You might also like
- Science 9 Q1 Module 1 Respiratory and Circulatory With Key AnswerDocument42 pagesScience 9 Q1 Module 1 Respiratory and Circulatory With Key AnswerJan Ice90% (128)
- Young Child with Acute Respiratory DistressDocument25 pagesYoung Child with Acute Respiratory Distresspriyarajan007100% (2)
- Mosaicplasty 1030208g UsDocument12 pagesMosaicplasty 1030208g UsAnil SoodNo ratings yet
- Pathology exam preparationDocument7 pagesPathology exam preparationRIZ KHANNo ratings yet
- 75T BP DPS 2 AHTS Vessel for Oil & Gas OperationsDocument2 pages75T BP DPS 2 AHTS Vessel for Oil & Gas OperationsJason UchennnaNo ratings yet
- Chinese Auricular Acupuncture 2nd EditionDocument57 pagesChinese Auricular Acupuncture 2nd Editiongordon.gibson456100% (37)
- Applications: Functions andDocument350 pagesApplications: Functions andJason UchennnaNo ratings yet
- Defibrillators (C)Document41 pagesDefibrillators (C)Percy Caceres OlivaresNo ratings yet
- GCS dan REMS dalam Memprediksi Outcome Pasien Trauma KepalaDocument12 pagesGCS dan REMS dalam Memprediksi Outcome Pasien Trauma KepalaSatria Yosi HernawanNo ratings yet
- An Epidemiologic Study of 389 Children With EpilepDocument6 pagesAn Epidemiologic Study of 389 Children With Epilepbilal hadiNo ratings yet
- International Journal Health Research: Peer-Reviewed Online JournalDocument6 pagesInternational Journal Health Research: Peer-Reviewed Online JournaldsNo ratings yet
- Etiology, Clinical Profile and Outcome of First Episode of Seizure in ChildrenDocument5 pagesEtiology, Clinical Profile and Outcome of First Episode of Seizure in ChildrenUlan SariNo ratings yet
- The Complex Aetiology of Cerebral PalsyDocument16 pagesThe Complex Aetiology of Cerebral PalsyAileen MéndezNo ratings yet
- Edward R Newton The Relationship Between IntrapartumDocument10 pagesEdward R Newton The Relationship Between IntrapartumJonathan GrandasNo ratings yet
- Pediatric Neurology: David Dufresne MD, Lynn Dagenais BSC, Michael I. Shevell MD Repacq ConsortiumDocument4 pagesPediatric Neurology: David Dufresne MD, Lynn Dagenais BSC, Michael I. Shevell MD Repacq ConsortiumNelviza RiyantiNo ratings yet
- Ophthalmogenetic and Epidemiological Studies of Egyptian Children With Mental RetardationDocument8 pagesOphthalmogenetic and Epidemiological Studies of Egyptian Children With Mental Retardationray m deraniaNo ratings yet
- Predictors of Unprovoked Seizure After Febrile Seizure: Short-Term OutcomesDocument7 pagesPredictors of Unprovoked Seizure After Febrile Seizure: Short-Term Outcomesrizad mohamadNo ratings yet
- JournalDocument6 pagesJournalnaelarizqiNo ratings yet
- Research: Neurological Sequelae in Survivors of Cerebral MalariaDocument9 pagesResearch: Neurological Sequelae in Survivors of Cerebral MalariaHervi LaksariNo ratings yet
- Prevalence of Schizophrenia Among Patients Admitted Into Neuro-Psychiatric Hospital, Rumuigbo, Port Harcourt, Rivers State, NigeriaDocument9 pagesPrevalence of Schizophrenia Among Patients Admitted Into Neuro-Psychiatric Hospital, Rumuigbo, Port Harcourt, Rivers State, NigeriaSteven JonesNo ratings yet
- Specific learning disorders and epilepsy factors in childrenDocument14 pagesSpecific learning disorders and epilepsy factors in childrensarahNo ratings yet
