You might also like
- Probability and Statistical Inference-CRC (2021)Document444 pagesProbability and Statistical Inference-CRC (2021)chanmanhcuong509100% (2)
- Drug Discovery and ProcessDocument12 pagesDrug Discovery and ProcessLinda DikeNo ratings yet
- Step-by-Step Guide to Creating a Conceptual FrameworkDocument3 pagesStep-by-Step Guide to Creating a Conceptual FrameworkMichelle Caliuag100% (1)
- Clinical Research MethodologyDocument11 pagesClinical Research MethodologymisganaNo ratings yet
- Bioequivalence Requirements in Various Global Jurisdictions-Springer International Publishing (2017)Document348 pagesBioequivalence Requirements in Various Global Jurisdictions-Springer International Publishing (2017)Solomon100% (1)
- Final Project LevofloxacinDocument102 pagesFinal Project LevofloxacinJalwaz TihamiNo ratings yet
- Fatigue Testing in Socket WeldsDocument31 pagesFatigue Testing in Socket WeldsAndres_Pastor1987100% (1)
- Clinical Trial Gadavala SarahDocument60 pagesClinical Trial Gadavala SarahSejal khuman100% (1)
- NASA's Manned Space Flight ProgramDocument127 pagesNASA's Manned Space Flight ProgramBob AndrepontNo ratings yet
- Guidance For Conducting Clinical Trials Based On Drugs Medical Products Good Clinical PracticeDocument44 pagesGuidance For Conducting Clinical Trials Based On Drugs Medical Products Good Clinical PracticeMostafa SalahNo ratings yet
- Scientific Insights: ICH S6 (R1) - Preclinical Safety of BiopharmaceuticalsDocument4 pagesScientific Insights: ICH S6 (R1) - Preclinical Safety of BiopharmaceuticalsHuntingdon Life Sciences100% (1)
- Weight Variation of BiscuitsDocument12 pagesWeight Variation of BiscuitsSandeep Haridas MNo ratings yet
- ICH-Guidelines SummaryDocument34 pagesICH-Guidelines SummarySamiksha More100% (1)
- Bioanalysis NotesDocument7 pagesBioanalysis NoteskeerthiNo ratings yet
- BOSCH7Document14 pagesBOSCH7Georgiana BusuiocNo ratings yet
- Understanding O.D: Dr. Nitika SharmaDocument59 pagesUnderstanding O.D: Dr. Nitika SharmaSalim KhanNo ratings yet
- Regulatory Perspective on Bioequivalence StudiesDocument12 pagesRegulatory Perspective on Bioequivalence Studiesbhanu99100% (2)
- An Approach For Developing Concept of Innovation Readiness LevelsDocument20 pagesAn Approach For Developing Concept of Innovation Readiness LevelsijmitNo ratings yet
- Lesson Plan CritiqueDocument3 pagesLesson Plan Critiqueapi-357257220No ratings yet
- Formulation of Monoclonal Antibody Therapies: From Lab to MarketFrom EverandFormulation of Monoclonal Antibody Therapies: From Lab to MarketNo ratings yet
- AHCC: The Medical Breakthrough in Natural ImmunotherapyFrom EverandAHCC: The Medical Breakthrough in Natural ImmunotherapyRating: 5 out of 5 stars5/5 (1)
- Bioequivalence of Generic and Branded Amoxicillin Capsules in Healthy Human VolunteersDocument6 pagesBioequivalence of Generic and Branded Amoxicillin Capsules in Healthy Human VolunteersAkhmad NgafifNo ratings yet
- Article Wjpps 1530096800Document12 pagesArticle Wjpps 1530096800bk regulatoryNo ratings yet
- Jurnal 2 AceclofenacDocument11 pagesJurnal 2 AceclofenacRossana Rizqita PutriNo ratings yet
- Albendazole, Mebendazole and Praziquantel. Review of Non-Clinical Toxicity and PharmacokineticsDocument19 pagesAlbendazole, Mebendazole and Praziquantel. Review of Non-Clinical Toxicity and PharmacokineticsGianmarcoSugarAventureroNo ratings yet
