You might also like
- Atlas of Coronary Intravascular Optical Coherence TomographyFrom EverandAtlas of Coronary Intravascular Optical Coherence TomographyNo ratings yet
- Acute Stroke AssessmentDocument7 pagesAcute Stroke AssessmentHanh NguyenNo ratings yet
- KJR 22 1964Document10 pagesKJR 22 1964melon segerNo ratings yet
- Correlates and Long Term Implication of Left Ventricular Mechanical Dispersion by Tqo Dimensional Speckle Tracking EchocardiographyDocument9 pagesCorrelates and Long Term Implication of Left Ventricular Mechanical Dispersion by Tqo Dimensional Speckle Tracking EchocardiographyMarco Antonio Viera ArevaloNo ratings yet
- 10.1007@s11936 020 0803 7Document17 pages10.1007@s11936 020 0803 7Paul CalbureanNo ratings yet
- 1 s2.0 S0914508719303648 MainDocument6 pages1 s2.0 S0914508719303648 MainMarina UlfaNo ratings yet
- Heart Blood Flow Simulation: A Perspective Review: Biomedical Engineering OnlineDocument28 pagesHeart Blood Flow Simulation: A Perspective Review: Biomedical Engineering Onlinemartin.dureux888No ratings yet
- Zhao 2018Document7 pagesZhao 2018Alexandru PusneiNo ratings yet
- Early Diagnosis of Intracranial Internal Carotid Artery Stenosis Using Extracranial Hemodynamic Indices From Carotid Doppler UltrasoundDocument13 pagesEarly Diagnosis of Intracranial Internal Carotid Artery Stenosis Using Extracranial Hemodynamic Indices From Carotid Doppler UltrasoundSamuelsonNo ratings yet
- Enfermedad MicrovascularDocument13 pagesEnfermedad MicrovascularWindar BaqueroNo ratings yet
- Detection and Localization of Coronary Arterial Lesion With The Aid of Impedance Cardiography and Artificial Neural NetworkDocument8 pagesDetection and Localization of Coronary Arterial Lesion With The Aid of Impedance Cardiography and Artificial Neural Networksudipta201988No ratings yet
- Imaging of Myocardial Fibrosis and ItsDocument9 pagesImaging of Myocardial Fibrosis and ItsGaal PinNo ratings yet
- Myocardial Work, An Echocardiographic Measure of Post Myocardial Infarct Scar On Contrast-Enhanced Cardiac Magnetic ResonanceDocument9 pagesMyocardial Work, An Echocardiographic Measure of Post Myocardial Infarct Scar On Contrast-Enhanced Cardiac Magnetic ResonanceHaribabuBabuNo ratings yet
- Jurnal 7Document10 pagesJurnal 7Zella ZakyaNo ratings yet
- Kondo Et Al 2022 Prognosis in Patients With Cardiogenic Shock Who Received Temporary Mechanical Circulatory SupportDocument13 pagesKondo Et Al 2022 Prognosis in Patients With Cardiogenic Shock Who Received Temporary Mechanical Circulatory Supporttegar ksatriaNo ratings yet
- Role of Exercise Treadmill Testing in The Assessment of Coronary Microvascular Disease - LopezDocument10 pagesRole of Exercise Treadmill Testing in The Assessment of Coronary Microvascular Disease - LopezM. PurnomoNo ratings yet
- Myocardial Contractile Dispersion: A New Marker For The Severity of Cirrhosis?Document5 pagesMyocardial Contractile Dispersion: A New Marker For The Severity of Cirrhosis?triNo ratings yet
- Association Between Systemic Inflammatory Response Index and Left Ventricular Remodeling and Systolic Dysfunction in Atrial Fibrillation PatientsDocument11 pagesAssociation Between Systemic Inflammatory Response Index and Left Ventricular Remodeling and Systolic Dysfunction in Atrial Fibrillation PatientsDr-Ashik RahmanNo ratings yet
- Pressure and Flow MeasurementsDocument25 pagesPressure and Flow Measurements윤원용No ratings yet