- An Analysis of Breakthrough Seizures and Related Factors in Paediatric EpilepsyDocument4 pagesAn Analysis of Breakthrough Seizures and Related Factors in Paediatric Epilepsygogih64190No ratings yet
- Tsao-2020-Long-term Neurodevelopmental OutcomeDocument8 pagesTsao-2020-Long-term Neurodevelopmental OutcomeHidayatt NurulNo ratings yet
- Clinico-Epidemiological ProfileDocument7 pagesClinico-Epidemiological ProfilephylienNo ratings yet
- Presentation Clinical Spectrum and Chromosomal Abnormalities of Children With Turner 1251Document6 pagesPresentation Clinical Spectrum and Chromosomal Abnormalities of Children With Turner 1251Mai SomaaNo ratings yet
- Pre-hospital Management of Febrile Seizures in ChildrenDocument5 pagesPre-hospital Management of Febrile Seizures in Childrenchaz5727xNo ratings yet
- Early Prognostic SeizureDocument10 pagesEarly Prognostic SeizureApriliyani IndrawatiNo ratings yet
- Knowledge Level and Determinants of Neonatal Jaundice A Cross-Sectional Study in The Effutu Municipality of GhanaDocument10 pagesKnowledge Level and Determinants of Neonatal Jaundice A Cross-Sectional Study in The Effutu Municipality of GhananicloverNo ratings yet
- Retrospective Survey of Perinatal Risk Factors in 104 Children With HoloprosencephalyDocument6 pagesRetrospective Survey of Perinatal Risk Factors in 104 Children With HoloprosencephalyFlávia MateusNo ratings yet
- Crawford 2005 EpilepsiaDocument50 pagesCrawford 2005 Epilepsiahendra_padangNo ratings yet
- Long-Term Follow-Up of Newborns at Neurological Risk: Research Open AccessDocument8 pagesLong-Term Follow-Up of Newborns at Neurological Risk: Research Open Accessleivaherre10No ratings yet
- INCLEN Diagnostic Tool For Epilepsy (INDT-EPI) For Primary Care Physicians: Development and ValidationDocument5 pagesINCLEN Diagnostic Tool For Epilepsy (INDT-EPI) For Primary Care Physicians: Development and ValidationAulya ArchuletaNo ratings yet
- Special Report 2010.xDocument15 pagesSpecial Report 2010.xDianMuliasariNo ratings yet
- Posterior Fossa Metaanalysis 2016 Part 2Document24 pagesPosterior Fossa Metaanalysis 2016 Part 2SahasraNo ratings yet
- Pediatric NeurologyDocument7 pagesPediatric NeurologyFarin MauliaNo ratings yet
- The Problems of Moderate Preterm Infants: Seminars in PerinatologyDocument4 pagesThe Problems of Moderate Preterm Infants: Seminars in Perinatologysam crushNo ratings yet
- Childhood Eating Disorders British National Surveillance StudyDocument7 pagesChildhood Eating Disorders British National Surveillance StudygharrisanNo ratings yet
- Neonatal JaundiceDocument4 pagesNeonatal JaundiceVictor UgoslyNo ratings yet
- Epidemiology of Pediatric Acute Encephalitis/Encephalopathy in JapanDocument7 pagesEpidemiology of Pediatric Acute Encephalitis/Encephalopathy in Japaneko andryNo ratings yet
- Prader WilliDocument15 pagesPrader WilliGVHHNo ratings yet
- Articol 1Document7 pagesArticol 1nistor97No ratings yet
- Perioperative Risk Factors For Neurological Impairment in Infants With Acute Liver Failure Following Liver TransplantationDocument8 pagesPerioperative Risk Factors For Neurological Impairment in Infants With Acute Liver Failure Following Liver TransplantationFernando Vazquez SSNo ratings yet
