0% found this document useful (0 votes)
541 views1 pageReferral Letter
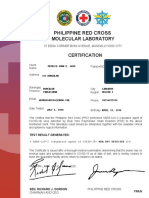
The referral letter refers an individual for a RT-PCR test at Tomboc - Salayog Hospital and advises home quarantine for a specified number of days. It was issued at the request of an unnamed person for an unspecified purpose other than for legal medical purposes. The letter is signed by the Medical Officer III of the Department of Education of the City Schools Division of Tacurong.
Uploaded by
Sugar CanibanCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
541 views1 pageReferral Letter
The referral letter refers an individual for a RT-PCR test at Tomboc - Salayog Hospital and advises home quarantine for a specified number of days. It was issued at the request of an unnamed person for an unspecified purpose other than for legal medical purposes. The letter is signed by the Medical Officer III of the Department of Education of the City Schools Division of Tacurong.
Uploaded by
Sugar CanibanCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd