You might also like
- Diagnosis & Evaluation of Respiratory DiseaseDocument99 pagesDiagnosis & Evaluation of Respiratory DiseaseAmalia Intan PermataNo ratings yet
- Family Case Presentation: Abat FamilyDocument80 pagesFamily Case Presentation: Abat FamilyGeraldine Marie SalvoNo ratings yet
- Comprehensive Clerkship Guide by Iferika JRDocument29 pagesComprehensive Clerkship Guide by Iferika JRtemitopeNo ratings yet
- Respiratory ExamDocument7 pagesRespiratory ExamBeomjun LeeNo ratings yet
- 2 History TakingDocument43 pages2 History TakingMohammad_Islam87100% (1)
- Shortness of Breath NotesDocument7 pagesShortness of Breath NotesChananNo ratings yet
- History Taking of Respiratory System 2003Document24 pagesHistory Taking of Respiratory System 2003YudiWatanabeNo ratings yet
- History TakingDocument19 pagesHistory TakingAlice Verran100% (1)
- HX TakingDocument37 pagesHX TakingAya SalahNo ratings yet
- Common General Practice Consultations - Notes For OSCEsDocument53 pagesCommon General Practice Consultations - Notes For OSCEsChanel ClarkNo ratings yet
- Chapt 06Document49 pagesChapt 06brentupdegraffNo ratings yet
- OSCE: Respiratory History and ExaminationDocument10 pagesOSCE: Respiratory History and ExaminationShahin KazemzadehNo ratings yet
- AsthmaDocument72 pagesAsthmaPatrick DycocoNo ratings yet
- Osce, BaselDocument302 pagesOsce, Baselbpjavi78% (9)
- g1b Asthma PDFDocument75 pagesg1b Asthma PDFAniq Zahran MasomNo ratings yet
- History and Causology - DR - ShamolDocument265 pagesHistory and Causology - DR - ShamolUmer Farooq100% (1)
- Pharm2an Eng-Signs SymptomesDocument4 pagesPharm2an Eng-Signs SymptomesBassirou BassanNo ratings yet
- Medicine: CardiorespiratoryDocument56 pagesMedicine: CardiorespiratoryWalaa abo foolNo ratings yet
- Heavy Periods 6 Pads/day: CasesDocument31 pagesHeavy Periods 6 Pads/day: Caseswalt65No ratings yet
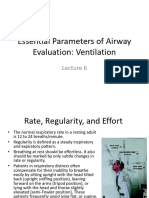
- Essential Parameters of Airway Evaluation Lecture 6Document27 pagesEssential Parameters of Airway Evaluation Lecture 69yqgmkvyzdNo ratings yet
- Respiratory System - History & Physical Examination: Mohan KumarDocument35 pagesRespiratory System - History & Physical Examination: Mohan KumaraagarwalmdNo ratings yet
- Medicine ClerkingDocument28 pagesMedicine ClerkingtemitopeNo ratings yet
- S O C R A T E S: History TakingDocument5 pagesS O C R A T E S: History Takingsnanan100% (1)
- History and Physical Exam For COPDDocument2 pagesHistory and Physical Exam For COPDKarenJulioNo ratings yet
- BreathlessnessDocument29 pagesBreathlessnessRajveerNo ratings yet
- History and Physical ExamDocument5 pagesHistory and Physical ExamAnastasia TjanNo ratings yet
- History Taking of Respiratory SystemDocument24 pagesHistory Taking of Respiratory SystemNadiya Elfira BilqisNo ratings yet
- Pedia WW Patient AmDocument32 pagesPedia WW Patient AmSam Raven AndresNo ratings yet
- 22 Long Cases in Medicine by Shamol Sir PDFDocument259 pages22 Long Cases in Medicine by Shamol Sir PDFHossain Muhammad80% (5)
- Respiratory Illnesses in ChildrenDocument42 pagesRespiratory Illnesses in ChildrenJakeNo ratings yet
- Modul Skill Lab!Document46 pagesModul Skill Lab!Imanuel SoniNo ratings yet
- Common General Practice Consultations Notes For OSCEsDocument52 pagesCommon General Practice Consultations Notes For OSCEsNadia SalwaniNo ratings yet
