You might also like
- Ped Med HandbookDocument27 pagesPed Med HandbookSoad Shedeed0% (1)
- Pediatric Drug DosesDocument8 pagesPediatric Drug DosesReview20No ratings yet
- LorazepamDocument6 pagesLorazepamIanDiel ParagosoNo ratings yet
- Premedication: Presenter-Dr - Srishti Moderator-Dr.R.Pal (Professor) Dr.P. Jain (Associate Professor)Document34 pagesPremedication: Presenter-Dr - Srishti Moderator-Dr.R.Pal (Professor) Dr.P. Jain (Associate Professor)Viresh Upase Roll No 130. / 8th termNo ratings yet
- Atropine Drug StudyDocument3 pagesAtropine Drug StudyMaej83% (6)
- Magnesium Sulfate - Drug InformationDocument10 pagesMagnesium Sulfate - Drug InformationLuisEnriqueDeLaCruzSolanoNo ratings yet
- Preanesthetic Medication JasminaDocument44 pagesPreanesthetic Medication Jasminaanjali sNo ratings yet
- Premedication for Dental SurgeryDocument44 pagesPremedication for Dental Surgeryanjali sNo ratings yet
- Premedication for Dental SurgeryDocument44 pagesPremedication for Dental Surgeryanjali s100% (1)
- Belarmino Drugstudy2Document7 pagesBelarmino Drugstudy2KakaiNo ratings yet
- DiazepamDocument11 pagesDiazepamDina HaryantiNo ratings yet
- For Drug Recitation 1Document33 pagesFor Drug Recitation 1Abigail LonoganNo ratings yet
- Availability: Verapamil HydrochlorideDocument21 pagesAvailability: Verapamil Hydrochloridesteffy sojanNo ratings yet
- Lecture 1. Drugs Used in PremedicationDocument17 pagesLecture 1. Drugs Used in PremedicationSamuel.MoriNo ratings yet
- Weekly Drug CardsDocument43 pagesWeekly Drug CardsErica SanchezNo ratings yet
- Brand Name: Generic Name: Classification: Recommended Dosage, Route, and FrequencyDocument2 pagesBrand Name: Generic Name: Classification: Recommended Dosage, Route, and FrequencyChristine Pialan SalimbagatNo ratings yet
- RanitidineDocument3 pagesRanitidineJoshua PenggeleNo ratings yet
- Drug CardsDocument19 pagesDrug Cardslani83% (6)
- Pediatric General Anesthesia: Moderator-Dr Tripat Kaur. Presenter - DR Ikjot KaurDocument80 pagesPediatric General Anesthesia: Moderator-Dr Tripat Kaur. Presenter - DR Ikjot Kaurashwini priyaNo ratings yet
- PLASIL antiemetics classificationDocument5 pagesPLASIL antiemetics classificationAbby MontealegreNo ratings yet
- Pro Pre Medication in NeonatesDocument31 pagesPro Pre Medication in Neonateselizeushanindito8113No ratings yet
- Advantages Disadvantages: Sedative Premedication Guidelines at RCHDocument3 pagesAdvantages Disadvantages: Sedative Premedication Guidelines at RCHdwNo ratings yet
- Ranitidine Drug Data for Erosive EsophagitisDocument3 pagesRanitidine Drug Data for Erosive EsophagitisArnzz AgbulosNo ratings yet
- AtropineDocument3 pagesAtropinegovind_soni_15No ratings yet
- analgesicsedationdrugsDocument4 pagesanalgesicsedationdrugshevere6273No ratings yet
- Generic Name: Acetaminophen Brand Name: Tylenol: ActionDocument22 pagesGeneric Name: Acetaminophen Brand Name: Tylenol: Actionp_dawg100% (14)
- PICU drug therapy challenges and safe administrationDocument32 pagesPICU drug therapy challenges and safe administrationNeethu Mariya MathewNo ratings yet
- Peptic Ulcer Disease DrugsDocument6 pagesPeptic Ulcer Disease DrugsApple MaeNo ratings yet
- Emergency and Critical CareDocument1 pageEmergency and Critical CareRodrigo Olmedo OrellanaNo ratings yet
- Paediatric Pam I DR On Ate IV MonographDocument2 pagesPaediatric Pam I DR On Ate IV MonographDouglas MutenyoNo ratings yet
- Hydralazine.1 3Document1 pageHydralazine.1 3SNo ratings yet
- Vademecum PDFDocument36 pagesVademecum PDFwalter0% (1)
- Midazolam: Disusun Untuk Memenuhi Tugas Mata Kuliah Farmakologi Dosen Pengampu: Apt. Drs. Muh Khusnul Khuluq, M.FarmDocument5 pagesMidazolam: Disusun Untuk Memenuhi Tugas Mata Kuliah Farmakologi Dosen Pengampu: Apt. Drs. Muh Khusnul Khuluq, M.Farmtiara shinta dewiNo ratings yet
- Drugstudy OrsdDocument10 pagesDrugstudy OrsdRafmar A. SalundaguitNo ratings yet
