You might also like
- Disorders of Maturation MD 3Document34 pagesDisorders of Maturation MD 3wizborrlyzo006No ratings yet
- High Risk New BornDocument36 pagesHigh Risk New BornIze C VijiNo ratings yet
- 1657109667917Document27 pages1657109667917Joanna Bee Rose MagyawiNo ratings yet
- Midterms-NCM-109-Pedia-Lec-Dean (Repaired)Document28 pagesMidterms-NCM-109-Pedia-Lec-Dean (Repaired)Drannel FajardoNo ratings yet
- Fetal Growth DisorderDocument100 pagesFetal Growth Disorderwidia iryuzzaNo ratings yet
- Fetal Growth Restriction - ACOG 2019Document23 pagesFetal Growth Restriction - ACOG 2019Adhitya Yudha MaulanaNo ratings yet
- Prematurity DR KazevuDocument22 pagesPrematurity DR KazevuMoses Jr KazevuNo ratings yet
- Intrauterine Growth Restriction: Diagnosis - No Consensus EFW (Effective Fetal Weight) 10th Centile For Gestational AgeDocument22 pagesIntrauterine Growth Restriction: Diagnosis - No Consensus EFW (Effective Fetal Weight) 10th Centile For Gestational Agedr_ashutosh756078No ratings yet
- Approach To Neonate With Low Birth WeightDocument40 pagesApproach To Neonate With Low Birth Weightnirajan khanalNo ratings yet
- Respiratory Distress Syndrome in A Premature BabyDocument29 pagesRespiratory Distress Syndrome in A Premature BabyVissalini JayabalanNo ratings yet
- I.U.G.R.: Presented byDocument49 pagesI.U.G.R.: Presented byOjer QuayNo ratings yet
- Iugr FinalDocument35 pagesIugr Finalsanthiyasandy100% (4)
- Low Birthweight InfantDocument42 pagesLow Birthweight InfantJoNo ratings yet
- Post MaturityDocument9 pagesPost MaturityM. jehovah Nissie YeshalomeNo ratings yet
- MCN Handouts 3Document25 pagesMCN Handouts 3Jasper Jann AbelisNo ratings yet
- Intrauterine Growth Restriction: Romy Mansour OBGYN Rotation October 2021Document52 pagesIntrauterine Growth Restriction: Romy Mansour OBGYN Rotation October 2021Romy MansourNo ratings yet
- Child Diseases SGA and LGADocument30 pagesChild Diseases SGA and LGACrapster GamingNo ratings yet
- High Risk PediatricsDocument207 pagesHigh Risk Pediatricsruby cubionaNo ratings yet
- FOETAL GROWTH Abnormalities (Autosaved) in NigeriaDocument23 pagesFOETAL GROWTH Abnormalities (Autosaved) in NigeriaIghodaro IsokenNo ratings yet
- Assessment of Fetal Well BeingDocument90 pagesAssessment of Fetal Well BeingSherlinNo ratings yet
- Small For Gestational AgeDocument14 pagesSmall For Gestational AgeMaria Delia Salvado100% (2)
- Growth & Development Neonatology Division, Child Health Department, Medical Faculty of Hasanuddin UniversityDocument44 pagesGrowth & Development Neonatology Division, Child Health Department, Medical Faculty of Hasanuddin Universitynurul dwi ratihNo ratings yet
- PrematurityDocument66 pagesPrematurityJolmajas JoharNo ratings yet
- High Risk Pregnancy HB TranxDocument11 pagesHigh Risk Pregnancy HB TranxangeliquepastranaNo ratings yet
- Birthweight RLTD IssuesDocument14 pagesBirthweight RLTD IssuesnoblefxNo ratings yet
- Student Unit 2 Topic 2.5 Jan 2018 TAYLORDocument42 pagesStudent Unit 2 Topic 2.5 Jan 2018 TAYLORKrista KloseNo ratings yet
- NURSING CARE of AT RISK HIGH RISK SICK CLIENTDocument2 pagesNURSING CARE of AT RISK HIGH RISK SICK CLIENTJanelle ArcillaNo ratings yet
- Test Scribd 3Document42 pagesTest Scribd 3Kiran KumarNo ratings yet
- Prematurity and Low Birth Weight: Sumaiya Bushra Farzana Mahbub Afrina Anjuman SaimaDocument51 pagesPrematurity and Low Birth Weight: Sumaiya Bushra Farzana Mahbub Afrina Anjuman SaimaBiscuits and milkNo ratings yet
- 3amali S9Document34 pages3amali S9Arsh KaiwanNo ratings yet
- Intrauterine Growth Restriction (IUGR)Document7 pagesIntrauterine Growth Restriction (IUGR)redhoprayuda100% (1)
- Obstetrics & Gynecology - SMKDocument187 pagesObstetrics & Gynecology - SMKRSNo ratings yet