- Q.C in YemenDocument6 pagesQ.C in YemenWafa BadullaNo ratings yet
- AmlodipinebesylatepaperDocument6 pagesAmlodipinebesylatepaperRakesh RauniyarNo ratings yet
- Jurnal Summary 1 H6Document13 pagesJurnal Summary 1 H6Novianto Meska PratamaNo ratings yet
- Innovative in Vitro Methodologies For Establishing Therapeutic EquivalenceDocument6 pagesInnovative in Vitro Methodologies For Establishing Therapeutic EquivalenceAnonymous 6OPLC9UNo ratings yet
- Tipuri de Efect PKDocument11 pagesTipuri de Efect PKLaiosAndreaNo ratings yet
- Huizhe Wu, MD Mingyan Liu, MD Shuang Wang, MD Wanyu Feng, MD, PHD Weifan Yao, Bs Haishan Zhao, Bs and Minjie Wei, MD, PHDDocument10 pagesHuizhe Wu, MD Mingyan Liu, MD Shuang Wang, MD Wanyu Feng, MD, PHD Weifan Yao, Bs Haishan Zhao, Bs and Minjie Wei, MD, PHDDyva VanillaNo ratings yet
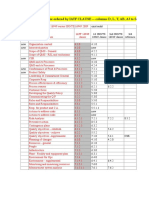
- Table of Content and Abstract on Pharmaceutical Product QualityDocument40 pagesTable of Content and Abstract on Pharmaceutical Product QualityAyush KesriNo ratings yet
- BiosimilarsDocument3 pagesBiosimilarsDr.Nalini PavuluriNo ratings yet
- IND Ashwani GoyalDocument16 pagesIND Ashwani Goyalashpharma007No ratings yet
- Clinical Pharmacokinetic Studies of PharmaceuticalsDocument23 pagesClinical Pharmacokinetic Studies of PharmaceuticalsPankaj SharmaNo ratings yet
- Pharmacopolitics, Implications and Implementation in Clinical StudiesDocument3 pagesPharmacopolitics, Implications and Implementation in Clinical StudiesNantarat KengkeatchaiNo ratings yet
- Admin,+Journal+Manager,+12 AJPCR 40 31720Document3 pagesAdmin,+Journal+Manager,+12 AJPCR 40 31720Komal RaneNo ratings yet
- Pharmacokinetic Study of Amoxicillin Capsule in HeDocument8 pagesPharmacokinetic Study of Amoxicillin Capsule in Hebk regulatoryNo ratings yet
- Safety Testing of PharmaceuticalsDocument39 pagesSafety Testing of PharmaceuticalsSaikumar RoithNo ratings yet
- Individual Assignment 1Document6 pagesIndividual Assignment 1Che InopiaNo ratings yet
- Chicken 7Document10 pagesChicken 7Mary VegaNo ratings yet
- Article On BA&BEDocument7 pagesArticle On BA&BENitin DhimanNo ratings yet
- Preclinical Development - WikipediaDocument13 pagesPreclinical Development - WikipediaMukta fuleNo ratings yet
- AducanumabDocument9 pagesAducanumabMamta PooniaNo ratings yet
- 2013 PavaniDocument11 pages2013 PavaniGopal KrishnaNo ratings yet
- Regulatory Requirements For The Product Approval of BiologicsDocument14 pagesRegulatory Requirements For The Product Approval of BiologicsSurround TechsNo ratings yet
- Approval & Development: DrugsDocument11 pagesApproval & Development: DrugsOmar SalehNo ratings yet
- Bcs Classification of DrugsDocument12 pagesBcs Classification of Drugsjigarpatel5No ratings yet
- Losartan Fda Bioequivalence RecenteDocument6 pagesLosartan Fda Bioequivalence Recentelamouna.lamittaNo ratings yet
- 2 Amrutaobjectivesandconsiderationsinbioavailabilitystudy 130211000517 Phpapp01 PDFDocument31 pages2 Amrutaobjectivesandconsiderationsinbioavailabilitystudy 130211000517 Phpapp01 PDFsaurabh chaturvediNo ratings yet
- Gen Pharmacology Intro BDSDocument23 pagesGen Pharmacology Intro BDSDr.U.P.Rathnakar.MD.DIH.PGDHMNo ratings yet