- Incidence and Prevalence of Childhood Epilepsy: A Nationwide Cohort StudyDocument11 pagesIncidence and Prevalence of Childhood Epilepsy: A Nationwide Cohort StudyasfwegereNo ratings yet
- Neurodevelopmental Delay Among Young Children in NigeriaDocument5 pagesNeurodevelopmental Delay Among Young Children in NigeriaRafika Cici AmeliaNo ratings yet
- Icbt07i4p369 PDFDocument6 pagesIcbt07i4p369 PDFretNo ratings yet
- 6754-Article Text-108154-1-10-20230524Document7 pages6754-Article Text-108154-1-10-20230524JOSHUA IARA BIAGNo ratings yet
- Tkachenko 2016Document17 pagesTkachenko 2016Phạm Văn HiệpNo ratings yet
- Neonatal Seizures : Types, Etiology and Long Term Neurodevelopmental Out-Come at A Tertiary Care HospitalDocument7 pagesNeonatal Seizures : Types, Etiology and Long Term Neurodevelopmental Out-Come at A Tertiary Care HospitalAgung NohuNo ratings yet
- Risk Factors For Seizures and Epilepsy in Children With Congenital Heart DiseaseDocument6 pagesRisk Factors For Seizures and Epilepsy in Children With Congenital Heart DiseaseclaudyNo ratings yet
- PHD Thesis EpilepsyDocument8 pagesPHD Thesis EpilepsyBestOnlinePaperWritersSingapore100% (2)
- She Vell 2003Document15 pagesShe Vell 2003Ivan VeriswanNo ratings yet
- Evaluation of The Child With Global Developmental DelayDocument14 pagesEvaluation of The Child With Global Developmental DelaylauramwoodyardNo ratings yet
- 1377 FullDocument23 pages1377 FullPutri Wahyuni AllfazmyNo ratings yet
- Febrile Convulsions Among Children Admitted in University of Port Harcourt Teaching Hospital, Rivers State, NigeriaDocument7 pagesFebrile Convulsions Among Children Admitted in University of Port Harcourt Teaching Hospital, Rivers State, NigeriaAzam alausyNo ratings yet
- Evaluation of Prescription Pattern and Risk Factors of Epilepsy in ChildrenDocument11 pagesEvaluation of Prescription Pattern and Risk Factors of Epilepsy in ChildrenTshiva AryalNo ratings yet
- Nelson, 1978Document10 pagesNelson, 1978Arisa RosyadaNo ratings yet
- Ficha Bibliografica de Parasitosis IntestinalDocument44 pagesFicha Bibliografica de Parasitosis Intestinalconsultorio la cardeneraNo ratings yet
- Papier EpilepsieDocument5 pagesPapier EpilepsieCelebre MualabaNo ratings yet
- ArticuloDocument13 pagesArticuloCecilia Murrieta LimonNo ratings yet
- Santoso 2020Document10 pagesSantoso 2020Aldo VictoriaNo ratings yet
- Literature Review Neonatal JaundiceDocument6 pagesLiterature Review Neonatal Jaundiceafdtvdcwf100% (1)
- 10 11648 J CNN 20200402 12Document4 pages10 11648 J CNN 20200402 12inunNo ratings yet
- Comorbidities in CerebrDocument9 pagesComorbidities in CerebrsaadchalidNo ratings yet
- Neonatal MRI To Predict Neurodevelopmental Outcomes in Preterm InfantsDocument10 pagesNeonatal MRI To Predict Neurodevelopmental Outcomes in Preterm InfantsJuan Camilo LandazuriNo ratings yet
- final thesis copyDocument22 pagesfinal thesis copyroshen02No ratings yet
- 2021 Article 817Document10 pages2021 Article 817Muriel FialiwanNo ratings yet
- Nephrotic Syndrome Among Children in Kano: A Clinicopathological StudyDocument6 pagesNephrotic Syndrome Among Children in Kano: A Clinicopathological StudyBANGDE TVNo ratings yet
