You might also like
- Lu K Uan Yu Taoist Yoga Alchemy and ImmortalityDocument229 pagesLu K Uan Yu Taoist Yoga Alchemy and Immortalitysegovia12345100% (3)
- Pancreas and SpleenDocument106 pagesPancreas and SpleenJorge De Vera100% (1)
- Notes From BoschDocument58 pagesNotes From BoschJohn Nixon100% (5)
- REFERAT Saraf FirdaDocument4 pagesREFERAT Saraf Firdanur bastianNo ratings yet
- Exercise to Prevent and Manage Chronic Disease Across the LifespanFrom EverandExercise to Prevent and Manage Chronic Disease Across the LifespanNo ratings yet
- Prepgenie Sample Full Test Answers PDFDocument16 pagesPrepgenie Sample Full Test Answers PDFjimNo ratings yet
- Summative Test #5 Gen BioDocument2 pagesSummative Test #5 Gen BioKennedy Fieldad Vagay100% (1)
- START Triage Training Presentation TTT 8 31 - 1 PDFDocument95 pagesSTART Triage Training Presentation TTT 8 31 - 1 PDFCM NajitoNo ratings yet
- INS119A RevC Carriere Motion ClassII Correction Appliance PDFDocument15 pagesINS119A RevC Carriere Motion ClassII Correction Appliance PDFchad smartNo ratings yet
- A Randomized Controlled Trial of High-Intensity Interval Training and Inspiratory Muscle Training For Chronic Heart Failure Patients With Inspiratory Muscle WeaknessDocument15 pagesA Randomized Controlled Trial of High-Intensity Interval Training and Inspiratory Muscle Training For Chronic Heart Failure Patients With Inspiratory Muscle WeaknessAprilleo ViedroNo ratings yet
- Exercise-Based Cardiac Rehabilitation Programs in Heart Failure PatientsDocument9 pagesExercise-Based Cardiac Rehabilitation Programs in Heart Failure PatientsheartfailureuitmNo ratings yet
- Begun H Et Al., (2020) Effect of Obesity OnDocument7 pagesBegun H Et Al., (2020) Effect of Obesity OnAna Flávia SordiNo ratings yet
- Impacto Del Ejercicios en CardiovascularDocument7 pagesImpacto Del Ejercicios en CardiovascularramonNo ratings yet
- Fibrosis PulmonarDocument9 pagesFibrosis PulmonarramonNo ratings yet
- JClinPrevCardiol63109-249318 065531Document6 pagesJClinPrevCardiol63109-249318 065531Himani PandyaNo ratings yet
- Effects of HIIT On Aerobic Capacity in Cardiac Patients, A Sistematic Review With Metanalysis - 2017Document17 pagesEffects of HIIT On Aerobic Capacity in Cardiac Patients, A Sistematic Review With Metanalysis - 2017alarconscamilaNo ratings yet
- Exercício Físico e Autofagia Seletiva Benefício e Risco Na Saúde CardiovascularDocument18 pagesExercício Físico e Autofagia Seletiva Benefício e Risco Na Saúde CardiovascularHenrique WilliamNo ratings yet
- Sugiharto 2019 IOP Conf. Ser. - Mater. Sci. Eng. 515 012033Document10 pagesSugiharto 2019 IOP Conf. Ser. - Mater. Sci. Eng. 515 012033Mella umi nurhalizaNo ratings yet
- Jurnal KardioDocument8 pagesJurnal KardioHalimah SadiahNo ratings yet
- Effect of Intermittent Isometric Handgrip Exercise Protocol With Short Exercise Duration On Cognitive PerformanceDocument7 pagesEffect of Intermittent Isometric Handgrip Exercise Protocol With Short Exercise Duration On Cognitive PerformanceRebeca BarrosNo ratings yet
- HIIT in Patients With Lifestyle-Induced Cardiometabolic Disease - A Systematic Review and Meta-AnalysisDocument10 pagesHIIT in Patients With Lifestyle-Induced Cardiometabolic Disease - A Systematic Review and Meta-AnalysisdariorguezNo ratings yet
- Potential Adverse Cardiovascular Effects From Excessive Endurance ExerciseDocument9 pagesPotential Adverse Cardiovascular Effects From Excessive Endurance Exercisewfaachannel8No ratings yet