- Clinical Pharmacology Answers 2022Document223 pagesClinical Pharmacology Answers 2022nancy voraNo ratings yet
- Pharmacotherapeutics-CH-1-Pharmacotherapeutics-NotesDocument9 pagesPharmacotherapeutics-CH-1-Pharmacotherapeutics-Notesmaharachandana18No ratings yet
- Daniel Wood Christopher Gregory: Understanding GenericsDocument9 pagesDaniel Wood Christopher Gregory: Understanding Genericsniravpharma21No ratings yet
- Drug DevelopmentDocument19 pagesDrug DevelopmentFaye PoncianoNo ratings yet
- Comparative Bioavailability Study of Phenytoin inDocument4 pagesComparative Bioavailability Study of Phenytoin inHuydiNo ratings yet
- V37-4 Art 3 pp186-193Document8 pagesV37-4 Art 3 pp186-193wikka94No ratings yet
- Beliefs and Attitudes of Generic Versus Original Drugs Among Doctors in A Tertiary-Care Hospital in Western IndiaDocument6 pagesBeliefs and Attitudes of Generic Versus Original Drugs Among Doctors in A Tertiary-Care Hospital in Western IndiaHavarbaniNo ratings yet
- Microbial Contamination of Nonsterile Pharmaceuticals in Public Hospital SettingsDocument8 pagesMicrobial Contamination of Nonsterile Pharmaceuticals in Public Hospital SettingsOghenekome Ereromebe AkpogumeNo ratings yet
- Craneetal 2019Document16 pagesCraneetal 2019บอส เลิศเกียรติรัชตะNo ratings yet
- Agnes PDFDocument18 pagesAgnes PDFTanzilla EvitasariNo ratings yet
- Pharmaco Vigilance of ASU Drugs:an Over View of Current Status, Challenges and SolutionsDocument55 pagesPharmaco Vigilance of ASU Drugs:an Over View of Current Status, Challenges and Solutionssuhas M100% (1)
- Monoclonal Antibodies A Review of Therapeutic ApplDocument11 pagesMonoclonal Antibodies A Review of Therapeutic ApplThanasisNo ratings yet
- Drug Use in Ophthalmology Out-Patient Department: A Prospective Study at A Tertiary Care Teaching HospitalDocument6 pagesDrug Use in Ophthalmology Out-Patient Department: A Prospective Study at A Tertiary Care Teaching HospitalHania AwadNo ratings yet
- Psychotropic DrugDocument10 pagesPsychotropic DrugAlexandra Elizabeth FloresNo ratings yet
- 2022 - Sun - Why 90% of Clinical Drug Development Fails and How To Improve ItDocument14 pages2022 - Sun - Why 90% of Clinical Drug Development Fails and How To Improve ItMohammed BaassiriNo ratings yet
- Pharmacy Orientation PPP211: Introduction To The Pharmacy Profession and The Future of The PharmacistDocument27 pagesPharmacy Orientation PPP211: Introduction To The Pharmacy Profession and The Future of The PharmacistJape GarridoNo ratings yet
- Pharmacological Impact of Edible Macrofungi D. Spathularia and S. Commune On Hematological Profile of Albino RatDocument7 pagesPharmacological Impact of Edible Macrofungi D. Spathularia and S. Commune On Hematological Profile of Albino RatIJAR JOURNALNo ratings yet
- Biowaiver for Aciclovir TabletsDocument13 pagesBiowaiver for Aciclovir TabletsRian Nurdiana100% (1)
- Pharmacokinetic Study of Amoxicillin Capsule in HeDocument8 pagesPharmacokinetic Study of Amoxicillin Capsule in Hebk regulatoryNo ratings yet
- Amoxacillin 2Document7 pagesAmoxacillin 2bk regulatoryNo ratings yet
- Amoxicillin WESASDocument14 pagesAmoxicillin WESASbk regulatoryNo ratings yet
- Comparative in Vitro Quality Evaluationof Different Brandsof Mebendazole TabletsDocument5 pagesComparative in Vitro Quality Evaluationof Different Brandsof Mebendazole Tabletsbk regulatoryNo ratings yet