- Risk Factors of Hearing Loss in Children Under 10 Years of Age - A Clinical Study in A Tertiary Care CentreDocument6 pagesRisk Factors of Hearing Loss in Children Under 10 Years of Age - A Clinical Study in A Tertiary Care CentreIJAR JOURNALNo ratings yet
- Childhood Seized: Linguistic Considerations of the Effects of Epilepsy on Cognition in Children with Benign Childhood EpilepsyFrom EverandChildhood Seized: Linguistic Considerations of the Effects of Epilepsy on Cognition in Children with Benign Childhood EpilepsyNo ratings yet
- My Attempt 1Document2 pagesMy Attempt 1Jason UchennnaNo ratings yet
- Moxyyy MtoDocument4 pagesMoxyyy MtoJason UchennnaNo ratings yet
- New Pdms CommAndsDocument19 pagesNew Pdms CommAndsJason UchennnaNo ratings yet
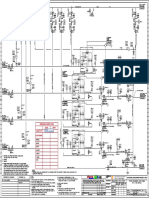
- P&IDDocument1 pageP&IDJason UchennnaNo ratings yet
- FUnction ApproximationDocument40 pagesFUnction ApproximationJason UchennnaNo ratings yet
- Lesson 33Document15 pagesLesson 33Jason UchennnaNo ratings yet
- The Riccati and Ermakov-Pinney HierarchiesDocument21 pagesThe Riccati and Ermakov-Pinney HierarchiesJason UchennnaNo ratings yet
- The Painlev e Methods (R. Conte and M. Mussette)Document29 pagesThe Painlev e Methods (R. Conte and M. Mussette)Jason UchennnaNo ratings yet
- Examples of Isometric Texts: All Written Information Should Remain OnDocument1 pageExamples of Isometric Texts: All Written Information Should Remain OnJason UchennnaNo ratings yet
- Differential Equations in MapleDocument14 pagesDifferential Equations in MapleAscanio BarbosaNo ratings yet
- My Attempt 1Document2 pagesMy Attempt 1Jason UchennnaNo ratings yet
- A Computational Approach For The Analytical Solving of Partial Differential Equations (Cheb-Terrab, E.S., and Von Bulow, K.)Document18 pagesA Computational Approach For The Analytical Solving of Partial Differential Equations (Cheb-Terrab, E.S., and Von Bulow, K.)Jason UchennnaNo ratings yet
- Z G W Z F DZ DW W DZ W D: Ince, E. L. (1926) - Ordinary Differential Equations. London: LongmansDocument1 pageZ G W Z F DZ DW W DZ W D: Ince, E. L. (1926) - Ordinary Differential Equations. London: LongmansJason UchennnaNo ratings yet
- Dear Sir, Below Is The Equation I Referred To in The Email.: W Z F C DZ DW W DZ W DDocument1 pageDear Sir, Below Is The Equation I Referred To in The Email.: W Z F C DZ DW W DZ W DJason UchennnaNo ratings yet
- UntitledDocument1 pageUntitledJason UchennnaNo ratings yet
- Alfred RamaniDocument2 pagesAlfred RamaniJason UchennnaNo ratings yet
- Robert Conte'sDocument11 pagesRobert Conte'sJason UchennnaNo ratings yet
- Some Materials From BookseeDocument2 pagesSome Materials From BookseeJason UchennnaNo ratings yet
- The American StatisticianDocument3 pagesThe American StatisticianJason UchennnaNo ratings yet
- Crest Star 3 - SpecsDocument3 pagesCrest Star 3 - SpecsJason UchennnaNo ratings yet
- IOP. A. Math. Gen.28 (1995) Hidden and contact symmetries of ODEsDocument11 pagesIOP. A. Math. Gen.28 (1995) Hidden and contact symmetries of ODEsJason UchennnaNo ratings yet
- Regularity Criteria For Hyperbolic Navier-Stokes and Related SystemDocument8 pagesRegularity Criteria For Hyperbolic Navier-Stokes and Related SystemSam SonNo ratings yet