- Feasibility and Estimated Efficacy of Blood Flow Restricted Training in Female Patients With Rheumatoid Arthritis A Randomized Controlled Pilot StudyDocument10 pagesFeasibility and Estimated Efficacy of Blood Flow Restricted Training in Female Patients With Rheumatoid Arthritis A Randomized Controlled Pilot StudyDaniel Andrés Bulla GarcíaNo ratings yet
- Brazilian Journal of Physical TherapyDocument12 pagesBrazilian Journal of Physical TherapyKen ABNo ratings yet
- Cardiac HypertrophyDocument9 pagesCardiac HypertrophyJulia WindiNo ratings yet
- Meine Azambuja 2020 Inspiratory Muscle Training in Patients With Heart Failure What Is NewDocument32 pagesMeine Azambuja 2020 Inspiratory Muscle Training in Patients With Heart Failure What Is Newtaaaatan.04No ratings yet
- The Endocannabinoid System and Physical ExerciseDocument23 pagesThe Endocannabinoid System and Physical ExerciseSantiago Hurtado GómezNo ratings yet
- High Intensity Interval Training Versus Moderate Intensity Continuous Training Within Cardiac Rehabilitation A Systematic Review and Meta AnalysisDocument18 pagesHigh Intensity Interval Training Versus Moderate Intensity Continuous Training Within Cardiac Rehabilitation A Systematic Review and Meta AnalysisAnatomska CentralaNo ratings yet
- Effectiveness and Approach of Rehabilitation in Patients With Acute Heart Failure: A ReviewDocument17 pagesEffectiveness and Approach of Rehabilitation in Patients With Acute Heart Failure: A ReviewheartfailureuitmNo ratings yet
- JURNAL 26 NadaDocument18 pagesJURNAL 26 NadaResky Ika Sah PutriNo ratings yet
- Heart EksDocument11 pagesHeart EksAndri FerdianNo ratings yet
- The Journal of Physiology - 2021 - Sabag - Low Volume High Intensity Interval Training For Cardiometabolic HealthDocument14 pagesThe Journal of Physiology - 2021 - Sabag - Low Volume High Intensity Interval Training For Cardiometabolic HealthBruno TeixeiraNo ratings yet
- Final Project Exp590-3Document19 pagesFinal Project Exp590-3api-315973465No ratings yet
- IntervalexercisetrialAnnals2006 PDFDocument12 pagesIntervalexercisetrialAnnals2006 PDFrunmenNo ratings yet
- Phenomenon of Athlete'S Heart, Positive Physiological Adaptation To Exercise: When and How?Document6 pagesPhenomenon of Athlete'S Heart, Positive Physiological Adaptation To Exercise: When and How?Jasmina Pluncevic GligoroskaNo ratings yet
- Cardiac Rehabilitation Exercise and Self-Care For Chronic Heart FailureDocument8 pagesCardiac Rehabilitation Exercise and Self-Care For Chronic Heart Failure黎欣慈No ratings yet
- Isaksen 2019Document8 pagesIsaksen 2019Filipe MendesNo ratings yet
- Chronic Stroke Patients Show Early and Robust Improvements in Muscle and Functional Performance in Response To..Document11 pagesChronic Stroke Patients Show Early and Robust Improvements in Muscle and Functional Performance in Response To..RobertoNo ratings yet
- The Effectiveness of 5 Weeks of High Intensity Interval Training On Cardiovascular Endurance in Karate Players: An Experimental StudyDocument6 pagesThe Effectiveness of 5 Weeks of High Intensity Interval Training On Cardiovascular Endurance in Karate Players: An Experimental StudyAmruta BhagwatNo ratings yet
