You might also like
- Amniotic FluidDocument3 pagesAmniotic FluidanonacadsNo ratings yet
- A8 - AMNIOTIC FLUIDDocument4 pagesA8 - AMNIOTIC FLUIDJuan De la CruzNo ratings yet
- Amniotic Fluid Physiology Chemical CompositionDocument5 pagesAmniotic Fluid Physiology Chemical CompositionMichelle San Miguel FeguroNo ratings yet
- Amniotic Fluid: Learning ObjectivesDocument11 pagesAmniotic Fluid: Learning ObjectivesWho KnowsNo ratings yet
- Amniotic FluidDocument7 pagesAmniotic FluidCherralaine CorderoNo ratings yet
- Amniotic Fluid Final HandoutDocument15 pagesAmniotic Fluid Final HandoutBae RonaNo ratings yet
- Aubf Finals TransDocument7 pagesAubf Finals TransElijah Mae MundocNo ratings yet
- Amniotic Fluid AnalysisDocument6 pagesAmniotic Fluid Analysisdan paolo sanchezNo ratings yet
- Amniotic Fluid AnalysisDocument6 pagesAmniotic Fluid Analysisdan paolo sanchezNo ratings yet
- OB - Disorders of The Amniotic Fluid (CCT)Document6 pagesOB - Disorders of The Amniotic Fluid (CCT)gellie gellesNo ratings yet
- Urinalysis and Body Fluids - Strasinger, Susan King, Di Lorenzo, Marjorie Schaub (1) .pdf-258-268Document11 pagesUrinalysis and Body Fluids - Strasinger, Susan King, Di Lorenzo, Marjorie Schaub (1) .pdf-258-268Remark AmbananNo ratings yet
- Amniotic Fluid: Learning ObjectivesDocument8 pagesAmniotic Fluid: Learning ObjectivesJym TampusNo ratings yet
- Prematurely Ruptured of Membranes (PROM)Document23 pagesPrematurely Ruptured of Membranes (PROM)NiNie Sie MbakayuNeNo ratings yet
- 109Document3 pages109Angel MoncadaNo ratings yet
- AUBF - Amniotic Fluid and Semen Study MaterialDocument10 pagesAUBF - Amniotic Fluid and Semen Study MaterialVienna Jamaica Be Cari-CariNo ratings yet
- Fetal DevelopmentDocument5 pagesFetal DevelopmentHazelGraceNo ratings yet
- Ward TeachingDocument23 pagesWard Teachingvani reddyNo ratings yet
- Disorders of AFV Placenta and Fetal Memberanes Dr. Olivar 2022Document5 pagesDisorders of AFV Placenta and Fetal Memberanes Dr. Olivar 2022Hans Aldrin AbocNo ratings yet
- Physiology of Labor PDFDocument68 pagesPhysiology of Labor PDFAJ MendozaNo ratings yet
- Amniotic Fluid: Intramembranous Flow - Absorption of AFDocument6 pagesAmniotic Fluid: Intramembranous Flow - Absorption of AFOsannah Irish InsongNo ratings yet
- Amniotic Fluid EmbolismDocument16 pagesAmniotic Fluid EmbolismShuaiba CutieNo ratings yet
- 8 Physio OB - Physiology of Labor I - IIDocument14 pages8 Physio OB - Physiology of Labor I - IIArnoldBorromeoNo ratings yet
- OBII - 16 Postterm Pregnancy - PDF Version 1Document6 pagesOBII - 16 Postterm Pregnancy - PDF Version 1Felina CabadingNo ratings yet
- Midterm PPT MaternalDocument6 pagesMidterm PPT MaternalJhayneNo ratings yet
- Placenta and Extraembryonic MembranesDocument19 pagesPlacenta and Extraembryonic MembranesYose RizalNo ratings yet
- Hemangiomas of InfancyDocument20 pagesHemangiomas of InfancynissaNo ratings yet
- Amniotic FluidDocument5 pagesAmniotic FluidPat Cabanit0% (1)
- Midterm PPT MaternalDocument13 pagesMidterm PPT Maternaladrianleet18No ratings yet
- Hydra Mi NosDocument8 pagesHydra Mi NosSudha DeviNo ratings yet
- OligohydramniosDocument9 pagesOligohydramniosDeepika Patidar0% (1)
- Amniotic Fluid and Placenta AbnormalitiesDocument60 pagesAmniotic Fluid and Placenta AbnormalitiesMicah Lou CalambaNo ratings yet
- Amniotic FluidDocument4 pagesAmniotic FluidxiumethemoneyNo ratings yet
