You might also like
- 7.4 Project Execution PlanDocument44 pages7.4 Project Execution PlanUnachukwu Sopulu Sopsy75% (4)
- Principles and Applications of Clinical Mass Spectrometry: Small Molecules, Peptides, and PathogensFrom EverandPrinciples and Applications of Clinical Mass Spectrometry: Small Molecules, Peptides, and PathogensNader RifaiNo ratings yet
- Insert - CalSet Anti-SARS-CoV-2 S.ms - 09289291190.v1.enDocument2 pagesInsert - CalSet Anti-SARS-CoV-2 S.ms - 09289291190.v1.enLilik IndrawatiNo ratings yet
- Autoverification Improved Process Efficiency, Reduced Staff Workload, and Enhanced Staff Satisfaction Using A Critical Path For Result ValidationDocument11 pagesAutoverification Improved Process Efficiency, Reduced Staff Workload, and Enhanced Staff Satisfaction Using A Critical Path For Result ValidationAli DokumaciogluNo ratings yet
- Analysis of Laboratory Critical Value Reporting at A Large Academic Medical CenterDocument7 pagesAnalysis of Laboratory Critical Value Reporting at A Large Academic Medical CenterLevi GasparNo ratings yet
- Validation QuantitiveDocument13 pagesValidation QuantitiveTrần Thị Thùy NgaNo ratings yet
- Automation Boosts Lab ProductivityDocument4 pagesAutomation Boosts Lab ProductivityMuhammad Hanzalah AtifNo ratings yet
- Application of Indices CP and CPK To Improve Quality Control Capability in Clinical Biochemistry LaboratoriesDocument6 pagesApplication of Indices CP and CPK To Improve Quality Control Capability in Clinical Biochemistry LaboratoriesMrinal BhandariNo ratings yet
- QC in Lab ChapterDocument10 pagesQC in Lab ChapterSasabilNo ratings yet
- A Matrix Model For Phlebotomy Quality AssuranceDocument15 pagesA Matrix Model For Phlebotomy Quality AssuranceandhiNo ratings yet
- Enhancing Laboratory Efficiency With Total Laboratory AutomationDocument8 pagesEnhancing Laboratory Efficiency With Total Laboratory AutomationHedo HidayatNo ratings yet
- Effect of Accreditation On Accuracy of Diagnostic Tests in Medical LaboratoriesDocument10 pagesEffect of Accreditation On Accuracy of Diagnostic Tests in Medical LaboratoriesFira Dwi OktavianiNo ratings yet
- The Impact of Laboratory Automation On Performance ImprovementDocument6 pagesThe Impact of Laboratory Automation On Performance ImprovementChris V-PandaNo ratings yet
- Gestión de Las Fases de Pre y Post-Analítica de La PDFDocument12 pagesGestión de Las Fases de Pre y Post-Analítica de La PDFUlises Saldías RoaNo ratings yet
- Critical Result ReportingDocument9 pagesCritical Result ReportingSafiqulatif AbdillahNo ratings yet
- Tugas 1Document9 pagesTugas 1Ramadhan OlongNo ratings yet
- 2007_3_6Document11 pages2007_3_6yonisNo ratings yet
- Linical Aboratory O: S H, MT (Ascp) SH B A. K, E D, Mls (Ascp), Cls (Nca)Document5 pagesLinical Aboratory O: S H, MT (Ascp) SH B A. K, E D, Mls (Ascp), Cls (Nca)Tito LeopardoNo ratings yet
- Najms 6 224Document5 pagesNajms 6 224fioravantipamela1321No ratings yet
- Comparison of Five Commonly Used Automated Susceptibility Testing Methods For Accuracy in The China Antimicrobial Resistance Surveillance System (CARSS) Hospitals PDFDocument12 pagesComparison of Five Commonly Used Automated Susceptibility Testing Methods For Accuracy in The China Antimicrobial Resistance Surveillance System (CARSS) Hospitals PDFntnquynhproNo ratings yet