- Efficacy and Safety of A Combined Aerobic, Strength and Flexibility Exercise Training Program in Patients With Implantable Cardiac Devices-2022Document10 pagesEfficacy and Safety of A Combined Aerobic, Strength and Flexibility Exercise Training Program in Patients With Implantable Cardiac Devices-2022Josemi Del Castillo MolinaNo ratings yet
- Ejercicio IntervalosDocument7 pagesEjercicio IntervalosOmar DVNo ratings yet
- Abstract Jincartos 19 - Eng-1Document1 pageAbstract Jincartos 19 - Eng-1Wikan PutridewiNo ratings yet
- Cipryan 2018Document9 pagesCipryan 2018197Anzali CahyatiNo ratings yet
- JurnalDocument11 pagesJurnalanindia wardhaniNo ratings yet
- Muscle Stem Cell and Physical Activity What Point Is The Debate atDocument13 pagesMuscle Stem Cell and Physical Activity What Point Is The Debate atZhao RuidiNo ratings yet
- Comparison of High-Intensity IDocument17 pagesComparison of High-Intensity IIulian-Stefan HOLUBIACNo ratings yet
- Sport 2Document11 pagesSport 2Nikola TanaskovicNo ratings yet
- 2022 Effects of Blood Flow Restriction Combined With Low-Intensity Resistance Training On Lower-Limb Muscle Strength and Mass in Post-Middle-Aged Adults.....Document15 pages2022 Effects of Blood Flow Restriction Combined With Low-Intensity Resistance Training On Lower-Limb Muscle Strength and Mass in Post-Middle-Aged Adults.....Antofa V EndeNo ratings yet
- JURNAL 18 GordonDocument17 pagesJURNAL 18 GordonResky Ika Sah PutriNo ratings yet
- Hsieh. Effects of High-Intensity Exercise Training in A Pulmonary Rehabilitation Programme For Patients With COPDDocument8 pagesHsieh. Effects of High-Intensity Exercise Training in A Pulmonary Rehabilitation Programme For Patients With COPDSofia MandolaNo ratings yet
- The Effect of Pursed - Lip Breathing Exercise Vs Diaphragmatic Breathing in Stabilizing The Vitals After 6-MWT Among Overweight Individuals-IJRASETDocument12 pagesThe Effect of Pursed - Lip Breathing Exercise Vs Diaphragmatic Breathing in Stabilizing The Vitals After 6-MWT Among Overweight Individuals-IJRASETIJRASETPublicationsNo ratings yet
- Fasten AuDocument10 pagesFasten AuDina M LestaryNo ratings yet
- Inspiratory Muscle Training Potentiates The Beneficial Effects of Proportional Assisted Ventilation On Exertional Dyspnea and Exercise Tolerance inDocument9 pagesInspiratory Muscle Training Potentiates The Beneficial Effects of Proportional Assisted Ventilation On Exertional Dyspnea and Exercise Tolerance inZulfah MidahNo ratings yet
- Article 4Document12 pagesArticle 4obichideravicNo ratings yet
- 2022 Article 1233Document24 pages2022 Article 1233orellanaroco.10No ratings yet
- New Approaches in Pulmonary RehabilitationDocument10 pagesNew Approaches in Pulmonary Rehabilitationzwecker4458No ratings yet
- Ncbi PulmoDocument17 pagesNcbi PulmoMuada AsqilaNo ratings yet
- High-Intensity Interval Training in Cardiac RehabilitationDocument20 pagesHigh-Intensity Interval Training in Cardiac RehabilitationdariorguezNo ratings yet
- Japplphysiol 01078 2017Document12 pagesJapplphysiol 01078 2017Zulfah MidahNo ratings yet
- 33 Dr. Reham Adel After Reviewing DiscDocument14 pages33 Dr. Reham Adel After Reviewing DiscnidyaNo ratings yet
- Acute Hypotensive Response To Continuous and Accumulated Isocaloric Aerobic BoutsDocument8 pagesAcute Hypotensive Response To Continuous and Accumulated Isocaloric Aerobic BoutsLeticia N. S. NevesNo ratings yet
- CHF 4Document8 pagesCHF 4Prameswari ZahidaNo ratings yet
- Paper Epoc PDFDocument5 pagesPaper Epoc PDFNicolás Celis MonroyNo ratings yet