- Achim 2022Document8 pagesAchim 2022BözskeNo ratings yet
- Application of Strain and Other Echocardiographic Parameters in The Evaluation of Early and Long-Term Clinical Outcomes After Cardiac Surgery RevascularizationDocument8 pagesApplication of Strain and Other Echocardiographic Parameters in The Evaluation of Early and Long-Term Clinical Outcomes After Cardiac Surgery RevascularizationSondang JasmineNo ratings yet
- Active Versus Conventional Side Branch Protection Strategy For Coronary Bifurcation LesionsDocument8 pagesActive Versus Conventional Side Branch Protection Strategy For Coronary Bifurcation LesionsLuis Rafael Suárez U.No ratings yet
- Anterior Acute Myocardial Infarction Complicated With Ventricular Septal Rupture: Case Reports and Literature ReviewDocument5 pagesAnterior Acute Myocardial Infarction Complicated With Ventricular Septal Rupture: Case Reports and Literature ReviewIJAR JOURNALNo ratings yet
- De Baat 2021Document7 pagesDe Baat 2021Dhan RamadhanNo ratings yet
- J Jacc 2020 09 603Document12 pagesJ Jacc 2020 09 603Alejandro Alberto Garcia de la RochaNo ratings yet
- JCM 12 02274Document12 pagesJCM 12 02274Gaston HerediaNo ratings yet
- 1 s2.0 S073510971934553X MainDocument12 pages1 s2.0 S073510971934553X MainAlberto PolimeniNo ratings yet
- Assessment of Left Ventricular Function by EchocardiographyDocument15 pagesAssessment of Left Ventricular Function by EchocardiographyramangNo ratings yet
- 1 s2.0 S2590093522000224 MainDocument9 pages1 s2.0 S2590093522000224 MainSara TeixeiraNo ratings yet
- Acs 33 241Document9 pagesAcs 33 241Ratna AyieNo ratings yet
- Fmedt 04 748949Document12 pagesFmedt 04 748949Orlin ZlatarskiNo ratings yet
- Multimodality Cardiac Imaging of A Ventricular SepDocument4 pagesMultimodality Cardiac Imaging of A Ventricular SephengkileonardNo ratings yet
- Case Report Long Term Survival of Ventricular Septal Rupture (VSR) Closure Concomitant With CABG in Post-Acute Myocardial Infarction PatientDocument7 pagesCase Report Long Term Survival of Ventricular Septal Rupture (VSR) Closure Concomitant With CABG in Post-Acute Myocardial Infarction PatientDenny IntanNo ratings yet
- The Use of Fractional Flow Reserve (FFR) in Assessment of Residual IschemiaDocument10 pagesThe Use of Fractional Flow Reserve (FFR) in Assessment of Residual IschemiaM. PurnomoNo ratings yet
- Chronic Stable Coronary Artery Disease: Drugs vs. RevascularizationDocument16 pagesChronic Stable Coronary Artery Disease: Drugs vs. RevascularizationAndrea OrtizNo ratings yet
- Coronary Microvascular Disease Pathogenic Mechanisms and Therapeutic OptionsDocument17 pagesCoronary Microvascular Disease Pathogenic Mechanisms and Therapeutic OptionsZuleynny TellesNo ratings yet
- Transcranial Doppler: An Introduction For Primary Care PhysiciansDocument7 pagesTranscranial Doppler: An Introduction For Primary Care PhysiciansdediNo ratings yet
- Echocardiographic Assessment of Ischemic Mitral RegurgitationDocument16 pagesEchocardiographic Assessment of Ischemic Mitral RegurgitationNag Mallesh RaoNo ratings yet
- Characteristics of Coronary Artery Disease Among Patients With Atrial Fibrillation Compared To Patients With Sinus RhythmDocument9 pagesCharacteristics of Coronary Artery Disease Among Patients With Atrial Fibrillation Compared To Patients With Sinus RhythmFaisal AdamNo ratings yet
