You might also like
- Inpatient Geriatric Psychiatry: Optimum Care, Emerging Limitations, and Realistic GoalsFrom EverandInpatient Geriatric Psychiatry: Optimum Care, Emerging Limitations, and Realistic GoalsHoward H. FennNo ratings yet
- Jer 12 3 194 PDFDocument8 pagesJer 12 3 194 PDFAlvian PemimpiNo ratings yet
- Assessment of Depression Among Older AdultsDocument9 pagesAssessment of Depression Among Older Adultsrani nauraNo ratings yet
- Health and Gender: Resilience and Vulnerability Factors For Women's Health in the Contemporary SocietyFrom EverandHealth and Gender: Resilience and Vulnerability Factors For Women's Health in the Contemporary SocietyIlaria TarriconeNo ratings yet
- Auriculotherapy To Reduce Anxiety and Pain in Nursing Professionals: A Randomized Clinical TrialDocument9 pagesAuriculotherapy To Reduce Anxiety and Pain in Nursing Professionals: A Randomized Clinical TrialСлавољуб КостићNo ratings yet
- Creemers Et Al. (2019) - PreventionDocument22 pagesCreemers Et Al. (2019) - PreventionMelNo ratings yet
- Jurnal MHCLN PeplauDocument10 pagesJurnal MHCLN Peplaubasok buhariNo ratings yet
- Hearing Voices: Qualitative Inquiry in Early PsychosisFrom EverandHearing Voices: Qualitative Inquiry in Early PsychosisNo ratings yet
- Jurnal ReadingDocument24 pagesJurnal ReadingRevienaNo ratings yet
- Gmez 2008 Transsexuals From Spain PDFDocument16 pagesGmez 2008 Transsexuals From Spain PDFTherese EspinosaNo ratings yet
- Centre For Policy On Ageing Information Service Selected ReadingsDocument62 pagesCentre For Policy On Ageing Information Service Selected ReadingsC Hendra WijayaNo ratings yet
- Agesim PaperDocument10 pagesAgesim PaperadilNo ratings yet
- The Impact of Emotional Support in Managing Cardiovascular Diseases Among Hispanic and Non -Hispanic Menopausal Women Aged 55 to 84 YearsFrom EverandThe Impact of Emotional Support in Managing Cardiovascular Diseases Among Hispanic and Non -Hispanic Menopausal Women Aged 55 to 84 YearsNo ratings yet
- Mental Health, Intellectual and Developmental Disabilities and the Ageing ProcessFrom EverandMental Health, Intellectual and Developmental Disabilities and the Ageing ProcessNo ratings yet
- Is Culture An Independent Variable in Psycho Geriatrics. The Case of Brazilian and Japanese ElderlyDocument4 pagesIs Culture An Independent Variable in Psycho Geriatrics. The Case of Brazilian and Japanese ElderlyGeriatric_NeurologyNo ratings yet
- Prevalence of Depression and Burden Among Informal Caregivers of People With Dementia: A Meta-AnalysisDocument75 pagesPrevalence of Depression and Burden Among Informal Caregivers of People With Dementia: A Meta-AnalysisCristina MPNo ratings yet
- Concurrent TreatmentDocument257 pagesConcurrent TreatmentRosi Del Rincon100% (2)
- 19 Babatsikou Original 10 3 PDFDocument10 pages19 Babatsikou Original 10 3 PDFade hastinNo ratings yet
- Jcop 22594Document15 pagesJcop 22594Shamså KånwalNo ratings yet
- 5063-5069 4.18 Pinar Sercekus PDFDocument7 pages5063-5069 4.18 Pinar Sercekus PDFNurul ShahirahNo ratings yet
- 27 Loh2015Document11 pages27 Loh2015Sergio Machado NeurocientistaNo ratings yet
- Chochinov - Dignity Therapy - A Feasibility Study of EldersDocument13 pagesChochinov - Dignity Therapy - A Feasibility Study of Eldersjuarezcastellar268No ratings yet
- Neurology, Psychiatry and Brain Research: B.A. Pramesona, S. TaneepanichskulDocument6 pagesNeurology, Psychiatry and Brain Research: B.A. Pramesona, S. TaneepanichskulMutiara Anak NegeriNo ratings yet
- Ho 2013Document6 pagesHo 2013Vera El Sammah SiagianNo ratings yet
- Gender Dysphoria and Social AnxietyDocument9 pagesGender Dysphoria and Social AnxietyJellybabyNo ratings yet
- Globalising Mental Health: A Neoliberal ProjectDocument7 pagesGlobalising Mental Health: A Neoliberal ProjectlizardocdNo ratings yet
