You might also like
- Eye Annual Highlights 2022Document6 pagesEye Annual Highlights 2022Someonelse47No ratings yet
- 053-013 - Anhang A Leitliniensynopsis - Akuter Und Chronischer Husten - FinalDocument11 pages053-013 - Anhang A Leitliniensynopsis - Akuter Und Chronischer Husten - FinalSomeonelse47No ratings yet
- DEGAM LL Muedigkeit 2023 ENG KurzDocument1 pageDEGAM LL Muedigkeit 2023 ENG KurzSomeonelse47No ratings yet
- BSLFRF Compliance and Reporting GuidanceDocument50 pagesBSLFRF Compliance and Reporting GuidanceSomeonelse47No ratings yet
- WHO Guidelines On Parenting Interventions To Prevent Maltreatment and Enhance Parent-Child Relationships With Children Aged 0-17 YearsDocument70 pagesWHO Guidelines On Parenting Interventions To Prevent Maltreatment and Enhance Parent-Child Relationships With Children Aged 0-17 YearsSomeonelse47No ratings yet
- TMTF Report 2Document13 pagesTMTF Report 2Someonelse47No ratings yet
- Technical Consultation To Assess Evidence On Community-Based Delivery of Intermittent Preventive Treatment in Pregnancy For MalariaDocument52 pagesTechnical Consultation To Assess Evidence On Community-Based Delivery of Intermittent Preventive Treatment in Pregnancy For MalariaSomeonelse47No ratings yet
- BSLFRF Final Rule WebinarDocument25 pagesBSLFRF Final Rule WebinarSomeonelse47No ratings yet
- CACEE Report User GuideDocument9 pagesCACEE Report User GuideSomeonelse47No ratings yet
- CNEU Non UGLG Agreements and Supporting DocumentsDocument15 pagesCNEU Non UGLG Agreements and Supporting DocumentsSomeonelse47No ratings yet
- BTitle VI AssurancesDocument3 pagesBTitle VI AssurancesSomeonelse47No ratings yet
- CJuly 2022 PE Report User GuideDocument142 pagesCJuly 2022 PE Report User GuideSomeonelse47No ratings yet
- CApril 2022 PE Report User GuideDocument119 pagesCApril 2022 PE Report User GuideSomeonelse47No ratings yet
- NEU Checklist For Requesting Initial PaymentDocument2 pagesNEU Checklist For Requesting Initial PaymentSomeonelse47No ratings yet
- List of Local GovernmentsDocument1,797 pagesList of Local GovernmentsSomeonelse47No ratings yet
- Federal Register / Vol. 87, No. 18 / Thursday, January 27, 2022 / Rules and RegulationsDocument117 pagesFederal Register / Vol. 87, No. 18 / Thursday, January 27, 2022 / Rules and RegulationsSomeonelse47No ratings yet
- ASLFRF Final Rule OverviewDocument44 pagesASLFRF Final Rule OverviewSomeonelse47No ratings yet
- NEU Award Terms and ConditionsDocument5 pagesNEU Award Terms and ConditionsSomeonelse47No ratings yet
- TalDocument1 pageTalSomeonelse47No ratings yet
- Status State NEU DistributionDocument3 pagesStatus State NEU DistributionSomeonelse47No ratings yet
- OlxDocument2 pagesOlxSomeonelse47No ratings yet
- NEU GuidanceDocument8 pagesNEU GuidanceSomeonelse47No ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- TCPS 2 - Core-2022Document2 pagesTCPS 2 - Core-2022Roshan PatelNo ratings yet
- Different Perspectives in PsychologyDocument23 pagesDifferent Perspectives in PsychologyChicki ChandwaniNo ratings yet
- Natural Cancer Remedies That WorkDocument48 pagesNatural Cancer Remedies That WorkAlessio Anam100% (1)
