You might also like
- Self Measures For Love and Compassion Research General Relationship SatisfactionDocument13 pagesSelf Measures For Love and Compassion Research General Relationship SatisfactionQasim AliNo ratings yet
- Assessment of Family Violence - A Handbook For Researchers and Practitioners (2002)Document563 pagesAssessment of Family Violence - A Handbook For Researchers and Practitioners (2002)Erica Oliveira100% (1)
- An Introduction To Theories of Personality 5th Edition by Robert B EwenDocument6 pagesAn Introduction To Theories of Personality 5th Edition by Robert B EwenBaby Glorypath0% (1)
- DSM-5 and Culture - The Need To Move Towards A Shared Model of Care Within A More Equal Patient-Physician PartnershipDocument3 pagesDSM-5 and Culture - The Need To Move Towards A Shared Model of Care Within A More Equal Patient-Physician PartnershipPearl SkyNo ratings yet
- Conners2011 PDFDocument297 pagesConners2011 PDFCristinaNo ratings yet
- Essentials of Neuropsychological Assessment 2ndDocument4 pagesEssentials of Neuropsychological Assessment 2ndRodrigo Caron0% (2)
- Global Assessment FunctioningDocument8 pagesGlobal Assessment Functioningapi-260339450No ratings yet
- Psychological Basis of School PsychologyDocument27 pagesPsychological Basis of School PsychologyVivek RamachandranNo ratings yet
- QS: Social Exchange Theory: FoundersDocument2 pagesQS: Social Exchange Theory: FounderssoulxpressNo ratings yet
- Zech - Alexithymia and Its Measurement Confirmatory Factor Analyses of The Twenty-Item Toronto Alexithymia ScaleDocument38 pagesZech - Alexithymia and Its Measurement Confirmatory Factor Analyses of The Twenty-Item Toronto Alexithymia ScaleGUSREYES69No ratings yet
- Y Bocs Information SampleDocument2 pagesY Bocs Information SampledevNo ratings yet
- Mechanisms of Change in Prolonged Exposure Therapy For PTSD-Implications For Clinical PracticeDocument9 pagesMechanisms of Change in Prolonged Exposure Therapy For PTSD-Implications For Clinical PracticeKelly GCNo ratings yet
- APA DSM 5 Paraphilic DisordersDocument2 pagesAPA DSM 5 Paraphilic DisordersAli FenNo ratings yet
- Psychosocial Dimensions of Displacement: Prevalence of Mental Health Outcomes and Related Stressors Among Idps in IraqDocument34 pagesPsychosocial Dimensions of Displacement: Prevalence of Mental Health Outcomes and Related Stressors Among Idps in IraqSocial InquiryNo ratings yet
- Men, Suicide and SocietyDocument155 pagesMen, Suicide and Societytimaza100% (2)
- Parent Child Bed SharingDocument24 pagesParent Child Bed SharingquinhoxNo ratings yet
- SAS 7 CRI 188 Therapeutic ModalitiesDocument9 pagesSAS 7 CRI 188 Therapeutic ModalitiesKaren Angel AbaoNo ratings yet
- 2001 - Schizophrenia in Children and Adolescents - RemschmidtDocument322 pages2001 - Schizophrenia in Children and Adolescents - RemschmidtvdenkerNo ratings yet
- Whats in The Name AlexithymiaDocument15 pagesWhats in The Name AlexithymiathebeholderNo ratings yet
- KIDDIE Formal Thought Disorder - Caplan1989Document9 pagesKIDDIE Formal Thought Disorder - Caplan1989Rafael MartinsNo ratings yet
- Clinical Intake SummaryDocument9 pagesClinical Intake Summaryvaz21No ratings yet
- Experimental Manipulations of Self-Affirmation REVIEW PDFDocument67 pagesExperimental Manipulations of Self-Affirmation REVIEW PDFAlex RichieNo ratings yet
- Clinical Interview: January 2015Document10 pagesClinical Interview: January 2015KAROL GUISELL PATIÑO ATEHORTUANo ratings yet
- 1 Clinical InterviewDocument14 pages1 Clinical InterviewClara Del Castillo ParísNo ratings yet
- Mueller Segal 2015Document7 pagesMueller Segal 2015Mónica RibeiroNo ratings yet
- Understanding The Assessment of Clinical Reasoning: Omar S. LaynesaDocument20 pagesUnderstanding The Assessment of Clinical Reasoning: Omar S. Laynesaomar laynesaNo ratings yet