- Psychopathology in Women: Incorporating Gender Perspective into Descriptive PsychopathologyFrom EverandPsychopathology in Women: Incorporating Gender Perspective into Descriptive PsychopathologyMargarita Sáenz-HerreroNo ratings yet
- RCT Spiritual ReminiscenceDocument8 pagesRCT Spiritual ReminiscencediyanarelNo ratings yet
- Social Aspects of The Quality of Life of Persons Suffering From SchizophreniaDocument11 pagesSocial Aspects of The Quality of Life of Persons Suffering From SchizophreniaFathur RNo ratings yet
- Who PhsycogeriatriDocument6 pagesWho PhsycogeriatriWilson WilliamNo ratings yet
- Vivir Con ParkinsonDocument22 pagesVivir Con ParkinsonAlexis Muñoz TrincadoNo ratings yet
- Effects of Dignity Therapy On Terminally Ill Patients: A Systematic ReviewDocument11 pagesEffects of Dignity Therapy On Terminally Ill Patients: A Systematic ReviewIwanNo ratings yet
- Chiang Et Al-2010-International Journal of Geriatric PsychiatryDocument9 pagesChiang Et Al-2010-International Journal of Geriatric PsychiatryFelipe Albornoz IllanesNo ratings yet
- 1 s2.0 S0883941722000905 MainDocument11 pages1 s2.0 S0883941722000905 MainReni Tri AstutiNo ratings yet
- Menopouse 26 45 PDFDocument21 pagesMenopouse 26 45 PDFevilasusantiNo ratings yet
- Suicidal Ideation, Depression and Quality of Life in The Elderly: Study in A Gerontopsychiatric ConsultationDocument10 pagesSuicidal Ideation, Depression and Quality of Life in The Elderly: Study in A Gerontopsychiatric ConsultationMinodora MilenaNo ratings yet
- Depression and The Elderly - FinalDocument8 pagesDepression and The Elderly - Finalapi-577539297No ratings yet
- Topic Name (Writer Name) (Instructor Name)Document20 pagesTopic Name (Writer Name) (Instructor Name)Hera ImranNo ratings yet
- 646-Article Text-1222-1-10-20210226Document10 pages646-Article Text-1222-1-10-20210226subanant11No ratings yet
- Debat Kel. FitrahDocument17 pagesDebat Kel. FitrahnurisNo ratings yet
- Marina Et Al 2021 Views of Psychologists About Their Role in Hastened DeathDocument16 pagesMarina Et Al 2021 Views of Psychologists About Their Role in Hastened DeathSofia CamachoNo ratings yet
- (2020) Perinatal Mental HealthDocument15 pages(2020) Perinatal Mental HealthRicardo EscNo ratings yet
- The Effects of Exercise Standards On The Quality of Life To People With Chronic DiseaseDocument18 pagesThe Effects of Exercise Standards On The Quality of Life To People With Chronic DiseaseMario LanzaNo ratings yet
- Psychosocial Support Groups For Patients With Multidrug Resistant Tuberculosis Five Years of ExperienceDocument15 pagesPsychosocial Support Groups For Patients With Multidrug Resistant Tuberculosis Five Years of ExperienceLinh NguyenNo ratings yet
- Cognitive Behavioral Therapy For Psychotic SymptomsDocument149 pagesCognitive Behavioral Therapy For Psychotic SymptomsCrina SerbanNo ratings yet
- Case Study On Severe Depression With Dissociative SpellsDocument59 pagesCase Study On Severe Depression With Dissociative SpellsAnshu PokharelNo ratings yet
- Multimodal Treatment of Acute Psychiatric Illness: A Guide for Hospital DiversionFrom EverandMultimodal Treatment of Acute Psychiatric Illness: A Guide for Hospital DiversionNo ratings yet
- Literature Review The Family Therapy and Non-FamilDocument6 pagesLiterature Review The Family Therapy and Non-FamilIsmael dos SantosNo ratings yet
- Stroke Article 1Document10 pagesStroke Article 1api-292843843No ratings yet
- The Nurses' Knowledge and Attitudes Towards The Palliative CareDocument10 pagesThe Nurses' Knowledge and Attitudes Towards The Palliative CareZein AhmadNo ratings yet
- Decision To Choose Acupuncture Therapy For Degenerative 'LVHDVHV DPRQJ WKH (OGHUO/ DW - D Idu 0Hglnd +rvslwdo KaranganyarDocument11 pagesDecision To Choose Acupuncture Therapy For Degenerative 'LVHDVHV DPRQJ WKH (OGHUO/ DW - D Idu 0Hglnd +rvslwdo KaranganyarSitilestariNo ratings yet