- Health History QuestionnaireDocument5 pagesHealth History QuestionnairegmanistaNo ratings yet
- Aap MCQ 2007-1Document71 pagesAap MCQ 2007-1Ammad Ali JaskaniNo ratings yet
- Medicine 250 Interactive Integrative Case Based Session Study Guide For StudentsDocument1 pageMedicine 250 Interactive Integrative Case Based Session Study Guide For StudentsBA OngNo ratings yet
- Pulmo AxDocument16 pagesPulmo AxPaula Grace MorfeNo ratings yet
- Admitting Conference: Bantasan, Anna Lee Clinical ClerkDocument63 pagesAdmitting Conference: Bantasan, Anna Lee Clinical ClerkAnna Lee BantasanNo ratings yet
- Health History ReportDocument8 pagesHealth History ReportHenrick LamandoNo ratings yet
- Clerking GuideDocument48 pagesClerking GuideAharauka ChiedozieNo ratings yet
- Lecture 11 History TakingDocument6 pagesLecture 11 History Takingpxb8dhqgs9No ratings yet
- OSCE Paeds Master Sheet Rachel AlbertDocument26 pagesOSCE Paeds Master Sheet Rachel AlbertVahni SamarooNo ratings yet
- Chapter 017Document21 pagesChapter 017api-3697326No ratings yet
- Preparation For Paces: HistoryDocument37 pagesPreparation For Paces: HistoryalaaNo ratings yet
- Approach To Child With WheezingpediatricsDocument25 pagesApproach To Child With WheezingpediatricsshahinaNo ratings yet
- Bec BreathingDocument78 pagesBec Breathingasalizwa ludlalaNo ratings yet
- Lecture 3Document39 pagesLecture 3shahadkudNo ratings yet
- Choronic Cough CmeDocument39 pagesChoronic Cough CmeVissalini JayabalanNo ratings yet
- Respiratory Osce: AMSA Edinburgh X IMU Y4Document34 pagesRespiratory Osce: AMSA Edinburgh X IMU Y4Abby LiewNo ratings yet
- Cough: Diagnosis and ManagementDocument65 pagesCough: Diagnosis and Managementsonu_23No ratings yet
- Common General Practice Consultations - Notes For OSCEsDocument54 pagesCommon General Practice Consultations - Notes For OSCEshaydenfarquhar89% (9)
- BEC Module 3 Part 1Document26 pagesBEC Module 3 Part 1colorred818No ratings yet
- History Taking: Dr.H.N.Sarker MBBS, FCPS, Macp (Usa), MRCP (London)Document25 pagesHistory Taking: Dr.H.N.Sarker MBBS, FCPS, Macp (Usa), MRCP (London)ARINDAM CHOWDHURYNo ratings yet
- NCM 112 Care of Clients With Problems in Oxygenation, Fluid and Electrolytes, Infectious, Inflammatory & Immunologic ReactionDocument52 pagesNCM 112 Care of Clients With Problems in Oxygenation, Fluid and Electrolytes, Infectious, Inflammatory & Immunologic ReactionJIMENEZ, TRISHA MARIE D.100% (1)
- Resp Lecture FinalDocument37 pagesResp Lecture Finalapi-195799092No ratings yet
- Respiratory System History Taking: Dr. Aiman Al ShareiDocument20 pagesRespiratory System History Taking: Dr. Aiman Al ShareiQusai IbraheemNo ratings yet
- Looking Back: A Case Presentation On Spinal TuberculosisDocument16 pagesLooking Back: A Case Presentation On Spinal TuberculosisArt GonzalesNo ratings yet
- Claas Mowers Disco 3600 F Disco 3500 FRC Assembly Instruction FR de en RuDocument23 pagesClaas Mowers Disco 3600 F Disco 3500 FRC Assembly Instruction FR de en Rumarkrush140898asj100% (89)
- Chapter 4 ParasitologyDocument35 pagesChapter 4 ParasitologyJuancho OsorioNo ratings yet
- CBLA (Cardiac Patient)Document10 pagesCBLA (Cardiac Patient)Llewelyn AgpaoaNo ratings yet
