You might also like
- Horizontal Alveolar Ridge Augmentation in Implant Dentistry: A Surgical ManualFrom EverandHorizontal Alveolar Ridge Augmentation in Implant Dentistry: A Surgical ManualRating: 4.5 out of 5 stars4.5/5 (2)
- Therapy of the Hand and Upper Extremity: Rehabilitation ProtocolsFrom EverandTherapy of the Hand and Upper Extremity: Rehabilitation ProtocolsNo ratings yet
- Medical Coding Mock PapersDocument16 pagesMedical Coding Mock PapersSathya Kishore100% (4)
- Musculoskeletal 20,000 Series CPT Questions With Answers-CpcDocument16 pagesMusculoskeletal 20,000 Series CPT Questions With Answers-Cpcanchalnigam25100% (7)
- Musculo SkeletalDocument2 pagesMusculo SkeletalMilla TanNo ratings yet
- 2 Series CPTDocument7 pages2 Series CPTRenuka bhaskarNo ratings yet
- Answer Key: Introduction To Clinical CodingDocument101 pagesAnswer Key: Introduction To Clinical Codingthamizh555100% (1)
- 2 - SERIES 2023 Updated-2Document8 pages2 - SERIES 2023 Updated-219ucs175No ratings yet
- 3 - Series - Ans 2022Document5 pages3 - Series - Ans 2022Vijay UNo ratings yet
- CPC Answers 2010Document23 pagesCPC Answers 2010Beverly GraciousNo ratings yet
- 2011 Appendix A UpdatesDocument65 pages2011 Appendix A UpdatesfaithNo ratings yet
- Chapter 08 MusculoskeletalDocument5 pagesChapter 08 MusculoskeletalBernard Paul GuintoNo ratings yet
- Sternal Wound Procedures Require Coding Accuracy OpDocument4 pagesSternal Wound Procedures Require Coding Accuracy OpbushaesNo ratings yet
- Coding ZupkoDocument8 pagesCoding Zupkoashwanirana09No ratings yet
- Musculoskeletal System (20000 Series) : A) 20205 B) 20206 C) 20225 D) 27324Document8 pagesMusculoskeletal System (20000 Series) : A) 20205 B) 20206 C) 20225 D) 27324JJKNo ratings yet
- 2008 CPC Practice Exam Section 1 AnswersDocument12 pages2008 CPC Practice Exam Section 1 AnswersBeverly GraciousNo ratings yet
- 3 2 1 Code It 5th Edition Green Test Bank 1Document8 pages3 2 1 Code It 5th Edition Green Test Bank 1elizabeth100% (32)
- MEDICON 20000 Series With QuestionsDocument12 pagesMEDICON 20000 Series With Questionsnemalijyothsna3No ratings yet
- Archivetemp2018 TransCode Mock Test 4-AnswersDocument17 pagesArchivetemp2018 TransCode Mock Test 4-AnswersSathya Kishore100% (1)
- UrologyDocument29 pagesUrologyAnonymous MtKJkerbpU100% (1)
- Surgery 1Document10 pagesSurgery 1Harsha Vipin100% (1)
- RESOLVE MEDICODE-Coimbatore, Bangalore, Madurai (8148452460) CPC Mock Exam - 1Document32 pagesRESOLVE MEDICODE-Coimbatore, Bangalore, Madurai (8148452460) CPC Mock Exam - 1Abhishek Soni100% (1)
- 6 Series - Notes Need To WriteDocument9 pages6 Series - Notes Need To WriteVijay UNo ratings yet
- 1 - Series - Ans 2022Document5 pages1 - Series - Ans 2022Vijay UNo ratings yet
- 150 CPC Exam 2008 QuestionsDocument25 pages150 CPC Exam 2008 QuestionsBeverly Gracious100% (3)
- 150 CPC Exam 2008 QuestionsDocument25 pages150 CPC Exam 2008 QuestionsMagical 25100% (1)
- Sample Test Questions For The CPC ExamDocument8 pagesSample Test Questions For The CPC ExamHarikaSabbineniNo ratings yet
- Radiology Exercises 08022013Document3 pagesRadiology Exercises 08022013anishrove2No ratings yet
- CCS Exam Preparation CorrectionsDocument3 pagesCCS Exam Preparation CorrectionsNerry WasawordNo ratings yet