- Wilson 2016Document6 pagesWilson 2016wismaekaNo ratings yet
- 2016 Agli Frecnh PDFDocument13 pages2016 Agli Frecnh PDFnermal93No ratings yet
- Quality of Life in Caregivers of Patients With Schizophrenia A Literature ReviewDocument6 pagesQuality of Life in Caregivers of Patients With Schizophrenia A Literature Reviewgw0q12dxNo ratings yet
- Jurnal MHCLN PeplauDocument27 pagesJurnal MHCLN PeplauZuhriya MeilitaNo ratings yet
- Psychosomatic Medicine: An International Guide for the Primary Care SettingFrom EverandPsychosomatic Medicine: An International Guide for the Primary Care SettingNo ratings yet
- Ayahuasca Observational Study of GriefDocument13 pagesAyahuasca Observational Study of GriefSam JyotishiNo ratings yet
- Original Research ArticleDocument8 pagesOriginal Research ArticleNurul Agustina WatiNo ratings yet
- JohannesTownsendFerris 13 1Document24 pagesJohannesTownsendFerris 13 1HemantNo ratings yet
- Advertisements - Large (SSR)Document3 pagesAdvertisements - Large (SSR)HemantNo ratings yet
- Models of CurriculumDocument15 pagesModels of CurriculumHemantNo ratings yet
- Nurses Continuing Education With The Appproach of Distance EducationDocument11 pagesNurses Continuing Education With The Appproach of Distance EducationHemantNo ratings yet
- SullivanDocument6 pagesSullivanAlsah Iqbal30No ratings yet
- Classification of Drugs Acting On CNSDocument10 pagesClassification of Drugs Acting On CNSHemantNo ratings yet
- Autonomy Accountability AssertivenessDocument55 pagesAutonomy Accountability AssertivenessHemantNo ratings yet
- Psychosocial Wellbeingandcopingstrategiesof Infertile Women Seeking Infertility TreatmentDocument6 pagesPsychosocial Wellbeingandcopingstrategiesof Infertile Women Seeking Infertility TreatmentHemantNo ratings yet
- Aim and Objective Domain WiseDocument9 pagesAim and Objective Domain WiseHemantNo ratings yet
- Values, Conceptual Model and Approaches.Document27 pagesValues, Conceptual Model and Approaches.HemantNo ratings yet
- Pooja Seminar FinalDocument13 pagesPooja Seminar FinalHemantNo ratings yet
- FVVinObGyn 2 131 138Document8 pagesFVVinObGyn 2 131 138HemantNo ratings yet
- Cam TherapyDocument31 pagesCam TherapyHemantNo ratings yet
- A Psychological Study of Male, Female Related and Unexplained Infertility in Indian Urban CouplesDocument14 pagesA Psychological Study of Male, Female Related and Unexplained Infertility in Indian Urban CouplesHemantNo ratings yet
- Cam TherapyDocument35 pagesCam TherapyHemantNo ratings yet
- PSYCHOIMMUNOLOGYDocument23 pagesPSYCHOIMMUNOLOGYHemant100% (1)
- Theory of Moral DevelopmentDocument12 pagesTheory of Moral DevelopmentHemantNo ratings yet
- Attention-Deficit Hyperactivity Disorder: by Chris GolnerDocument22 pagesAttention-Deficit Hyperactivity Disorder: by Chris GolnerChaé RiNo ratings yet
- Extended and Expended Role of Nurse FINALDocument16 pagesExtended and Expended Role of Nurse FINALHemantNo ratings yet
- Sedative HypnoticsDocument3 pagesSedative HypnoticsHemantNo ratings yet
- 121220190CNS StimulantsDocument23 pages121220190CNS StimulantsHemantNo ratings yet
- Voiding DysfunctionsDocument50 pagesVoiding DysfunctionsHemantNo ratings yet
- Guillain Barrésyndrome (GBS) DisabilityScore NeurologicalScalesDocument1 pageGuillain Barrésyndrome (GBS) DisabilityScore NeurologicalScalesSutama ArtaNo ratings yet
- Health BeliefDocument30 pagesHealth BeliefHemantNo ratings yet
- Cns Stimulants: DR Laith M Abbas Al-Huseini M.B.CH.B, M.SC., M.Res., PH.DDocument38 pagesCns Stimulants: DR Laith M Abbas Al-Huseini M.B.CH.B, M.SC., M.Res., PH.DHemantNo ratings yet
- CNS Stimulants (2016-06)Document18 pagesCNS Stimulants (2016-06)HemantNo ratings yet
- BDI ScaleDocument3 pagesBDI ScaleDeborah Bravian TairasNo ratings yet
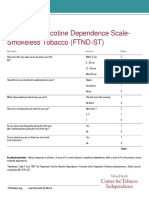