- FitriDHP - Cardiomegaly Dan Efusion PericardiumDocument40 pagesFitriDHP - Cardiomegaly Dan Efusion PericardiumIlham PrayogoNo ratings yet
- Materials MSDSGold MSDSVendors 2021 February 16 00-46-49-831 AM1Document260 pagesMaterials MSDSGold MSDSVendors 2021 February 16 00-46-49-831 AM1Rani NoumanNo ratings yet
- Laboratory 3Document6 pagesLaboratory 3Mariel CaylanNo ratings yet
- PHP2018Document25 pagesPHP2018radu nicolaeNo ratings yet
- Etextbook 978 0323354097 Understanding Pathophysiology 6th EditionDocument61 pagesEtextbook 978 0323354097 Understanding Pathophysiology 6th Editioneric.chandler298100% (45)
- 13 Approved Herbal Plants From DOHDocument2 pages13 Approved Herbal Plants From DOHRIK HAROLD GATPANDANNo ratings yet
- Anxiolytics and AntidepressantsDocument271 pagesAnxiolytics and AntidepressantsAmir PeljtoNo ratings yet
- Drug Name Classification Mechanism of Action Indication Contraindication Nursing Responsibilities Generic Name CVDocument3 pagesDrug Name Classification Mechanism of Action Indication Contraindication Nursing Responsibilities Generic Name CVDuchess Juliane Jose MirambelNo ratings yet
- Clinical Practice GuidelinesDocument99 pagesClinical Practice GuidelinesKersti Marzo100% (1)
- Public Safety Plan DocumentDocument7 pagesPublic Safety Plan DocumentPoblacion 04 San LuisNo ratings yet
- L4 U03 LA RC - DecryptedDocument3 pagesL4 U03 LA RC - Decryptedkrkshkn100% (1)
- Comprehensive H&PDocument2 pagesComprehensive H&PjwwisnerNo ratings yet
- Intern Journal reading-MRI-osteomyelitis-OOOE-2008Document6 pagesIntern Journal reading-MRI-osteomyelitis-OOOE-2008yuni madjidNo ratings yet
- InvertebratesDocument46 pagesInvertebratesIvy Mae ArnaizNo ratings yet
- Classification of Infectious DiseaseDocument64 pagesClassification of Infectious DiseaseSaadTamNo ratings yet
- RHINOSINSITISDocument2 pagesRHINOSINSITISSharmin ForondaNo ratings yet
- Mech-5-20-JSA - Activity For Erection of ScaffoldingDocument10 pagesMech-5-20-JSA - Activity For Erection of ScaffoldingNasrullah JanNo ratings yet
- Module 3 Nursing Skills Procedure On GI, Endo-Metab Concept (B)Document19 pagesModule 3 Nursing Skills Procedure On GI, Endo-Metab Concept (B)Nashebah A. BatuganNo ratings yet
- Non Hodgkins LymphomaDocument36 pagesNon Hodgkins LymphomaJohn Paul DalayoanNo ratings yet
- AnemiaDocument2 pagesAnemiaLazeh MeNo ratings yet
- Anatomy QBank EMRCSDocument117 pagesAnatomy QBank EMRCSTowhid HasanNo ratings yet
- Derma Trans Clerks Review 2019Document22 pagesDerma Trans Clerks Review 2019anonymousNo ratings yet
- Rapid Review For The Plastic Surgery Inservice & Board ExaminationsDocument183 pagesRapid Review For The Plastic Surgery Inservice & Board ExaminationsTahaniNo ratings yet
- Public Health Science Nursing Practice Savage Kub Grove Test BankDocument29 pagesPublic Health Science Nursing Practice Savage Kub Grove Test BankShelly JonesNo ratings yet
- Class IX-Chapter 13-Why Do We Fall IllDocument36 pagesClass IX-Chapter 13-Why Do We Fall IllPriyanshu choubeyNo ratings yet
- Week 13 Check Your Understanding A. Use Your Notes. Answer The Questions Based On The LectureDocument2 pagesWeek 13 Check Your Understanding A. Use Your Notes. Answer The Questions Based On The LectureIrem YilmazNo ratings yet
- Somatoform DisorderDocument30 pagesSomatoform DisorderRujuta BaramateNo ratings yet