- CPC Practice Exam CDocument6 pagesCPC Practice Exam CAndrea Navarro100% (1)
- Q2 2020 PCS Coding ClinicDocument5 pagesQ2 2020 PCS Coding ClinicRashiden MadjalesNo ratings yet
- CPC Mock 10Document33 pagesCPC Mock 10Azra Muzafar100% (4)
- Series Coding Certification Tips - CompressDocument15 pagesSeries Coding Certification Tips - CompressAbhishek jogdandNo ratings yet
- Nervous SystemDocument11 pagesNervous SystemAnonymous MtKJkerbpUNo ratings yet
- PDF Q&aDocument15 pagesPDF Q&aArun Attrey75% (4)
- CPC Mock 8-Q-1Document19 pagesCPC Mock 8-Q-1Vishnu VichuZNo ratings yet
- MS Spine 2 Slide41Document2 pagesMS Spine 2 Slide41testNo ratings yet
- 4 - Series - Ans 2022Document6 pages4 - Series - Ans 2022Vijay UNo ratings yet
- Mock Exam - 1 QuestionsDocument23 pagesMock Exam - 1 QuestionsEva GraceNo ratings yet
- With AnswersDocument16 pagesWith AnswersHarsha Vipin75% (4)
- 2019 CCS - Self ReviewDocument5 pages2019 CCS - Self ReviewKash Jamasali91% (22)
- Berkshire CC Coding Chapter 4 ExamDocument8 pagesBerkshire CC Coding Chapter 4 Examcharlotte macairanNo ratings yet
- 3 - Series 2022Document9 pages3 - Series 2022Vijay UNo ratings yet
- Autologous Osteochondral Mosaicplasty For Osteochondritis Dissecans of The Elbow in Teenage AthletesDocument9 pagesAutologous Osteochondral Mosaicplasty For Osteochondritis Dissecans of The Elbow in Teenage AthletesAlejandro RamírezNo ratings yet
- 2023 CPT Coding ChangesDocument114 pages2023 CPT Coding ChangesJUNAID RAHMAN100% (1)
- PQ1Document50 pagesPQ1명수김100% (1)
- MS - Knee Arthroscopy - 1 - Slide16Document2 pagesMS - Knee Arthroscopy - 1 - Slide16testNo ratings yet
- Musculoskeletal System SurgeryDocument11 pagesMusculoskeletal System SurgeryAkhila sudheerbabuNo ratings yet
- Silo - Tips - Sample Test Questions For The CPC ExamDocument7 pagesSilo - Tips - Sample Test Questions For The CPC ExamBala Siva Murti OrganisationNo ratings yet
- Microstructural Scaffold Patch Insertion Without Autologous Cell Implantation For Repairing Symptomatic Chondral Knee Defects PDF 18998720410Document10 pagesMicrostructural Scaffold Patch Insertion Without Autologous Cell Implantation For Repairing Symptomatic Chondral Knee Defects PDF 18998720410JanetNo ratings yet
- MS Spine 1 Slide40Document2 pagesMS Spine 1 Slide40testNo ratings yet
- 1 - Series 2022Document9 pages1 - Series 2022Vijay U100% (1)
- Chapter 09 RespiratoryDocument3 pagesChapter 09 RespiratoryBernard Paul Guinto0% (2)
- Limb Reconstruction SystemDocument83 pagesLimb Reconstruction SystemGermán0% (1)
- PM 070 E0Document23 pagesPM 070 E0Radu HarliscaNo ratings yet
- Shoulder CodeDocument2 pagesShoulder CodeNasfikurNo ratings yet
- Sample QuestionsDocument15 pagesSample QuestionsAnonymous MtKJkerbpUNo ratings yet
- HCPCS-CPT QuizDocument16 pagesHCPCS-CPT QuizANAN FATHIMA SIRAJNo ratings yet
- Clinical Maxillary Sinus Elevation SurgeryFrom EverandClinical Maxillary Sinus Elevation SurgeryDaniel W. K. KaoNo ratings yet
- Minimally Invasive Periodontal Therapy: Clinical Techniques and Visualization TechnologyFrom EverandMinimally Invasive Periodontal Therapy: Clinical Techniques and Visualization TechnologyNo ratings yet