- NCM 108 - Nursing Care During Normal Pregnancy and Care of The Developing FetusDocument5 pagesNCM 108 - Nursing Care During Normal Pregnancy and Care of The Developing FetusKristine BartsNo ratings yet
- PROMDocument59 pagesPROMTalye begashawNo ratings yet
- Amnion 3Document18 pagesAmnion 3yani marlinaNo ratings yet
- Lect12 - Amniotic Fluid ModifiedDocument22 pagesLect12 - Amniotic Fluid Modifiedyelisetti DakshayaniNo ratings yet
- Hydramnios or PolyhydramniosDocument4 pagesHydramnios or PolyhydramniosAngel MoncadaNo ratings yet
- Balance de Agua en El Feto y El Recién NacidoDocument5 pagesBalance de Agua en El Feto y El Recién NacidoCarlos ReveloNo ratings yet
- Amniotic FluidDocument31 pagesAmniotic FluidPrincessJielRamirezNo ratings yet
- Respiratory Distress SyndromeDocument3 pagesRespiratory Distress SyndromeLuigi GeduqueNo ratings yet
- Subject-Obstetrical and Gynecological Nursing: TopicDocument2 pagesSubject-Obstetrical and Gynecological Nursing: TopicBhawna JoshiNo ratings yet
- Amniotic FluidDocument29 pagesAmniotic FluidZeytun AbdullahiNo ratings yet
- Amnion 1Document2 pagesAmnion 1Oryza SativaniNo ratings yet
- Amniotic Fluid EmbolismDocument10 pagesAmniotic Fluid EmbolismRebecca ApeladoNo ratings yet
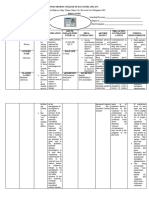
- Drug Study Format 1Document3 pagesDrug Study Format 1Janeenne Fe Nicole SilvanoNo ratings yet
- OB-amniotic FluidDocument10 pagesOB-amniotic FluidMicah Lou CalambaNo ratings yet
- Unit 2 FinalDocument127 pagesUnit 2 FinalaucukagapeNo ratings yet
- Amniotuc FluidDocument9 pagesAmniotuc FluidYormae QuezonNo ratings yet
- Poly Hi DR AmnionDocument7 pagesPoly Hi DR Amnionwanwan_adongNo ratings yet
- Amniotic Fluid: Group 5Document29 pagesAmniotic Fluid: Group 5Francis ValdezNo ratings yet
- Module No. Date: Topic:: Cues/Questions/Keywords NotesDocument103 pagesModule No. Date: Topic:: Cues/Questions/Keywords Notesanon ymousNo ratings yet
- Gestational and Placental Disorders: Ovary Pregnancy Results From TheDocument4 pagesGestational and Placental Disorders: Ovary Pregnancy Results From TheyepNo ratings yet
- Hydramnios and Premature Rupture of MembranesDocument5 pagesHydramnios and Premature Rupture of Membranessarguss14No ratings yet
- Fetal MembranesDocument17 pagesFetal MembranesQaiser InayatNo ratings yet
- AmnioticDocument7 pagesAmnioticCasey del RosarioNo ratings yet
- Complications of Pregnancy: Jose, Leana Louisse D. BSN 2BDocument14 pagesComplications of Pregnancy: Jose, Leana Louisse D. BSN 2BLiana Louisse JoseNo ratings yet
- MCN LectureDocument8 pagesMCN LectureEmily BernatNo ratings yet
- LaporDocument4 pagesLapormohammed alkanani100% (1)
- HISTOPATH ImmunohistochemistryDocument3 pagesHISTOPATH ImmunohistochemistryRichelyn Grace B. VenusNo ratings yet
- AUBF Serous FluidDocument7 pagesAUBF Serous FluidRichelyn Grace B. VenusNo ratings yet
- HISTOPATH AutopsyDocument2 pagesHISTOPATH AutopsyRichelyn Grace B. Venus0% (1)
- AUBF SemenDocument7 pagesAUBF SemenRichelyn Grace B. VenusNo ratings yet
- BACTE NonfermentativeDocument3 pagesBACTE NonfermentativeRichelyn Grace B. VenusNo ratings yet
- AUBF Synovial FluidDocument6 pagesAUBF Synovial FluidRichelyn Grace B. VenusNo ratings yet
- AUBF Gastric AnalysisDocument3 pagesAUBF Gastric AnalysisRichelyn Grace B. VenusNo ratings yet
- Historical Overview of ImmunohematologyDocument3 pagesHistorical Overview of ImmunohematologyRichelyn Grace B. VenusNo ratings yet