- Pediatric Dosage CalculationsDocument5 pagesPediatric Dosage CalculationsLovely Anjenell MacalingaNo ratings yet
- Key Points: Balanced Anesthesia in Small Animal Patients: Incorporating Cri'SDocument2 pagesKey Points: Balanced Anesthesia in Small Animal Patients: Incorporating Cri'SAlejandro Estrada RiosNo ratings yet
- Gastrointestinal Diseases: Clinical Pharmacist Hasan BayashotDocument117 pagesGastrointestinal Diseases: Clinical Pharmacist Hasan BayashotRawabi SalehNo ratings yet
- How Antispasmodic Agents Work to Relieve GI DiscomfortDocument11 pagesHow Antispasmodic Agents Work to Relieve GI Discomfortairon jakeNo ratings yet
- AminophyllineDocument3 pagesAminophyllineAmna Kazmi ShehzadNo ratings yet
- PICU Protocol 1 Ain Shams UniversityDocument52 pagesPICU Protocol 1 Ain Shams UniversityAhmad ElgazzarNo ratings yet
- Farmakologi Saluran Cerna: Nasruhan Arifianto Stikes - Buana HusadaDocument21 pagesFarmakologi Saluran Cerna: Nasruhan Arifianto Stikes - Buana Husadaandyra betanamaNo ratings yet
- Iligan - DiazepamDocument6 pagesIligan - DiazepamJamaicah IliganNo ratings yet
- Padilla-Drug StudyDocument5 pagesPadilla-Drug Studybunso padillaNo ratings yet
- Atropine SulfateDocument6 pagesAtropine SulfateManelle SingzonNo ratings yet
- ASM Use Childhood Epilepsy PDFDocument7 pagesASM Use Childhood Epilepsy PDFIchrak GhachemNo ratings yet
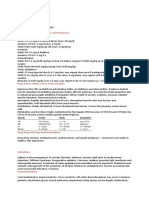
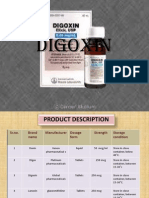
- DigoxinDocument20 pagesDigoxinAbdulRehmanChaudaryNo ratings yet
- Medication: Captopril (Capoten) Is An ACE Inhibitor and A Common Antihypertensive. Captopril Generic Name Contents (Hide)Document43 pagesMedication: Captopril (Capoten) Is An ACE Inhibitor and A Common Antihypertensive. Captopril Generic Name Contents (Hide)Kath Rubio0% (1)
- Common Drugs in Obsgyn 2Document42 pagesCommon Drugs in Obsgyn 2Meekel SusikuNo ratings yet
- Indications and Usage: M M M M M M M M M M MDocument4 pagesIndications and Usage: M M M M M M M M M M MJesthony Lee CorderoNo ratings yet
- DATE ORDERED: August 15, 2009 ORDERED DOSE: 50 Ig IVTT Q 8 Hours GENERIC NAME: Ranitidine Brand Name/SDocument4 pagesDATE ORDERED: August 15, 2009 ORDERED DOSE: 50 Ig IVTT Q 8 Hours GENERIC NAME: Ranitidine Brand Name/SConn_Casipe_8158No ratings yet
- EhrDocument4 pagesEhrapi-608465780No ratings yet
- No SpaDocument6 pagesNo SpaIlyes FerenczNo ratings yet
- Medications for Pain ManagementDocument8 pagesMedications for Pain ManagementapalestiNo ratings yet
- Pediatric Drug ReferenceDocument86 pagesPediatric Drug Referenceromaine_as100% (1)
- Appendicitis DrugsDocument6 pagesAppendicitis DrugsCross0No ratings yet
- Antipsychotic DrugsDocument2 pagesAntipsychotic DrugsDana Mae AfanNo ratings yet
- Insulin GNTDocument41 pagesInsulin GNTV Narayan Rao TummalaNo ratings yet
- Salazar Medsurg Drug StudyDocument2 pagesSalazar Medsurg Drug StudyAlyssa Marie PepitoNo ratings yet
- Fix Your Genes to Fit Your Jeans: Optimizing Diet, Health and Weight Through Personal GeneticsFrom EverandFix Your Genes to Fit Your Jeans: Optimizing Diet, Health and Weight Through Personal GeneticsNo ratings yet
- Sepsis & Septic Shock: Case Studies in Therapeutics (Iv)Document23 pagesSepsis & Septic Shock: Case Studies in Therapeutics (Iv)Dima MasadehNo ratings yet
- Overview of Clinical and Pharmacy Practice Research: Mayyada Wazaify, PHD March 2023Document53 pagesOverview of Clinical and Pharmacy Practice Research: Mayyada Wazaify, PHD March 2023Dima MasadehNo ratings yet
- Evidence Based Medicine:: The Know What, How and Where!Document68 pagesEvidence Based Medicine:: The Know What, How and Where!Dima MasadehNo ratings yet
- Research: Critical ThinkingDocument39 pagesResearch: Critical ThinkingDima MasadehNo ratings yet
- Not Associated With Significant Weight GainDocument9 pagesNot Associated With Significant Weight GainDima MasadehNo ratings yet
- Surgical Protocol - ImplanTize CompactDocument12 pagesSurgical Protocol - ImplanTize CompactGonçalo Cunha-CoutinhoNo ratings yet