- 6 Series - Notes Need To WriteDocument9 pages6 Series - Notes Need To WriteVijay UNo ratings yet
- Colon & Digestive System AnatomyDocument12 pagesColon & Digestive System AnatomyVijay UNo ratings yet
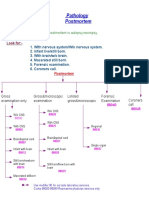
- Autopsy - NajboonDocument1 pageAutopsy - NajboonVijay UNo ratings yet
- Em 99 Series Full Part Need To WriteDocument18 pagesEm 99 Series Full Part Need To WriteVijay UNo ratings yet
- 7 Series (Radiology) : X-Ray Coding PointsDocument7 pages7 Series (Radiology) : X-Ray Coding PointsVijay UNo ratings yet
- Integumentary System ProceduresDocument13 pagesIntegumentary System ProceduresVijay UNo ratings yet
- 9 - Series - Ans 2022Document5 pages9 - Series - Ans 2022Vijay UNo ratings yet
- 99 Series QueDocument9 pages99 Series QueVijay UNo ratings yet
- 5 Series - Notes Need To WriteDocument9 pages5 Series - Notes Need To WriteVijay UNo ratings yet
- Using OLAP Tools for e-HRM AnalysisDocument27 pagesUsing OLAP Tools for e-HRM AnalysisVijay UNo ratings yet
- 9 - Series 2022Document8 pages9 - Series 2022Vijay UNo ratings yet
- 0 Series - Notes Need To TakeDocument6 pages0 Series - Notes Need To TakeVijay UNo ratings yet
- 3 - Series 2022Document9 pages3 - Series 2022Vijay UNo ratings yet
- 99 Series - ANSDocument7 pages99 Series - ANSVijay UNo ratings yet
- 4 - Series - Ans 2022Document6 pages4 - Series - Ans 2022Vijay UNo ratings yet
- 3 Series Respiratory SystemDocument8 pages3 Series Respiratory SystemVijay UNo ratings yet
- Arun PalaniswamyDocument15 pagesArun PalaniswamyVijay UNo ratings yet
- 9 series (medicine) Bio feedback and dialysisDocument10 pages9 series (medicine) Bio feedback and dialysisVijay UNo ratings yet
- 2 - Series 2022Document9 pages2 - Series 2022Vijay U100% (1)
- 1 - Series - Ans 2022Document5 pages1 - Series - Ans 2022Vijay UNo ratings yet
- 3 - Series - Ans 2022Document5 pages3 - Series - Ans 2022Vijay UNo ratings yet
- BALAMURUGAN D - CibilDocument3 pagesBALAMURUGAN D - CibilVijay UNo ratings yet
- 2 Series Class Notes Need To TakeDocument10 pages2 Series Class Notes Need To TakeVijay UNo ratings yet
- Neet PG 2023 PDFDocument3 pagesNeet PG 2023 PDFVijay UNo ratings yet
- Ilovepdf Merged PDFDocument7 pagesIlovepdf Merged PDFVijay UNo ratings yet
- Satheesh Kumar PDFDocument8 pagesSatheesh Kumar PDFVijay UNo ratings yet
- 1 - Series 2022Document9 pages1 - Series 2022Vijay U100% (1)
- Satheeshkumar R PDFDocument4 pagesSatheeshkumar R PDFVijay UNo ratings yet
- Folliculitis Decalvans Update July 2019 - Lay Reviewed July 2019Document4 pagesFolliculitis Decalvans Update July 2019 - Lay Reviewed July 2019sjeyarajah21No ratings yet
- Chairside Diagnostic Kit - Dr. PriyaDocument25 pagesChairside Diagnostic Kit - Dr. PriyaDr. Priya PatelNo ratings yet
- Gingival Tissue ManagementDocument36 pagesGingival Tissue ManagementSriram PugalenthiNo ratings yet
- Treatment of Dental Caries in The Young PermanentDocument39 pagesTreatment of Dental Caries in The Young PermanentShahid HameedNo ratings yet
- Periodontal DiseasesDocument47 pagesPeriodontal DiseasesPratikNo ratings yet
- Regional Sales Manager Medical Devices in Dallas FT Worth TX Resume James MooreDocument2 pagesRegional Sales Manager Medical Devices in Dallas FT Worth TX Resume James MooreJamesMoore2No ratings yet