- HISTOPATH AdhesivesDocument2 pagesHISTOPATH AdhesivesRichelyn Grace B. VenusNo ratings yet
- Cancer and The Philippine Cancer Control ProgramDocument11 pagesCancer and The Philippine Cancer Control ProgramcamilleNo ratings yet
- SET UP Computer ServerDocument3 pagesSET UP Computer ServerRicHArdNo ratings yet
- NUFLO Low Power Pre-Amplifier: SpecificationsDocument2 pagesNUFLO Low Power Pre-Amplifier: SpecificationsJorge ParraNo ratings yet
- Statement of Cash Flows AnswerDocument3 pagesStatement of Cash Flows Answeranber mohammadNo ratings yet
- DD 3600 3500 3000 Parts CatalogDocument46 pagesDD 3600 3500 3000 Parts CatalogAndres Fdo Mora D100% (2)
- SmoothWall Express 2.0 Quick-Start GuideDocument6 pagesSmoothWall Express 2.0 Quick-Start Guideinfobits100% (1)
- Shaft DeflectionDocument15 pagesShaft Deflectionfreek_jamesNo ratings yet
- Bell Single-Sleeve Shrug Crochet PatternDocument2 pagesBell Single-Sleeve Shrug Crochet PatternsicksoxNo ratings yet
- GENUS Clock Gating Timing CheckDocument17 pagesGENUS Clock Gating Timing Checkwasimhassan100% (1)
- Sample Hum RepDocument21 pagesSample Hum RepPritam PiyushNo ratings yet
- Complex Poly (Lactic Acid) - Based - 1Document20 pagesComplex Poly (Lactic Acid) - Based - 1Irina PaslaruNo ratings yet
- Applied Computational AerodynamicsDocument15 pagesApplied Computational AerodynamicsjoereisNo ratings yet
- FCC O Cials Denounce Lawmakers' Attempts To Censor NewsroomsDocument52 pagesFCC O Cials Denounce Lawmakers' Attempts To Censor NewsroomsKeithStewartNo ratings yet
- Taxonomy: Family StaphylococcaceaeDocument40 pagesTaxonomy: Family StaphylococcaceaeMarissa Terrado SorianoNo ratings yet
- Lahainaluna High School Cafeteria: Lahaina, Maui, HawaiiDocument42 pagesLahainaluna High School Cafeteria: Lahaina, Maui, HawaiiKeerthy MoniNo ratings yet
- Automatic Coconut Dehusking MachineDocument12 pagesAutomatic Coconut Dehusking MachineKumaresh Salem0% (1)
- Research Paper Effect of Mobile Banking On Customer-823Document11 pagesResearch Paper Effect of Mobile Banking On Customer-823amittaneja28No ratings yet
- Nursing EnglishDocument139 pagesNursing EnglishSara Williams100% (3)
- MT4 EA Installation Guide Digital - EnglishDocument7 pagesMT4 EA Installation Guide Digital - EnglishThe Trading PitNo ratings yet
- CV Old NicDocument4 pagesCV Old NicTensonNo ratings yet
- Articles About Social Issues - Whiter SkinDocument9 pagesArticles About Social Issues - Whiter Skinf aNo ratings yet
- ATA212001Document3 pagesATA212001Tarek DeghedyNo ratings yet
- Moinho Disco PKM PDFDocument6 pagesMoinho Disco PKM PDFPaulo WilkerNo ratings yet
- Victaulic-FP-FireLock Fire-Pac Series 745 PreactionDocument9 pagesVictaulic-FP-FireLock Fire-Pac Series 745 PreactionTấn ĐạtNo ratings yet
- Grange Fencing Garden Products Brochure PDFDocument44 pagesGrange Fencing Garden Products Brochure PDFDan Joleys100% (1)
- Components of Vectors Prepared By: Victor Rea OribeDocument17 pagesComponents of Vectors Prepared By: Victor Rea OribeGerone Tolentino AtienzaNo ratings yet
- U04 Fxs of Humeral ShaftDocument88 pagesU04 Fxs of Humeral Shaftadrian_mogosNo ratings yet
- What On Earth Is A MainframeDocument132 pagesWhat On Earth Is A MainframeCarlos DantasNo ratings yet
- Rise of Al JazeeraDocument1 pageRise of Al Jazeeraইlish ProductionsNo ratings yet
- Selux Installation Manual PDFDocument75 pagesSelux Installation Manual PDFIgorr75% (8)
- Rotc Reviewer FinalsDocument11 pagesRotc Reviewer FinalsAngel Atienza100% (1)