- Jomb 40 3 2103225ADocument12 pagesJomb 40 3 2103225APhuong LeNo ratings yet
- Week 2 - Overview and Lab MathematicsDocument4 pagesWeek 2 - Overview and Lab Mathematicsbudolera.ph21No ratings yet
- Quality Control in HistopathologyDocument30 pagesQuality Control in HistopathologyMuhammad Jamiu Bello78% (9)
- Bertholf2017 Chapter LaboratoryStructureAndFunctionDocument23 pagesBertholf2017 Chapter LaboratoryStructureAndFunctionci8084102No ratings yet
- Using Outlier Events To Monitor Test Turnaround TimeDocument8 pagesUsing Outlier Events To Monitor Test Turnaround TimeWilmer UcedaNo ratings yet
- 2015 Fda LDT Workshop CapDocument9 pages2015 Fda LDT Workshop CapTadilakshmikiranNo ratings yet
- Good Clinical Laboratory Practice GCLPDocument36 pagesGood Clinical Laboratory Practice GCLPPatrick Kosgei100% (1)
- Original Papers: Pre-Analytical Errors Management in The Clinical Laboratory: A Five-Year StudyDocument10 pagesOriginal Papers: Pre-Analytical Errors Management in The Clinical Laboratory: A Five-Year StudyadrianaNo ratings yet
- Broadhurst 2018 MAS 20 516Document17 pagesBroadhurst 2018 MAS 20 516birgit.feldererNo ratings yet
- Pengendalian Mutu Laboratorium Kimia KliDocument16 pagesPengendalian Mutu Laboratorium Kimia KliNikma 21No ratings yet
- 10.1515_cclm-2022-0878Document8 pages10.1515_cclm-2022-0878controldecalidadlogincaNo ratings yet
- Ajcpath125 0016Document10 pagesAjcpath125 0016Asad AliNo ratings yet
- The REALAB Project A New Method For The PDFDocument9 pagesThe REALAB Project A New Method For The PDFAdrianaManouNo ratings yet
- 1057 PDFDocument11 pages1057 PDFRcristySNo ratings yet
- Lean Six Sigma Methodologies Improve Clinical Laboratory Efficiency and Reduce Turnaround TimesDocument5 pagesLean Six Sigma Methodologies Improve Clinical Laboratory Efficiency and Reduce Turnaround TimesVipul SehgalNo ratings yet
- Mistakes in A Stat Laboratory: Types and Frequency: Clinical Chemistry September 1997Document5 pagesMistakes in A Stat Laboratory: Types and Frequency: Clinical Chemistry September 1997Othman MaaiNo ratings yet
- Principles and Practices of Analytical Method Validation: Validation of Analytical Methods Is Time Consuming But EssentialDocument4 pagesPrinciples and Practices of Analytical Method Validation: Validation of Analytical Methods Is Time Consuming But EssentialMaulik PatelNo ratings yet
- Quality Control Recommendations and Procedures For in Clinical LaboratoriesDocument8 pagesQuality Control Recommendations and Procedures For in Clinical Laboratoriesvitalab llanograndeNo ratings yet
- InTech-Good Clinical Laboratory Practice GCLP For Molecular Based Tests Used in Diagnostic Laboratories PDFDocument26 pagesInTech-Good Clinical Laboratory Practice GCLP For Molecular Based Tests Used in Diagnostic Laboratories PDFLega DeviNo ratings yet
- Lot-To-Lot Variation and Verification - cclm-2022-1126Document8 pagesLot-To-Lot Variation and Verification - cclm-2022-1126Georgiana Daniela DragomirNo ratings yet
- JOURNAL Errors in Clinical Laboratories or Errors in LaboratoryDocument11 pagesJOURNAL Errors in Clinical Laboratories or Errors in LaboratoryVincent ReyesNo ratings yet
- Accreditation of Medical Laboratories - System ProDocument7 pagesAccreditation of Medical Laboratories - System ProSubhasish BarikNo ratings yet