- SeminarDocument34 pagesSeminarMuhammad Faiz Satria WibowoNo ratings yet
- A&P - 2. Blood Vessels of The Brain (9p)Document9 pagesA&P - 2. Blood Vessels of The Brain (9p)Gabriel StratulatNo ratings yet
- Multiple PregnancyDocument55 pagesMultiple PregnancyNathaniel YeriNo ratings yet
- Ganesh Pediatric Intraocular Lens Power CalculationDocument5 pagesGanesh Pediatric Intraocular Lens Power CalculationViraNo ratings yet
- PMMA Antibiotic Bead Chains for Local Antibiotic DeliveryDocument4 pagesPMMA Antibiotic Bead Chains for Local Antibiotic DeliverySakthi Annamalai.cNo ratings yet
- Standard and Non-Standard Sciatica Acupuncture PointsDocument3 pagesStandard and Non-Standard Sciatica Acupuncture PointsAndrei PetriciNo ratings yet
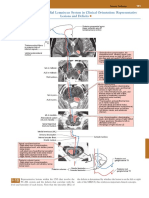
- Posterior Column-Medial Lemniscus System in Clinical Orientation: Representative Lesions and DeficitsDocument1 pagePosterior Column-Medial Lemniscus System in Clinical Orientation: Representative Lesions and DeficitsEduardo RodriguezNo ratings yet
- Anatomy Part 2Document3 pagesAnatomy Part 2ashna anilNo ratings yet
- Healing and RepairDocument38 pagesHealing and RepairDr.rajender ThakralNo ratings yet
- Direction: Encircle The Letter of The Correct AnswerDocument2 pagesDirection: Encircle The Letter of The Correct Answerariel agos100% (1)
- Ape - Endorsement LetterDocument1 pageApe - Endorsement LetterIsmael Brix ChanNo ratings yet
- Licensing Fee Schedule for Healthcare FacilitiesDocument1 pageLicensing Fee Schedule for Healthcare FacilitiesMuhammad ZubairNo ratings yet
- Anatomy and Physiology Lab WorksheetDocument7 pagesAnatomy and Physiology Lab WorksheetJANE ACEVEDONo ratings yet
- Single Use Cannula V-System: Efficient ERCP Cannulation & ExchangeDocument18 pagesSingle Use Cannula V-System: Efficient ERCP Cannulation & ExchangeEny Sri RyNo ratings yet
- Brochure - STAAR Surgical - EVO Visian ICL (Surgeon Brochure) (En)Document12 pagesBrochure - STAAR Surgical - EVO Visian ICL (Surgeon Brochure) (En)Andreea L. MihalceaNo ratings yet
- VBMDocument24 pagesVBMSupervisor HCVNo ratings yet
- Clinical Manifestations and Evaluation of Adults With Suspected Left-Sided Native Valve Endocarditis - UpToDateDocument35 pagesClinical Manifestations and Evaluation of Adults With Suspected Left-Sided Native Valve Endocarditis - UpToDateSyed Akram AliNo ratings yet
- Nervio FacialDocument3 pagesNervio FacialAngélica Valenzuela AndrighiNo ratings yet
- Abdominoplasty Classic Principles and TechniqueDocument18 pagesAbdominoplasty Classic Principles and TechniqueJonathan Zenteno JiménezNo ratings yet
- Risk Factors Contributing To Symptomatic Plate Removal in Orthognathic Surgery PatientsDocument4 pagesRisk Factors Contributing To Symptomatic Plate Removal in Orthognathic Surgery PatientsAli FaridiNo ratings yet
- Nursing Process Stages and PurposesDocument30 pagesNursing Process Stages and PurposesAlyanna TiglaoNo ratings yet
- Start: Completion of The Surgical ChecklistDocument3 pagesStart: Completion of The Surgical ChecklistAliyah Jewel JimenezNo ratings yet
- Treatment of Distal Tibial Fractures With Ilizarov Methodology. Maurizio A. CatagniDocument15 pagesTreatment of Distal Tibial Fractures With Ilizarov Methodology. Maurizio A. CatagniNuno Craveiro LopesNo ratings yet
- Abdominal PeDocument52 pagesAbdominal PeEd Alexis LicarteNo ratings yet
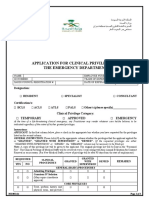
- Ms-001 (2) Clinical Priv Form Emergency 2019Document3 pagesMs-001 (2) Clinical Priv Form Emergency 2019Athira Rajan100% (2)
- Floating ShoulderDocument10 pagesFloating ShoulderMuhamad Amar'sNo ratings yet
- Ventilator SynoVent E5 Standard ConfigurationDocument2 pagesVentilator SynoVent E5 Standard ConfigurationAlfie FachryNo ratings yet
- Skin GraftingDocument3 pagesSkin GraftingTrish PangilinanNo ratings yet
- CBCTDocument19 pagesCBCTFernanda CombaNo ratings yet