- Lesson 1 Clinical PsychologyDocument7 pagesLesson 1 Clinical PsychologyTin EupenaNo ratings yet
- What Is Clinical Psychology?: DefinitionsDocument15 pagesWhat Is Clinical Psychology?: DefinitionsJay Mark CabreraNo ratings yet
- Self CompassionDocument2 pagesSelf CompassionMUSYOKA KITUKUNo ratings yet
- Clinical Psychology at WorkDocument22 pagesClinical Psychology at WorkMark Kenneth NicartNo ratings yet
- Clinical Pre Finals Chapter 11-15Document49 pagesClinical Pre Finals Chapter 11-15justfunkyou1No ratings yet
- Interview Method in AssessmentDocument13 pagesInterview Method in AssessmentAnanya100% (2)
- Research On Psychotherapy Efficacy and EffectivenessDocument18 pagesResearch On Psychotherapy Efficacy and EffectivenesspsicandreiaNo ratings yet
- Getting The Most Out of The Clinical Encounter: The Four Habits ModelDocument10 pagesGetting The Most Out of The Clinical Encounter: The Four Habits Modelliao01No ratings yet
- Clinical Reasoning: Linking Theory To Practice and Practice To TheoryDocument14 pagesClinical Reasoning: Linking Theory To Practice and Practice To Theorylumac1087831No ratings yet
- Clinical Reasoning in Manual TherapyDocument11 pagesClinical Reasoning in Manual TherapyKhushboo PakhraniNo ratings yet
- Clinical Psychology Notes No. 1Document2 pagesClinical Psychology Notes No. 1Jerine Bonus ApostolNo ratings yet
- Clinical Assessment Psychodiagnostic Decision MakingDocument158 pagesClinical Assessment Psychodiagnostic Decision MakingKilana LichterfeldNo ratings yet
- Introduction To Clinical AssessmentDocument13 pagesIntroduction To Clinical AssessmentnurmeenNo ratings yet
- Unit-1 Unit-3 PsychodiadnosisDocument18 pagesUnit-1 Unit-3 PsychodiadnosisOmi PreetamNo ratings yet
- Training Professionals in Motivational InterviewingDocument38 pagesTraining Professionals in Motivational InterviewingMdEssaNo ratings yet
- Van Scoyoc, S. (2017) - The Use and Misuse of Psychometrics in Clinical Settings. in B. Cripps (Ed.)Document17 pagesVan Scoyoc, S. (2017) - The Use and Misuse of Psychometrics in Clinical Settings. in B. Cripps (Ed.)susanvanscoyoc9870No ratings yet
- Documentary of ExplanationDocument17 pagesDocumentary of ExplanationMuhammad Hamza AshfaqNo ratings yet
- Critical Thinking in NursingDocument37 pagesCritical Thinking in NursingAmmar Zaki NabilaNo ratings yet
- Clinical Reasoning in Psychosocial Occupational Therapy - The Evaluation Process. Barris1987Document16 pagesClinical Reasoning in Psychosocial Occupational Therapy - The Evaluation Process. Barris1987saraNo ratings yet
- Approaches To LearningDocument10 pagesApproaches To LearningBulan KakanitaNo ratings yet
- Clinical Assessment - TahiraDocument72 pagesClinical Assessment - TahiraVaneeza AliNo ratings yet
- Understanding and Evaluating QualitativeDocument16 pagesUnderstanding and Evaluating QualitativeSubashni VeeramuthuNo ratings yet
- Mental HealthDocument11 pagesMental Healthmahmoodosman91No ratings yet
- Clinical Assessment Referral, Components, and PurposeDocument53 pagesClinical Assessment Referral, Components, and PurposeBrinda ChughNo ratings yet
- A Scientific Approach To Your Research: Sample Chapter From Conducting Your Pharmacy Practice Research ProjectDocument18 pagesA Scientific Approach To Your Research: Sample Chapter From Conducting Your Pharmacy Practice Research ProjectKrisel IbanezNo ratings yet
- Qualitative Research-Critical Appraisal A Qualitative Study Experiences of Stigma by People With Mental Health ProblemsDocument16 pagesQualitative Research-Critical Appraisal A Qualitative Study Experiences of Stigma by People With Mental Health Problemscaleb mwanziaNo ratings yet
- Clinical ReasoningDocument23 pagesClinical Reasoningathe_triiaNo ratings yet