- Bhavanadhar 2018Document7 pagesBhavanadhar 2018Dr Suhail AkbarNo ratings yet
- Ehf2 7 2956Document6 pagesEhf2 7 2956Sebastian ChandraNo ratings yet
- s13089 022 00286 2Document11 pagess13089 022 00286 2Maudiel BrionesNo ratings yet
- WJCC 3 148Document9 pagesWJCC 3 148Sinisa RisticNo ratings yet
- TADocument7 pagesTAAngela Villanueva SocolaNo ratings yet
- Review ArticleDocument14 pagesReview ArticleBùi Ngọc Anh HSTCNo ratings yet
- Native t1 MappingDocument10 pagesNative t1 MappingRaiyanNo ratings yet
- Comparing The Adverse Clinical OutcomesDocument8 pagesComparing The Adverse Clinical Outcomes吴善统No ratings yet
- JCDD 08 00100 v2Document16 pagesJCDD 08 00100 v2Paulina ArteagaNo ratings yet
- RRC Art-1aqDocument12 pagesRRC Art-1aqCristi AlexandruNo ratings yet
- Atherosclerosis Phenotypes in 2023Document13 pagesAtherosclerosis Phenotypes in 2023Pedro SeguraNo ratings yet
- MidcabDocument7 pagesMidcabNs PadiludinNo ratings yet
- T1 Mapping and Feature Tracking Imaging of Left VeDocument12 pagesT1 Mapping and Feature Tracking Imaging of Left VeAlfian PramuditaNo ratings yet
- Diab 6Document6 pagesDiab 6marsim92No ratings yet
- Qader Othman 2019 J. Phys. Conf. Ser. 1294 062110Document11 pagesQader Othman 2019 J. Phys. Conf. Ser. 1294 062110GoranNo ratings yet
- Biomedicines 10 02407 v2Document13 pagesBiomedicines 10 02407 v2akinaNo ratings yet
- The Importance of Mean Platelet Volume To Lymphocyte Ratio in Predicting Atrial Fibrillation After Coronary Bypass OperationsDocument5 pagesThe Importance of Mean Platelet Volume To Lymphocyte Ratio in Predicting Atrial Fibrillation After Coronary Bypass OperationsM Ali AdrianNo ratings yet
- Application Zhong2018 PDFDocument17 pagesApplication Zhong2018 PDFHakan ENESNo ratings yet
- Computerized Medical Imaging and Graphics: Zhonghua Sun, Lei XuDocument13 pagesComputerized Medical Imaging and Graphics: Zhonghua Sun, Lei XuKain SmithNo ratings yet
- The Contribution of CMR To Patients Undergoing The PDFDocument14 pagesThe Contribution of CMR To Patients Undergoing The PDFTarigNo ratings yet
- Coronary 23716Document32 pagesCoronary 23716Luis David Sanchez MayoNo ratings yet
- Seiple HowtoChemdrawDocument3 pagesSeiple HowtoChemdrawabcdefNo ratings yet
- 1999/2000 Õa Keemiaolümpiaadi III Vooru Ülesannete LahendusedDocument2 pages1999/2000 Õa Keemiaolümpiaadi III Vooru Ülesannete LahendusedabcdefNo ratings yet
- Q Bernoulli Numbers and Q Bernoulli Polynomials RevisitedDocument8 pagesQ Bernoulli Numbers and Q Bernoulli Polynomials RevisitedabcdefNo ratings yet
- Determination and Metabolism of Dithiol Chelating AgentsDocument11 pagesDetermination and Metabolism of Dithiol Chelating AgentsabcdefNo ratings yet
- Ic 5018714Document10 pagesIc 5018714abcdefNo ratings yet
- Mock I Cho ProblemsDocument24 pagesMock I Cho ProblemsQuynh TranNo ratings yet
- The Chemistry Xenon': Chemistry Division, Argonne National Laboratory, Argonne, IllinoisDocument38 pagesThe Chemistry Xenon': Chemistry Division, Argonne National Laboratory, Argonne, IllinoisAlfa MenufanduNo ratings yet
- Acsomega 6b00506Document9 pagesAcsomega 6b00506abcdefNo ratings yet
- KjeldahlDocument1 pageKjeldahlabcdefNo ratings yet
- Theoretical Problems Solutions: Mock Icho 2021Document39 pagesTheoretical Problems Solutions: Mock Icho 2021abcdefNo ratings yet
- Solid-Supported Reagents For Organic SynthesisDocument13 pagesSolid-Supported Reagents For Organic SynthesisabcdefNo ratings yet
