pages2023 Weight Journal & Exercise LogRadosław SzymańskiNo ratings yet
- Bnap 2024Document1 pageBnap 2024Aedrian MacawiliNo ratings yet
- Laboratory of Anatomy and Physical Activity Sciences, College of General Education, Ibaraki UniversityDocument8 pagesLaboratory of Anatomy and Physical Activity Sciences, College of General Education, Ibaraki UniversityJhonnyAndresBonillaHenaoNo ratings yet
- Pre-Assesment FinalDocument8 pagesPre-Assesment Finalapi-641177207No ratings yet
- TIME TABLE ODD SEM 2023 4th YEARDocument2 pagesTIME TABLE ODD SEM 2023 4th YEARtyagihemant281No ratings yet
- Warren Sweet - May 16Document15 pagesWarren Sweet - May 16warrenmsweetNo ratings yet
- Intro to Metabolic Enhancement Training (MET): Two Metabolic Weight Training Conditioning Programs for Fat Loss and Muscle GainFrom EverandIntro to Metabolic Enhancement Training (MET): Two Metabolic Weight Training Conditioning Programs for Fat Loss and Muscle GainRating: 4.5 out of 5 stars4.5/5 (8)
- Superhero AssignmentDocument5 pagesSuperhero Assignmentprathibha asok kumarNo ratings yet
- Titration LabDocument5 pagesTitration Labprathibha asok kumarNo ratings yet
- Adult General Passport Application: For Canadians 16 Years of Age or Over Applying in Canada or The USADocument7 pagesAdult General Passport Application: For Canadians 16 Years of Age or Over Applying in Canada or The USAmai nguyenNo ratings yet
- Energy LabDocument29 pagesEnergy Labprathibha asok kumarNo ratings yet
- Titration LabDocument5 pagesTitration Labprathibha asok kumarNo ratings yet
- Acculturation ResearchDocument2 pagesAcculturation Researchprathibha asok kumarNo ratings yet
- Chem3 1B v2 Feb17Document8 pagesChem3 1B v2 Feb17prathibha asok kumarNo ratings yet
- Field Trip Permission Slip - StudentDocument1 pageField Trip Permission Slip - StudentChristine Angelica EvangelistaNo ratings yet
- Medical TopicDocument25 pagesMedical Topicbhavana NandakumarNo ratings yet
- Data Pasien HipertensiDocument43 pagesData Pasien HipertensiDewi Antonia SiregarNo ratings yet
- B1 UNIT 4 Extra Grammar Practice ExtensionDocument1 pageB1 UNIT 4 Extra Grammar Practice ExtensiongabrielaNo ratings yet
- Nekky ExselDocument217 pagesNekky ExselpokjarspkNo ratings yet
- Daftar Nama ObatDocument22 pagesDaftar Nama Obatapotek anandaNo ratings yet
- Learning Exercise Chapter 6Document6 pagesLearning Exercise Chapter 6Shadow RazeNo ratings yet
- 3 - Pre-Analytical UnitDocument17 pages3 - Pre-Analytical UnitMary Cabalce100% (1)
- FORMAT LAPORAN MALARIA BARU DinasDocument5 pagesFORMAT LAPORAN MALARIA BARU DinasNoenoeNo ratings yet
- M3 Procedure of Entry1Document25 pagesM3 Procedure of Entry1Josh SamNo ratings yet
- Concepts of Community CHN2 090120Document62 pagesConcepts of Community CHN2 090120Pucha MorinNo ratings yet
- Orderan Apotek Rosa MalangDocument2 pagesOrderan Apotek Rosa MalangKristiana DewiNo ratings yet
- 001 Hilton Dr. Directory 2Document20 pages001 Hilton Dr. Directory 2Muhammad Siraj KhanNo ratings yet
- Shaheed Zulfiqar Ali Bhutto Medical University: Application FormDocument4 pagesShaheed Zulfiqar Ali Bhutto Medical University: Application FormSidraNo ratings yet
- Why We Sleep Mind MapDocument1 pageWhy We Sleep Mind Mapthecampaign45No ratings yet
- Mitsuya Et Al., 2023Document11 pagesMitsuya Et Al., 2023Rodrigo AlvesNo ratings yet
- Bharti Axa Health India Network HospitalsDocument530 pagesBharti Axa Health India Network HospitalsKumarNo ratings yet
- 15-03-00064 User Manual, English HDDocument125 pages15-03-00064 User Manual, English HDdodyNo ratings yet
- Rybelsus DataDocument252 pagesRybelsus Datasanskargaglani03No ratings yet
- FX PCv3.1 PDFDocument12 pagesFX PCv3.1 PDFKerry Prisel MoranNo ratings yet
- Contoh Soal PG Bahasa Inggris Kelas XI Semester 1 K13 Beserta JawabanDocument12 pagesContoh Soal PG Bahasa Inggris Kelas XI Semester 1 K13 Beserta JawabanIntan Wahyu DhamayantiNo ratings yet
- ID Analisis Pengelolaan Kesehatan Lingkungan Rumah Sakit Sebagai Usaha Pencegahan IDocument6 pagesID Analisis Pengelolaan Kesehatan Lingkungan Rumah Sakit Sebagai Usaha Pencegahan IKisah Dari LucasNo ratings yet
- 7703-Article Text-42970-1-10-20210526Document13 pages7703-Article Text-42970-1-10-20210526Raisa Louise Gamiao TattaoNo ratings yet
- BasingDocument6 pagesBasingAndri Septriadi100% (1)
- The Therapeutics of Acupuncture and Moxibustion (Otitis Media, Tinnitusdeafness, Toothache, Sore Throat)Document22 pagesThe Therapeutics of Acupuncture and Moxibustion (Otitis Media, Tinnitusdeafness, Toothache, Sore Throat)clerise3No ratings yet
- Rectal Exam Skill SheetDocument1 pageRectal Exam Skill SheetMuhammed ElgasimNo ratings yet
- Eco-5 NCPDocument86 pagesEco-5 NCPLokesh KumarNo ratings yet
- Self-Care Management in Adults Undergoing Hemodialysis: Cleo J. RichardDocument1 pageSelf-Care Management in Adults Undergoing Hemodialysis: Cleo J. Richardkamila auliaNo ratings yet