- Zovirax Tablets PIDocument10 pagesZovirax Tablets PIbk regulatoryNo ratings yet
- Lido, Pril CRM IE S 5% Sep2017 v1Document16 pagesLido, Pril CRM IE S 5% Sep2017 v1bk regulatoryNo ratings yet
- 27 Vol. 2 Issue 12 RA 948 2011 Paper 27Document9 pages27 Vol. 2 Issue 12 RA 948 2011 Paper 27bk regulatoryNo ratings yet
- Tropical Med Int Health - 2005 - Boeree - Efficacy and Safety of Two Dosages of Cotrimoxazole As Preventive Treatment ForDocument11 pagesTropical Med Int Health - 2005 - Boeree - Efficacy and Safety of Two Dosages of Cotrimoxazole As Preventive Treatment Forbk regulatoryNo ratings yet
- Impact of Modernization On FamDocument6 pagesImpact of Modernization On FamReza Gokal100% (1)
- Psa Activity and Questions Sheet: Step 1: Thinking About PsasDocument2 pagesPsa Activity and Questions Sheet: Step 1: Thinking About PsasanibeliNo ratings yet
- CCPDocument65 pagesCCPnaveeth11No ratings yet
- MSc Economics Course Structure & SyllabusDocument41 pagesMSc Economics Course Structure & SyllabusSiddarth RamanNo ratings yet
- Analytical DesignDocument38 pagesAnalytical Designsawyl AHAMEFULA MBANo ratings yet
- BBS57 EPGE Study Guide Rodney Sim V3-1Document41 pagesBBS57 EPGE Study Guide Rodney Sim V3-1Allana NacinoNo ratings yet
- Preparing Children To Solve ProblemsDocument31 pagesPreparing Children To Solve ProblemsJennylyn Layan AlnajesNo ratings yet
- Online Glossary For Ap Psychology WeeblyDocument52 pagesOnline Glossary For Ap Psychology Weeblyapi-276687593No ratings yet
- Example 10 Test of HypothesisDocument3 pagesExample 10 Test of HypothesisPorosh Uddin Ahmed TaposhNo ratings yet
- Impact of Science & Tech on SocietyDocument7 pagesImpact of Science & Tech on SocietyshielaNo ratings yet
- Report Writing Guide: 10 Easy StepsDocument19 pagesReport Writing Guide: 10 Easy StepsAhmad ButtNo ratings yet
- Aleza Menorca COMPILATION Module - Industrial Organizational Psychology FinalDocument80 pagesAleza Menorca COMPILATION Module - Industrial Organizational Psychology FinalALEZA MENORCANo ratings yet
- Legal Internship Resume - Sample 1: Sachin XXXXXXDocument4 pagesLegal Internship Resume - Sample 1: Sachin XXXXXXshivani soniNo ratings yet
- Appleton & Lange Review of Anatomy, Sixth Edition: NoticeDocument1 pageAppleton & Lange Review of Anatomy, Sixth Edition: NoticeSomiZafarNo ratings yet
- Juki Sweing Machine ProjectDocument61 pagesJuki Sweing Machine ProjectApple ComputersNo ratings yet
- Man Power Planning Jyoti DubeyDocument95 pagesMan Power Planning Jyoti DubeydhruvNo ratings yet
- Acfrogax921n5vuh0aokftspbcs5bfratl Eskijgvqo Txz4l5mlvtiumiv37iyxdd Sewetasvwgkaw8rcoovd7ke Te6o9nokz5nk7crfg3gtg9riefsewuxhtruylgtknfbuqgda2e9u2veDocument49 pagesAcfrogax921n5vuh0aokftspbcs5bfratl Eskijgvqo Txz4l5mlvtiumiv37iyxdd Sewetasvwgkaw8rcoovd7ke Te6o9nokz5nk7crfg3gtg9riefsewuxhtruylgtknfbuqgda2e9u2veCecilia FauquieNo ratings yet
- Chapter 1Document4 pagesChapter 1Jayshri ThakurNo ratings yet
- Ra 6975 - Dilg Act of 1990Document28 pagesRa 6975 - Dilg Act of 1990tristanmunar100% (1)
- OSH AuditDocument44 pagesOSH Auditsdtseurdiu8f9No ratings yet
- Issues in Financial Reporting Izza Urooj Sap Id 6884 Sir AmanullahDocument11 pagesIssues in Financial Reporting Izza Urooj Sap Id 6884 Sir AmanullahAli AwanNo ratings yet