- What Is Mental Health? Evidence Towards A New Definition From A Mixed Methods Multidisciplinary International SurveyDocument11 pagesWhat Is Mental Health? Evidence Towards A New Definition From A Mixed Methods Multidisciplinary International SurveyBRENNETH CANIBELNo ratings yet
- Case Formulation in PsychotherapyDocument5 pagesCase Formulation in PsychotherapySimona MoscuNo ratings yet
- Clinical Interview PhasesDocument5 pagesClinical Interview Phasesmomina sarwarNo ratings yet
- Tests SsDocument14 pagesTests SsjvtoselaNo ratings yet
- Conducting 2e SampleDocument18 pagesConducting 2e SampleIbn Hamz El-SalamyNo ratings yet
- Assessment of Clinical Reasoning Three EvolutionsDocument6 pagesAssessment of Clinical Reasoning Three EvolutionsFrederico PóvoaNo ratings yet
- Getting The Most Out of The Clinical Encounter: The Four Habits ModelDocument11 pagesGetting The Most Out of The Clinical Encounter: The Four Habits ModelFacu YaneNo ratings yet
- Case Study - IPT For DepressionDocument13 pagesCase Study - IPT For DepressionIsaac FullartonNo ratings yet
- Prevalence and Correlates of Suicide Planning and Attempt Among Individuals With SIDocument8 pagesPrevalence and Correlates of Suicide Planning and Attempt Among Individuals With SIIsaac FullartonNo ratings yet
- Psychologistsas Expert Witnessesin Australian CourtroomsDocument10 pagesPsychologistsas Expert Witnessesin Australian CourtroomsIsaac FullartonNo ratings yet
- Clinical Considerations for a Strength-Based Intake AssessmentDocument12 pagesClinical Considerations for a Strength-Based Intake AssessmentIsaac FullartonNo ratings yet
- Allan 2006 Prediction of The Risk of Male SexuDocument10 pagesAllan 2006 Prediction of The Risk of Male SexuIsaac FullartonNo ratings yet
- 22 Psychol Pub Poly L427Document13 pages22 Psychol Pub Poly L427Isaac FullartonNo ratings yet
- Using family systems, migration histories and acculturation in CBT assessmentDocument21 pagesUsing family systems, migration histories and acculturation in CBT assessmentIsaac FullartonNo ratings yet
- W1 - Why Therapists Should Walk The TalkDocument13 pagesW1 - Why Therapists Should Walk The TalkIsaac FullartonNo ratings yet
- The Mental Status ExaminationDocument7 pagesThe Mental Status Examinationdra.hadleyNo ratings yet
- Vuoskoski Eerola 2011 Music Pers Mood EmotpercDocument8 pagesVuoskoski Eerola 2011 Music Pers Mood EmotpercIsaac FullartonNo ratings yet
- Understanding School Shootings With Crime Script AnalysisDocument14 pagesUnderstanding School Shootings With Crime Script AnalysisIsaac FullartonNo ratings yet
- Depression and Anxiety in High-Achieving Researcher due to Childhood TraumaDocument2 pagesDepression and Anxiety in High-Achieving Researcher due to Childhood TraumaIsaac FullartonNo ratings yet
- The State of Mentoring - Change Agents ReportDocument31 pagesThe State of Mentoring - Change Agents ReportIsaac FullartonNo ratings yet
- Stimulus Set 2Document3 pagesStimulus Set 2Isaac FullartonNo ratings yet
- The Effect of Exercise on Episodic Memory in Individuals With and Without SCDDocument60 pagesThe Effect of Exercise on Episodic Memory in Individuals With and Without SCDIsaac FullartonNo ratings yet
- HUMSS - DIASS12-Ia-1 Aug.24Document3 pagesHUMSS - DIASS12-Ia-1 Aug.24Sharon DannugNo ratings yet
- Critical Reading StrategiesDocument3 pagesCritical Reading StrategiesJoash Charlotte VillanuevaNo ratings yet
- Research Ethic Review Form TemplateDocument7 pagesResearch Ethic Review Form Templatejohnlloydt045No ratings yet
- Acupressure Points For Brain StimulationDocument9 pagesAcupressure Points For Brain Stimulationلوليتا وردةNo ratings yet
- TOEFL Writing SamplesDocument3 pagesTOEFL Writing SamplesMai Hà ThanhNo ratings yet
- Introduction to Assessment in Education: Qualities of a Good Traditional TestDocument24 pagesIntroduction to Assessment in Education: Qualities of a Good Traditional TestHarvagale BlakeNo ratings yet