- Fagerstrom Scale For Nicotine Dependence Smokeless TobaccoDocument1 pageFagerstrom Scale For Nicotine Dependence Smokeless TobaccoHemantNo ratings yet
- The Rights of Persons With Disability Act, 2016 .34Document7 pagesThe Rights of Persons With Disability Act, 2016 .34HemantNo ratings yet
- Individual TherapyDocument7 pagesIndividual TherapyHemant100% (1)
- As A Man ThinkethDocument50 pagesAs A Man Thinkeththubtendrolma100% (5)
- ContinuingbondsDocument67 pagesContinuingbondsBrenda ChaconNo ratings yet
- Simplify Magazine: A Quarterly, Digital Publication For FamiliesDocument75 pagesSimplify Magazine: A Quarterly, Digital Publication For FamiliesGeorgiana MadalinaNo ratings yet
- Preventive, Promotive, Curative, RehabilitativeDocument54 pagesPreventive, Promotive, Curative, Rehabilitativetintu100% (1)
- Fischer Hoffman ProcessDocument11 pagesFischer Hoffman ProcessNatalie Douglas100% (1)
- Organizational Behaviour - Revision of Unit - 1Document5 pagesOrganizational Behaviour - Revision of Unit - 1bhavanyaNo ratings yet
- Capstone Project Title ProposalDocument4 pagesCapstone Project Title ProposalCapstoneNo ratings yet
- About TulpasDocument4 pagesAbout Tulpasvictorbessa96No ratings yet
- AggressionDocument21 pagesAggressionkhanminal466No ratings yet
- Addiction Report Psychologist MubeenDocument20 pagesAddiction Report Psychologist MubeenRafia ManzoorNo ratings yet
- Jurnal Berkaiatan Token EkonomiDocument14 pagesJurnal Berkaiatan Token EkonomithilaNo ratings yet
- Holistic Care in NursingDocument31 pagesHolistic Care in NursingKinley DorjiNo ratings yet
- Self-Discrepancy TheoryDocument29 pagesSelf-Discrepancy TheoryNitin GulwaniNo ratings yet
- Transactional AnalysisDocument10 pagesTransactional AnalysisBk Anubhav GuptaNo ratings yet
- Feelings and Needs SheetDocument2 pagesFeelings and Needs Sheetozanad7714No ratings yet
- The Self-Sabotage Cycle - Why We Repeat Behaviors That Create Hardships and Ruin Relationships (PDFDrive) PDFDocument193 pagesThe Self-Sabotage Cycle - Why We Repeat Behaviors That Create Hardships and Ruin Relationships (PDFDrive) PDFSubhajyoti Das100% (1)
- Health 7Document7 pagesHealth 7Markus Antonio Singelicio-SedicolNo ratings yet
- Compatibility of INFJ With ISFJ in Relationships TruityDocument6 pagesCompatibility of INFJ With ISFJ in Relationships TruityDarnell WoodardNo ratings yet
- Nursing Skill Book IDocument178 pagesNursing Skill Book IWahyu Dwi YuliyantiNo ratings yet
- Building Family Bridges WorkshopsDocument3 pagesBuilding Family Bridges WorkshopsFamily Court-CorruptionNo ratings yet
- 8 Dream Jobs For Adults With ADHD: From The ADHD Experts atDocument8 pages8 Dream Jobs For Adults With ADHD: From The ADHD Experts atPsicóloga Caroline Lopes Nogueira100% (2)
- PDF 5Document6 pagesPDF 5Sainath RacharlaNo ratings yet
- Case Study 1: Sigmund FreudDocument2 pagesCase Study 1: Sigmund FreudJoyce CeciliaNo ratings yet
- Lesson 1 Self DevelopmentDocument25 pagesLesson 1 Self DevelopmentRamos John CedricNo ratings yet
- The Role of Stigma in The Barriers To Mental Health Treatment inDocument33 pagesThe Role of Stigma in The Barriers To Mental Health Treatment inelshimyhebaNo ratings yet
- Caars Self L Int1Document9 pagesCaars Self L Int1Mona Refaei100% (1)
- GRAMMAR: Choose The Correct Answer To Fill in The BlankDocument2 pagesGRAMMAR: Choose The Correct Answer To Fill in The BlankDương LinhNo ratings yet
- Q1 - W6 - Key Concepts and Approaches (Part 3)Document39 pagesQ1 - W6 - Key Concepts and Approaches (Part 3)angie vibarNo ratings yet
- My Courses: Home Baed-Pdev2111-2012S Week 7: The Powers of The Mind Performancetask2Document4 pagesMy Courses: Home Baed-Pdev2111-2012S Week 7: The Powers of The Mind Performancetask2Daniel John D. Velasco67% (3)
- Perceptual DisordersDocument3 pagesPerceptual DisordersAkshayaaNo ratings yet