- Chromium Catalysts For Ethylene Polymerization and OligomerizationDocument65 pagesChromium Catalysts For Ethylene Polymerization and OligomerizationabcdefNo ratings yet
- Team Alpha Moo Mock Camp Test Theoretical Problems Exam 1Document26 pagesTeam Alpha Moo Mock Camp Test Theoretical Problems Exam 1abcdefNo ratings yet
- BCC 2019 OrgoDocument3 pagesBCC 2019 OrgoabcdefNo ratings yet
- Tcr,&Drcu Vol. 44, No. 2, Pp. 619 10 624, 1988 Riami Owoao20/88 S3.Oo+.AlDocument6 pagesTcr,&Drcu Vol. 44, No. 2, Pp. 619 10 624, 1988 Riami Owoao20/88 S3.Oo+.AlabcdefNo ratings yet
- Reducción de Azul de Metileno Por Acido AscorbicoDocument6 pagesReducción de Azul de Metileno Por Acido AscorbicoÁngelNo ratings yet
- Tcr,&Drcu Vol. 44, No. 2, Pp. 619 10 624, 1988 Riami Owoao20/88 S3.Oo+.AlDocument6 pagesTcr,&Drcu Vol. 44, No. 2, Pp. 619 10 624, 1988 Riami Owoao20/88 S3.Oo+.AlabcdefNo ratings yet
- Kinetics of Methylene Blue Reduction by Ascorbic Acid PDFDocument4 pagesKinetics of Methylene Blue Reduction by Ascorbic Acid PDFAndrés Felipe PerezNo ratings yet
- 0040 4039 (84) 80121 5Document4 pages0040 4039 (84) 80121 5abcdefNo ratings yet
- Multipurpose Experiments in Inorganic and Physical ChemistryDocument5 pagesMultipurpose Experiments in Inorganic and Physical ChemistryabcdefNo ratings yet
- s0040 4039 (00) 87545 0Document4 pagess0040 4039 (00) 87545 0abcdefNo ratings yet
- Reducción de Azul de Metileno Por Acido AscorbicoDocument6 pagesReducción de Azul de Metileno Por Acido AscorbicoÁngelNo ratings yet
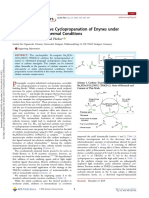
- Fe-Catalyzed Selective Cyclopropanation of Enynes Under Photochemical or Thermal ConditionsDocument5 pagesFe-Catalyzed Selective Cyclopropanation of Enynes Under Photochemical or Thermal ConditionsabcdefNo ratings yet
- Another DistanceDocument3 pagesAnother DistanceabcdefNo ratings yet
- Acsomega 6b00506Document9 pagesAcsomega 6b00506abcdefNo ratings yet
- Acsomega 6b00506Document9 pagesAcsomega 6b00506abcdefNo ratings yet
- Enantioselective Synthesis of Fused Polycyclic Tropanes Via Dearomative (3 + 2) Cycloaddition Reactions of 2 NitrobenzofuransDocument4 pagesEnantioselective Synthesis of Fused Polycyclic Tropanes Via Dearomative (3 + 2) Cycloaddition Reactions of 2 NitrobenzofuransabcdefNo ratings yet
- Computational Transition-State Design Provides Experimentally Verified CR (P, N) Catalysts For Control of Ethylene Trimerization and TetramerizationDocument6 pagesComputational Transition-State Design Provides Experimentally Verified CR (P, N) Catalysts For Control of Ethylene Trimerization and TetramerizationabcdefNo ratings yet
- Imidazolylidene Cu (II) Complexes: Synthesis Using Imidazolium Carboxylate Precursors and Structure Rearrangement PathwaysDocument12 pagesImidazolylidene Cu (II) Complexes: Synthesis Using Imidazolium Carboxylate Precursors and Structure Rearrangement PathwaysabcdefNo ratings yet
- Protective Effect of Hydroxytyrosol Against Cardiac Remodeling After Isoproterenol-Induced Myocardial Infarction in RatDocument12 pagesProtective Effect of Hydroxytyrosol Against Cardiac Remodeling After Isoproterenol-Induced Myocardial Infarction in RatMba DghisNo ratings yet
- Writing A Simulation Scenario: A Step-By-Step Guide: Deborah Bambini, PHD, WHNP-BC, Cne, ChseDocument10 pagesWriting A Simulation Scenario: A Step-By-Step Guide: Deborah Bambini, PHD, WHNP-BC, Cne, ChseEsteban RamosNo ratings yet