- 42 Rules For Your New Leadership Role - The Manual They Didn't Hand You When You Made VP, Director, or ManagerDocument136 pages42 Rules For Your New Leadership Role - The Manual They Didn't Hand You When You Made VP, Director, or Managerpntuanhcm100% (1)
- Activity Ac 1Document4 pagesActivity Ac 1faye cuevasNo ratings yet
- Great-Management-Lessons - HTML 1. The Elephant RopeDocument99 pagesGreat-Management-Lessons - HTML 1. The Elephant RopeSathyanarayanan Srinivasan RajappaNo ratings yet
- Five Kinds of Listening PDFDocument4 pagesFive Kinds of Listening PDFAnand MauryaNo ratings yet
- Child Development Theories and StagesDocument18 pagesChild Development Theories and StagesRaffy EsquilloNo ratings yet
- Paranoid Mage - InadvisablyCompelledDocument254 pagesParanoid Mage - InadvisablyCompelledspeedsspiegelNo ratings yet
- How People Lived in the PastDocument4 pagesHow People Lived in the PastTram NguyenNo ratings yet
- ESL Language Test English 2024 01-06-47231Document4 pagesESL Language Test English 2024 01-06-47231louiehernandez11No ratings yet
- Final Exam English 12Document2 pagesFinal Exam English 12api-550115538No ratings yet
- Cool Air by H.P. LovecraftDocument13 pagesCool Air by H.P. LovecraftpattoninplaidNo ratings yet
- Project End 2013-14 EvaluationDocument98 pagesProject End 2013-14 Evaluationhoneysinghuk14% (7)
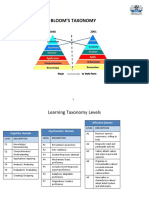
- BloomsTaxonomy SamplesDocument6 pagesBloomsTaxonomy SamplesWan HamizaNo ratings yet
- What Is "Academic" Writing?: by L. Lennie IrvinDocument1 pageWhat Is "Academic" Writing?: by L. Lennie IrvinNeri La LunaNo ratings yet
- Detailed Lesson Plan For English 10Document3 pagesDetailed Lesson Plan For English 10Kristela Tapis ReyesNo ratings yet
- Influencing Factors of Emotional Attachment On Luxury Brands: An Empirical Study in TanzaniaDocument7 pagesInfluencing Factors of Emotional Attachment On Luxury Brands: An Empirical Study in TanzaniaNovelty JournalsNo ratings yet
- What It's Like Being An INTJ Woman Introvert, DearDocument1 pageWhat It's Like Being An INTJ Woman Introvert, DearVaneza PhieterNo ratings yet
- A Practice Theory For Organizational Learning John Shibley PDFDocument6 pagesA Practice Theory For Organizational Learning John Shibley PDFDayana SierraNo ratings yet
- Curriculum EvaluationDocument2 pagesCurriculum Evaluationglenn florNo ratings yet
- JMW PersonaltheoryDocument8 pagesJMW Personaltheoryapi-632123997No ratings yet
- Meskimen Ogl340 Aikidoway ReflectionDocument4 pagesMeskimen Ogl340 Aikidoway Reflectionapi-444454786No ratings yet
- Importance of Travelling Essay: FriendsDocument2 pagesImportance of Travelling Essay: FriendsĐào Trần Nhật AnhNo ratings yet
- A Tale of Three SistersDocument14 pagesA Tale of Three SistersNila AlifahNo ratings yet
- Mariam Mohamed Pema Chunto Making Connections Lab Report TemplateDocument6 pagesMariam Mohamed Pema Chunto Making Connections Lab Report Templateapi-395788256100% (1)
- Senior High School Gretchen S. Osabel: Decoding Watch?V F0Txm-C5Qyy-How H?V Iqsahmtn7N4 - BodyDocument4 pagesSenior High School Gretchen S. Osabel: Decoding Watch?V F0Txm-C5Qyy-How H?V Iqsahmtn7N4 - BodyGretchen SanchezNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (15)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Troubled: A Memoir of Foster Care, Family, and Social ClassFrom EverandTroubled: A Memoir of Foster Care, Family, and Social ClassRating: 4.5 out of 5 stars4.5/5 (25)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeFrom EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeNo ratings yet
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Summary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (61)