- Intrauterine Growth RestrictionDocument26 pagesIntrauterine Growth RestrictionrajaeasNo ratings yet
- High-Risk Newborns and Child During Illness and Hospitalization - Pediatric NursingDocument200 pagesHigh-Risk Newborns and Child During Illness and Hospitalization - Pediatric Nursingjaggermeister20100% (8)
- Lecture 4 - IUGR, Dr. Dr. Diah Rumekti H SP - OG (K) (2021)Document59 pagesLecture 4 - IUGR, Dr. Dr. Diah Rumekti H SP - OG (K) (2021)ofa daniNo ratings yet
- Sga 5Document4 pagesSga 5Shane PangilinanNo ratings yet
- Concept, Assessment, Goals, Objectives of High Risk NewbornDocument76 pagesConcept, Assessment, Goals, Objectives of High Risk NewbornEsha KuttiNo ratings yet
- Script Pedia 1Document38 pagesScript Pedia 1Jessy Arcaina BañagaNo ratings yet
- Gyno... PTL & PRODocument30 pagesGyno... PTL & PROhailemichael chekolNo ratings yet
- Sesion 30 RCIUDocument27 pagesSesion 30 RCIUBrunoindsNo ratings yet
- Term PaperDocument85 pagesTerm PaperAbhilash PaulNo ratings yet
- The High Risk Prenatal ClientDocument46 pagesThe High Risk Prenatal ClientPaul Albert Agunod100% (2)
- 1 AncDocument48 pages1 AncKaruna PrasanthNo ratings yet
- Intrauterine Growth RestrictionDocument40 pagesIntrauterine Growth RestrictionnusriniNo ratings yet
- Small For Gestational Age Presentation 3rd Year MedicineDocument19 pagesSmall For Gestational Age Presentation 3rd Year MedicinedotbotNo ratings yet
- Course Learning OutcomeDocument7 pagesCourse Learning OutcomeJumamoy, Bea ArabelaNo ratings yet
- SEGi ANC and HIGH RISK PREGNANCYDocument65 pagesSEGi ANC and HIGH RISK PREGNANCYAbdulrahman Naji100% (1)
- Antenatal AssessmentDocument40 pagesAntenatal AssessmentKailash NagarNo ratings yet
- Harika Priyanka. K Asst. Professor AconDocument30 pagesHarika Priyanka. K Asst. Professor AconArchana MoreyNo ratings yet
- Intra Uterine Growth Restriction (IUGR)Document44 pagesIntra Uterine Growth Restriction (IUGR)Afiqi FikriNo ratings yet
- Live Preterm Baby Delivered NSDDocument13 pagesLive Preterm Baby Delivered NSDKristine Anne SorianoNo ratings yet
- The Low Birth Weight Infant: Julniar M Tasli Herman BermawiDocument42 pagesThe Low Birth Weight Infant: Julniar M Tasli Herman BermawiJoNo ratings yet
- Fetal Growth RestrictionDocument74 pagesFetal Growth RestrictionKalpavriksha1974No ratings yet
- High Risk Newborn: Problems Related To Maturity Preterm NewbornDocument36 pagesHigh Risk Newborn: Problems Related To Maturity Preterm Newbornwerismy daddyNo ratings yet
- 2 - Ivica Zalud - IUGR Bali 2012.ppt (Read-Only)Document43 pages2 - Ivica Zalud - IUGR Bali 2012.ppt (Read-Only)Azura MotovlogNo ratings yet
- High Risk NewbornDocument76 pagesHigh Risk NewbornVijith.V.kumar91% (22)
- Intrauterinegrowth RestrictionDocument48 pagesIntrauterinegrowth Restrictionshyam792No ratings yet
- Fetal Assessment and Wellbeing in Pregnancy (FetalDocument23 pagesFetal Assessment and Wellbeing in Pregnancy (Fetalapi-3705046100% (1)
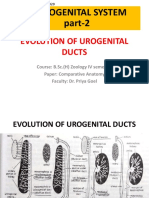
- Evolution of Urogenital Ducts Part-2 27.03.2020Document10 pagesEvolution of Urogenital Ducts Part-2 27.03.2020Sonali SahooNo ratings yet
- Practice Template Red FlagsDocument32 pagesPractice Template Red FlagsAngelaNo ratings yet
- Eco-Farming Melalui Sistem Integrasi Tanaman Dan Ternak Untuk Keberlanjutan Sumberdaya PanganDocument21 pagesEco-Farming Melalui Sistem Integrasi Tanaman Dan Ternak Untuk Keberlanjutan Sumberdaya PanganBayuNo ratings yet
- Karakteristik Ibu Dan Post Natal Treatment (PNT) Berhubungan Dengan Terjadinya Postpartum Blues Ibu NifasDocument7 pagesKarakteristik Ibu Dan Post Natal Treatment (PNT) Berhubungan Dengan Terjadinya Postpartum Blues Ibu NifasNoeng AzZahNo ratings yet
- Knowledge Attitudes and Practices Regarding ModernDocument7 pagesKnowledge Attitudes and Practices Regarding Modernnaasir abdiNo ratings yet