- Drug Infusions in ICU Made Simple 2016Document28 pagesDrug Infusions in ICU Made Simple 2016ta lê thanhNo ratings yet
- Efficacy and Safety o A Dedicated LAAO Protocol 2022Document3 pagesEfficacy and Safety o A Dedicated LAAO Protocol 2022吳醫師No ratings yet
- 06 - HSE Alert Emergency Response - Electrical IncidentDocument2 pages06 - HSE Alert Emergency Response - Electrical Incidentmohammad_shahzad_iiuiNo ratings yet
- Lets Talk SafetyDocument139 pagesLets Talk SafetymineprincessNo ratings yet
- Medical Aspects of Fitness For Work Offshore - Guidance For Examining PhysiciansDocument80 pagesMedical Aspects of Fitness For Work Offshore - Guidance For Examining PhysiciansJamie Taylor100% (6)
- Omron Blood Pressure Monitor Hem-7203 Instruction ManualDocument1 pageOmron Blood Pressure Monitor Hem-7203 Instruction Manualpriyod_chandran50% (2)
- HRV - Handbook of Clinical NeurologyDocument15 pagesHRV - Handbook of Clinical NeurologyGonçalo MirandaNo ratings yet
- Bremshey Cardio Control Exercise BikeDocument64 pagesBremshey Cardio Control Exercise BikeStuart McAleeseNo ratings yet
- Damage Control ResuscitationDocument32 pagesDamage Control Resuscitationrima oktariniNo ratings yet
- Imaging of Central Nervous System Ischemia.6Document19 pagesImaging of Central Nervous System Ischemia.6Gabriela ArvelaezNo ratings yet
- ResPlus B 30P BiPAP User ManualDocument35 pagesResPlus B 30P BiPAP User ManualVikasNo ratings yet
- Ventricular Isovolumetric Contractions: Tiara Calvo Leon, M.DDocument1 pageVentricular Isovolumetric Contractions: Tiara Calvo Leon, M.DSarah KhanNo ratings yet
- Interventional Cardiology ImagingDocument255 pagesInterventional Cardiology ImagingArtur TarsaNo ratings yet
- Eacvi Handbook of Cardiovascular CT Oliver Gaemperli Full ChapterDocument67 pagesEacvi Handbook of Cardiovascular CT Oliver Gaemperli Full Chaptermilton.alvarado146100% (7)
- Stop-Acei Trial Journal ClubDocument3 pagesStop-Acei Trial Journal Clubapi-648891519No ratings yet
- Basic Electrocardiography NewDocument25 pagesBasic Electrocardiography NewMoh Arif KurniawanNo ratings yet
- First Grading VIDocument82 pagesFirst Grading VIIvy Villanueva Divino100% (1)
- Heart BlockDocument17 pagesHeart Blocklitan dasNo ratings yet
- DOWLEX™ 2038.68G: Polyethylene ResinDocument3 pagesDOWLEX™ 2038.68G: Polyethylene ResinJosé PalmaNo ratings yet
- Chapter 11 Adaptations To Aeribic and Anaerobic TrainingDocument26 pagesChapter 11 Adaptations To Aeribic and Anaerobic Trainingshahbaz AkhtarNo ratings yet
- Milrinone NeomedDocument4 pagesMilrinone NeomedmuarifNo ratings yet
- Vital Signs Procedure ChecklistDocument10 pagesVital Signs Procedure Checklistako at ang exoNo ratings yet
- Kami Export - CirculatorySystem12052022Document1 pageKami Export - CirculatorySystem12052022Nyla ScottNo ratings yet
- Heart AttackDocument4 pagesHeart AttackMirella Lereleré100% (1)
- Journal ClubDocument3 pagesJournal ClubAmreen RahmanNo ratings yet
- Ecg Made EasyDocument45 pagesEcg Made EasyVinoth Kumar RaviNo ratings yet
- PJB Pada Dewasa AASDocument54 pagesPJB Pada Dewasa AAS1e23e2ewNo ratings yet
- Cost Analysis of Cath Lab Procedures Done at A Tertiary Care Hospital of North IndiaDocument9 pagesCost Analysis of Cath Lab Procedures Done at A Tertiary Care Hospital of North IndiaIJAR JOURNALNo ratings yet