- Let'S Do This!: Activity 1 Lifestyle EvaluationDocument2 pagesLet'S Do This!: Activity 1 Lifestyle EvaluationracmaNo ratings yet
- Pranayama Yoga The Ultimate Guide For EveryoneDocument8 pagesPranayama Yoga The Ultimate Guide For Everyoneshiv yogaNo ratings yet
- Expository Cause & Effect EssayDocument2 pagesExpository Cause & Effect EssayAutoDefenceNo ratings yet
- Tonic-Clonic Seizure?: SymptomsDocument3 pagesTonic-Clonic Seizure?: SymptomsMaria Jessica DumdumNo ratings yet
- UN B. Inggris-2009Document13 pagesUN B. Inggris-2009fitriNo ratings yet
- Contribution of Sociology in MedicineDocument11 pagesContribution of Sociology in Medicinelaiba imtiazNo ratings yet
- Professional Nursing ValuesDocument11 pagesProfessional Nursing ValuesAzra BalochNo ratings yet
- Common Errors-1Document12 pagesCommon Errors-1Sama N SamirNo ratings yet
- QUIZDocument2 pagesQUIZroelNo ratings yet
- What Is XBX?: Same Order, and in The Same Maximum Time LimitDocument2 pagesWhat Is XBX?: Same Order, and in The Same Maximum Time LimitMohammad IslamNo ratings yet
- Reflection in CosmetologyDocument3 pagesReflection in CosmetologyMaria CeciliaNo ratings yet
- Respiratory Module 4 8Document11 pagesRespiratory Module 4 8David Dwane Art SilorioNo ratings yet
- Chapter 3, Unit 1, Social and Preventive Pharmacy, B Pharmacy 8th Sem, Carewell PharmaDocument5 pagesChapter 3, Unit 1, Social and Preventive Pharmacy, B Pharmacy 8th Sem, Carewell Pharmasasimadurai1975No ratings yet
- 4.4 Keeping A Fetus HealthyDocument12 pages4.4 Keeping A Fetus HealthyhypezakramNo ratings yet
- Stanley Milgram Case StudyDocument4 pagesStanley Milgram Case StudyJonathan JohnsonNo ratings yet
- PerfectionismDocument15 pagesPerfectionismNatacha Cabete100% (1)
- City Bantay Asin TaskDocument1 pageCity Bantay Asin TaskBob JoeNo ratings yet
- Gathering Instrument For TraineeDocument4 pagesGathering Instrument For TraineeArnold M. MendozaNo ratings yet
- Course Syllabus Guide Fundamentals of Nutrition - ALLH 220 3 CreditsDocument7 pagesCourse Syllabus Guide Fundamentals of Nutrition - ALLH 220 3 CreditsEm JayNo ratings yet
- Gano Massage Oil - English - Malaysia - v2Document13 pagesGano Massage Oil - English - Malaysia - v2bigjebatNo ratings yet
- LESSON PLAN Health Lesson PlanDocument2 pagesLESSON PLAN Health Lesson PlanSusie Hauchab ChalitaNo ratings yet
- ScheduleDocument2 pagesScheduleMax SaubermanNo ratings yet
- Accuracy and Validity of HbA1c POCT Report - August 2020Document86 pagesAccuracy and Validity of HbA1c POCT Report - August 2020Iura FlorinNo ratings yet
- Department of Comprensive Nurse Department of Comprensive NurseDocument22 pagesDepartment of Comprensive Nurse Department of Comprensive NurseAmir AbdiNo ratings yet
- ConditionalsDocument3 pagesConditionalsvojaradNo ratings yet
- CF Host Dept List 2023 24 v12Document111 pagesCF Host Dept List 2023 24 v12Antal Dorin CristianNo ratings yet
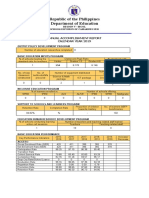
- Republic of The Philippines Department of Education: Annual Accomplishment Report Calendar Year 2019Document4 pagesRepublic of The Philippines Department of Education: Annual Accomplishment Report Calendar Year 2019sheareign dainchylles gamayanNo ratings yet