- High Intensity Interval Training For Patients With Cardiovascular Disease-Is It Safe A Systematic ReviewDocument19 pagesHigh Intensity Interval Training For Patients With Cardiovascular Disease-Is It Safe A Systematic Reviewling lungNo ratings yet
- 3086 FullDocument10 pages3086 FullMaulida PuspitasariNo ratings yet
- EIM-FactSheet CoronaryHD Professionals FINAL-webDocument2 pagesEIM-FactSheet CoronaryHD Professionals FINAL-webDimasPrasetyoNo ratings yet
- Otot Rangka Dan Latihan-Main WordDocument5 pagesOtot Rangka Dan Latihan-Main WordGandhira AkbarNo ratings yet
- Strength For WarfightersDocument12 pagesStrength For Warfightersbeltran230111No ratings yet
- MODULe 1 Ana PhysioDocument10 pagesMODULe 1 Ana Physiojoshua ordenaNo ratings yet
- Đề thi cuối kỳ 2 môn Tiếng Anh lớp 12 Trường THPT Ngô Gia Tự năm 2020-2021Document3 pagesĐề thi cuối kỳ 2 môn Tiếng Anh lớp 12 Trường THPT Ngô Gia Tự năm 2020-2021quynh phuongNo ratings yet
- Pathophysiology of Cardiogenic Pulmonary Edema - UpToDateDocument9 pagesPathophysiology of Cardiogenic Pulmonary Edema - UpToDateRoberto López MataNo ratings yet
- Annex I Summary of Product CharacteristicsDocument118 pagesAnnex I Summary of Product Characteristicsandi namirahNo ratings yet
- Section 3: Medical Nutrition TherapyDocument46 pagesSection 3: Medical Nutrition TherapygopscharanNo ratings yet
- Anatomy Unit 4 - Tissue TypesDocument31 pagesAnatomy Unit 4 - Tissue TypesDevaki SubramaniamNo ratings yet
- Modified by Dr. Salah H Sinjary College of Medicine HMU Department of Medicine 07504454134Document47 pagesModified by Dr. Salah H Sinjary College of Medicine HMU Department of Medicine 07504454134Chro MANo ratings yet
- Adminisitration of OxygenDocument2 pagesAdminisitration of OxygenHamss AhmedNo ratings yet
- Pulmonary Rehabilitation (S)Document79 pagesPulmonary Rehabilitation (S)liz100% (3)
- Exam Question So Far Save My Exams MARK SCHEMEDocument11 pagesExam Question So Far Save My Exams MARK SCHEMEArooj AbidNo ratings yet
- 5090 w11 Ms 62Document3 pages5090 w11 Ms 62mstudy123456No ratings yet
- Assignment DPS BIO Practice Paper-01 Class-X 0110Document2 pagesAssignment DPS BIO Practice Paper-01 Class-X 0110amartyaNo ratings yet
- LeukemiaDocument8 pagesLeukemiapriscillaNo ratings yet
- 294 Fetal Heart Rate Monitoring. Principles and Interpretation of Cardiotocography LR PDFDocument9 pages294 Fetal Heart Rate Monitoring. Principles and Interpretation of Cardiotocography LR PDFelenNo ratings yet
- Gastrointestinal AnaphysioDocument7 pagesGastrointestinal AnaphysioJanine SantosNo ratings yet
- Video - Recap - of - Cells Intro - Recap - by - Amoeba - SistersDocument2 pagesVideo - Recap - of - Cells Intro - Recap - by - Amoeba - SistersLizandra AraujoNo ratings yet
- Fao - Tilmicosin DraftDocument37 pagesFao - Tilmicosin DraftandreililioanceaNo ratings yet
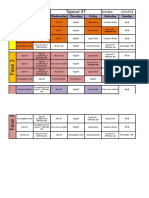
- Tapout XT: Monday Tuesday Wednesday Thursday Friday Saturday SundayDocument7 pagesTapout XT: Monday Tuesday Wednesday Thursday Friday Saturday SundayGiezi MisaelNo ratings yet
- Intracranial HypertensionDocument28 pagesIntracranial HypertensionHussein TarhiniNo ratings yet
- Dalhousie Dyspnea ScalesDocument7 pagesDalhousie Dyspnea ScalesOxana TurcuNo ratings yet
- Pathology Images MarrowDocument21 pagesPathology Images MarrowRAJDEEP DASNo ratings yet
- Small BowelDocument7 pagesSmall BowelIfeanyichukwu OgbonnayaNo ratings yet