- Laboratory-Developed Tests in Molecular Diagnostics: F - G C T. GDocument10 pagesLaboratory-Developed Tests in Molecular Diagnostics: F - G C T. GCristian AgostiniNo ratings yet
- A Review of Medical Errors in Laboratory Diagnostics and Where We Are TodayDocument4 pagesA Review of Medical Errors in Laboratory Diagnostics and Where We Are TodaytaghamdNo ratings yet
- Improving Quality in Medical LabsDocument7 pagesImproving Quality in Medical LabsNatasha SolanoNo ratings yet
- The Quality of Laboratory Testing TodayDocument13 pagesThe Quality of Laboratory Testing TodaysantoshelapandaNo ratings yet
- 58635 Ce(Ad) f(is) Pf1(Aka Ss) Pfa(Ss) Pn(Ss)Document4 pages58635 Ce(Ad) f(is) Pf1(Aka Ss) Pfa(Ss) Pn(Ss)marvel ecstasyNo ratings yet
- لابDocument66 pagesلابYaRa HamarshehNo ratings yet
- Good Clinical Laboratory Practice (GCLP) : Quality Demanding From Clinical LaboratoriesDocument5 pagesGood Clinical Laboratory Practice (GCLP) : Quality Demanding From Clinical LaboratoriesJaneNo ratings yet
- The Clinical LaboratoryDocument24 pagesThe Clinical LaboratoryRomar DurianNo ratings yet
- The Clinical LaboratoryDocument24 pagesThe Clinical LaboratoryRomar Durian100% (2)
- VisDocument16 pagesVisAyahnyaFidelaFawniaNo ratings yet
- Using SigmaDocument35 pagesUsing SigmaAnonymous 701fZ0Rs7No ratings yet
- Chapitre Validation Diagnostics Assays PDFDocument18 pagesChapitre Validation Diagnostics Assays PDFBuddhi BhaskaraNo ratings yet
- Adjusting Quality Control Chart Limits For WBC, RBC, HB, and PLT Counts To Reduce Daily Control Risks in Hospital LaboratoryDocument11 pagesAdjusting Quality Control Chart Limits For WBC, RBC, HB, and PLT Counts To Reduce Daily Control Risks in Hospital LaboratoryHerbanu PramonoNo ratings yet
- (Clinical Chemistry and Laboratory Medicine (CCLM) ) Implementation of Standardization in Clinical Practice Not Always An Easy TaskDocument5 pages(Clinical Chemistry and Laboratory Medicine (CCLM) ) Implementation of Standardization in Clinical Practice Not Always An Easy TaskJulián Mesa SierraNo ratings yet
- Analytical Validation SOP-0014Document10 pagesAnalytical Validation SOP-0014os4185100% (3)
- Internal Quality Control Practices in Coagulation LaboratoriesDocument10 pagesInternal Quality Control Practices in Coagulation LaboratoriesMy LeNo ratings yet
- Quality Management For The Laboratory: Managers'Document4 pagesQuality Management For The Laboratory: Managers'visiniNo ratings yet
- Quality Indicators in A Hematology Laboratory-A Retrospective AnalysisDocument6 pagesQuality Indicators in A Hematology Laboratory-A Retrospective AnalysisCenyiqanita NurqanitaNo ratings yet
- Errors in Laboratory Testing: Reducing Mistakes Throughout the Total Testing ProcessDocument11 pagesErrors in Laboratory Testing: Reducing Mistakes Throughout the Total Testing ProcessShahid HussainNo ratings yet
- Task 22: Dosen PembmbingDocument3 pagesTask 22: Dosen Pembmbingni'mah hartatiNo ratings yet
- Histopathologic & Cytologic TechniquesDocument9 pagesHistopathologic & Cytologic Techniquescloudiest euniceNo ratings yet
- MEGA HADIATMA - SITI ARIFAH FixDocument10 pagesMEGA HADIATMA - SITI ARIFAH FixDwie RahmawatiNo ratings yet