- Activity Sheets in Science 5 Quarter 2, Week 1: Parts of The Reproductive System and Their FunctionsDocument6 pagesActivity Sheets in Science 5 Quarter 2, Week 1: Parts of The Reproductive System and Their Functionsricardo salayonNo ratings yet
- Primary and Secondary Infertility NotesDocument17 pagesPrimary and Secondary Infertility NotesMeangafo GraciaNo ratings yet
- Nclex AobyDocument7 pagesNclex Aobyvienny kayeNo ratings yet
- Pediatric Intake Form SampleDocument10 pagesPediatric Intake Form SampleТравма ЮніверсумNo ratings yet
- Jailcare: Finding The Safety Net For Women Behind BarsDocument1 pageJailcare: Finding The Safety Net For Women Behind BarsGail LeondarWrightNo ratings yet
- Intrahepatic Cholestasis of PregnancyDocument20 pagesIntrahepatic Cholestasis of PregnancyEzequiel GonzalezNo ratings yet
- Conservative Management of Early-Onset Severe Preeclampsia: Comparison Between Randomized and Observational Studies A Systematic ReviewDocument9 pagesConservative Management of Early-Onset Severe Preeclampsia: Comparison Between Randomized and Observational Studies A Systematic ReviewCorey WoodsNo ratings yet
- Thesis of Sarita Thakur - Nursing - 30.01.2021Document146 pagesThesis of Sarita Thakur - Nursing - 30.01.2021Chakrapani ChaturvediNo ratings yet
- A. Menstrual Cycle Here Are Important Events During The Menstrual CycleDocument2 pagesA. Menstrual Cycle Here Are Important Events During The Menstrual CycleRosiro33% (3)
- EINC Handout by Nicole Honrado BSN 2ADocument7 pagesEINC Handout by Nicole Honrado BSN 2A2A - Nicole Marrie HonradoNo ratings yet
- Newborn ScreeningDocument51 pagesNewborn ScreeningDenaya Tika ReskiaNo ratings yet
- Uts Group 2. The Sexual SelfDocument54 pagesUts Group 2. The Sexual SelfFaith BandibasNo ratings yet
- Pregnancy in Women With Systemic Lupus Erythematosus - UpToDateDocument25 pagesPregnancy in Women With Systemic Lupus Erythematosus - UpToDateKarla GonzalezNo ratings yet
- 45 - Breast Developement and AnatomyDocument5 pages45 - Breast Developement and AnatomysasNo ratings yet
- Assisted Breech Delivery1Document28 pagesAssisted Breech Delivery1swatisinghnigeria100% (4)
- Intrauterine Contraceptive Devices Situated KnowledgesDocument14 pagesIntrauterine Contraceptive Devices Situated KnowledgesKathyNogalesNo ratings yet
- Male and Female Infertility: Causes, and Management: September 2019Document7 pagesMale and Female Infertility: Causes, and Management: September 2019Seema SuyalNo ratings yet
- A Case of Chronic Hepatitis B Merged With Acute Fatty Liver of Pregnancy With Severe CoagulopathyDocument4 pagesA Case of Chronic Hepatitis B Merged With Acute Fatty Liver of Pregnancy With Severe CoagulopathyYuna YulianaNo ratings yet
- Fetal MalpresentationDocument13 pagesFetal MalpresentationJhing Rodriguez Borjal75% (4)
- Factors Affecting Utilization of Maternal Health CDocument8 pagesFactors Affecting Utilization of Maternal Health CYussufNo ratings yet
- 1008-Main Article Text (Blinded Article File) - 2118-3-10-20200715Document3 pages1008-Main Article Text (Blinded Article File) - 2118-3-10-20200715putrinrainiNo ratings yet
- Sexual Aspects of Self Group 6Document23 pagesSexual Aspects of Self Group 6Rexlyn Jane CortezNo ratings yet
- Designing and Evaluating Autoverification Rules For Thyroid Function Profiles and Sex Hormone TestsDocument10 pagesDesigning and Evaluating Autoverification Rules For Thyroid Function Profiles and Sex Hormone TestsAli DokumaciogluNo ratings yet
- NCM 109 Problems With Power DraftDocument3 pagesNCM 109 Problems With Power DraftJP Porras AliNo ratings yet
- Prevalence of Postpartum Depression and Interventions Utilized For Its ManagementDocument8 pagesPrevalence of Postpartum Depression and Interventions Utilized For Its ManagementFrida RasyidNo ratings yet