- Encyclopedia of Cancer PDFDocument461 pagesEncyclopedia of Cancer PDFBachtiar Muhammad ArifNo ratings yet
- Effect of Steam Inhalation On Nasal Mucociliary Clearance in Normal Individuals and Nasal Disease Sta PDFDocument3 pagesEffect of Steam Inhalation On Nasal Mucociliary Clearance in Normal Individuals and Nasal Disease Sta PDFyolandaNo ratings yet
- Robertson2013 PDFDocument88 pagesRobertson2013 PDFArini NurlelaNo ratings yet
- Cornea PDFDocument465 pagesCornea PDFputraNo ratings yet
- Diabetes Mellitus ComplicationDocument40 pagesDiabetes Mellitus ComplicationHathorNo ratings yet
- Ms - CardiovascularDocument70 pagesMs - CardiovascularMark OngNo ratings yet
- Provision of Heel Cast For Treatment of Heel Ulcers December 2016 NWCEG GuidelineDocument39 pagesProvision of Heel Cast For Treatment of Heel Ulcers December 2016 NWCEG GuidelineneilNo ratings yet
- Perinatal Mental Health Policy BriefDocument3 pagesPerinatal Mental Health Policy BriefThe Wilson CenterNo ratings yet
- 2019 - 2020 - Boston Immunization - Hult Immunization FormDocument4 pages2019 - 2020 - Boston Immunization - Hult Immunization FormOscar RomainvilleNo ratings yet
- Nonadherence To Medications Among Persons With Bipolar Affective Disorder - A ReviewDocument9 pagesNonadherence To Medications Among Persons With Bipolar Affective Disorder - A ReviewIra DomunNo ratings yet
- (Pediaii) - 021 - Disorders of The Respiratory TractDocument17 pages(Pediaii) - 021 - Disorders of The Respiratory TractdoktoraronaNo ratings yet
- Physeo Microbiology 2019Document358 pagesPhyseo Microbiology 2019Harald Vogt100% (1)
- Psychedelics in Psychiatry-Keeping The Renaissance From Going Off The RailsDocument3 pagesPsychedelics in Psychiatry-Keeping The Renaissance From Going Off The RailsPaloma David VelasquezNo ratings yet
- Practical Guide To Insulin TherapyDocument40 pagesPractical Guide To Insulin TherapyjeyakanthaNo ratings yet
- Hyperosmolar Hyperglycemic StateDocument10 pagesHyperosmolar Hyperglycemic StateMirko S. León RguezNo ratings yet
- Amniotic MembraneDocument8 pagesAmniotic Membraneapi-481789048No ratings yet
- CARDIAC EMERGENCIES IN DAILY PRACTICEDocument45 pagesCARDIAC EMERGENCIES IN DAILY PRACTICEnikenNo ratings yet
- NCP - Ineffective Breathing PatternDocument4 pagesNCP - Ineffective Breathing PatternPRINCESS KOBAYASHINo ratings yet
- 2 Pathophysiology EpidemiologyDocument36 pages2 Pathophysiology EpidemiologyYosefina CindyNo ratings yet
- The Pharmacological History of Cannabis: January 2014Document22 pagesThe Pharmacological History of Cannabis: January 2014saraNo ratings yet
- Local Anesthetic Systemic Complications and TreatmentDocument35 pagesLocal Anesthetic Systemic Complications and Treatmentsatya_mdsNo ratings yet
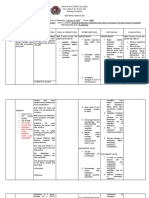
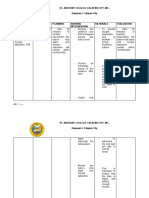
- St. Anthony College Calapan City, Inc. Bayanan I, Calapan CityDocument3 pagesSt. Anthony College Calapan City, Inc. Bayanan I, Calapan CityMike Faustino SolangonNo ratings yet
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailsCTM MURUGANNo ratings yet
- Brochura UrgoTul AGDocument4 pagesBrochura UrgoTul AGDaniguedesNo ratings yet