- Chapter 2 - Industrial Hygiene Surveys and Survey Reports: GeneralDocument40 pagesChapter 2 - Industrial Hygiene Surveys and Survey Reports: GeneralRamadhan Lana ThawadaNo ratings yet
- Non-Invasive Panel For Prediction of Large Esophageal Varices in Patients With HCV-Related Cirrhosis After DAAS TherapyDocument15 pagesNon-Invasive Panel For Prediction of Large Esophageal Varices in Patients With HCV-Related Cirrhosis After DAAS TherapyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- State Common Entrance Test CellDocument100 pagesState Common Entrance Test CellAditya LadhaNo ratings yet
- Annual Audit of Radiation Protection Program-R0Document1 pageAnnual Audit of Radiation Protection Program-R0Sana’ Jabber YaseenNo ratings yet
- Albumin FS : Order Information Assay ProcedureDocument2 pagesAlbumin FS : Order Information Assay Proceduremahardina tsaroyaNo ratings yet
- Problem 1: Group N Mean Std. Deviation Std. Error Mean Scores Type A 10 11.20 2.700 .854 Type B 10 7.20 2.044 .646Document3 pagesProblem 1: Group N Mean Std. Deviation Std. Error Mean Scores Type A 10 11.20 2.700 .854 Type B 10 7.20 2.044 .646aaaaasssNo ratings yet
- BP Open Sampling & Additivisation Procedure 1 - 0Document51 pagesBP Open Sampling & Additivisation Procedure 1 - 0ParaZzzitNo ratings yet
- EID - Guideline - November 2023 (Approved) EIDDocument74 pagesEID - Guideline - November 2023 (Approved) EIDDAPCU TiruvallurNo ratings yet
- NCM 111Document6 pagesNCM 111Erika Mae Sta. MariaNo ratings yet
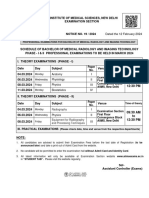
- 19-MRIT Ph-I-II-Date Sheet-MRIT March 2024 WebsiteDocument1 page19-MRIT Ph-I-II-Date Sheet-MRIT March 2024 Websitesoumyajitchakraborty0238No ratings yet
- YUSI AssignmentModule6Document4 pagesYUSI AssignmentModule6Reyne YusiNo ratings yet
- LIPASEDocument4 pagesLIPASEsyufriyadiNo ratings yet
- CAPE Sociology Unit 2 Mark SchemeDocument3 pagesCAPE Sociology Unit 2 Mark SchemeMonique MosesNo ratings yet
- Personality Insight Reflection DISCDocument5 pagesPersonality Insight Reflection DISCnavya sharmaNo ratings yet
- Probability Mixed Practice QDocument2 pagesProbability Mixed Practice QDCNo ratings yet
- REC - 42 - pdf190 Remote InspectionDocument2 pagesREC - 42 - pdf190 Remote InspectionHelmyNo ratings yet
- Research Methodology MCQsDocument3 pagesResearch Methodology MCQsamber tariqNo ratings yet
- BR Biomerieux 9307487006gb Chemunexd Count BrochureDocument2 pagesBR Biomerieux 9307487006gb Chemunexd Count BrochureAbhishek BanerjeeNo ratings yet
- Manual de Usuario de Centrifuge McKessonDocument6 pagesManual de Usuario de Centrifuge McKessonfoxhoundforces100% (1)
- SYLLABUS PSY325 Fall 2018 - CREATED JULY 17Document4 pagesSYLLABUS PSY325 Fall 2018 - CREATED JULY 17gabiNo ratings yet
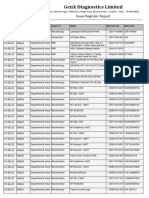
- Aug-23 Stock Issue RegisterDocument14 pagesAug-23 Stock Issue RegistergenxmainstoreNo ratings yet
- ANOVA & ANACOVA and Previous RGUHS Questions With AnswersDocument55 pagesANOVA & ANACOVA and Previous RGUHS Questions With AnswersAjju NagarNo ratings yet
- Theory U1t2 UnlockedDocument11 pagesTheory U1t2 Unlockedcarlos santanaNo ratings yet
- Laboratory OOS Investigations: The Missing LinkDocument46 pagesLaboratory OOS Investigations: The Missing LinkAli GoutasNo ratings yet
- Presentation1 of OSCE-OSPEDocument10 pagesPresentation1 of OSCE-OSPETiku SahuNo ratings yet