- Section of A Fibre BundleDocument2 pagesSection of A Fibre BundleJason UchennnaNo ratings yet
- MDPL Asha DeepDocument1 pageMDPL Asha DeepJason UchennnaNo ratings yet
- MDPL 9-60tDocument2 pagesMDPL 9-60tJason UchennnaNo ratings yet
- A Primer On Elliptic Functions With Applications in Classical Mechanics (Alan Blaisard)Document23 pagesA Primer On Elliptic Functions With Applications in Classical Mechanics (Alan Blaisard)Jason UchennnaNo ratings yet
- On generalized elliptic integrals and modular functionsDocument79 pagesOn generalized elliptic integrals and modular functionsJason UchennnaNo ratings yet
- Solvable Models of Relativistic Charged Spherically Symmetric Fluids (Rod Halburd)Document15 pagesSolvable Models of Relativistic Charged Spherically Symmetric Fluids (Rod Halburd)Jason UchennnaNo ratings yet
- Screening TestDocument4 pagesScreening TestTed Martinez Desiderio Jr.No ratings yet
- Catheter Ablationin in AF With CHFDocument11 pagesCatheter Ablationin in AF With CHFKristian Sudana HartantoNo ratings yet
- PATH Fit module on safety protocols and exercise health appraisalDocument1 pagePATH Fit module on safety protocols and exercise health appraisaljinNo ratings yet
- LEC 1 Microbiology Intro and Hx. Lec 1Document62 pagesLEC 1 Microbiology Intro and Hx. Lec 1nicewanNo ratings yet
- Manage Newborn HypothermiaDocument3 pagesManage Newborn HypothermiaYwagar YwagarNo ratings yet
- Drugs Used in Disorders of CoagulationDocument6 pagesDrugs Used in Disorders of CoagulationAimee Redor100% (1)
- NCP FinalDocument4 pagesNCP Finalmarkanthony3903No ratings yet
- MEGACODEDocument6 pagesMEGACODESafety JNo ratings yet
- Aids HandoutDocument2 pagesAids Handoutapi-272957818No ratings yet
- Nursing Care PlanDocument10 pagesNursing Care PlanSittie Rohaina SabanNo ratings yet
- AbscessDocument4 pagesAbscessShivBalakChauhanNo ratings yet
- Basic Pharmacovigilance Interview Questions For FRESHERSDocument8 pagesBasic Pharmacovigilance Interview Questions For FRESHERSPrakash MishraNo ratings yet
- CP For Eye NurseDocument3 pagesCP For Eye NursemelanNo ratings yet
- Pathologt of The HeartDocument40 pagesPathologt of The HeartJudithNo ratings yet
- Recent Updates On Nanomedicine Based Products: Current Sce-Nario and Future OpportunitiesDocument13 pagesRecent Updates On Nanomedicine Based Products: Current Sce-Nario and Future OpportunitiesvijuNo ratings yet
- CT Bowel WallDocument12 pagesCT Bowel WallBrian LucasNo ratings yet
- Family Case StudyDocument25 pagesFamily Case StudyJezner GamosNo ratings yet
- Introduction To Functional Electrical StimulationDocument14 pagesIntroduction To Functional Electrical StimulationJia HuiNo ratings yet
- Inborn Error of MetabolismDocument13 pagesInborn Error of MetabolismKuzhandai VeluNo ratings yet
- ArikDocument14 pagesArikArditya Romy Stay CoolNo ratings yet
- Thoracentesis Reflective EssayDocument2 pagesThoracentesis Reflective EssayAnjae GariandoNo ratings yet
- Implantology and The Severely Resorbed Edentulous MandibleDocument9 pagesImplantology and The Severely Resorbed Edentulous MandibleAfiz ZullahNo ratings yet
- 3817 Respiratory PreworkDocument3 pages3817 Respiratory PreworkAhmad BustamiNo ratings yet