You might also like
- JSA FOR ROAD LAYING WORK (Asphalt Paving)Document10 pagesJSA FOR ROAD LAYING WORK (Asphalt Paving)wahyu nugroho86% (7)
- Final NCP HerniaDocument5 pagesFinal NCP HerniaDenisse Shazz Mae Maret100% (2)
- Postconcussion SyndromeDocument16 pagesPostconcussion SyndromeonaNo ratings yet
- Lesson Plan DepressionDocument19 pagesLesson Plan DepressionRahul Kumar Diwakar100% (1)
- Sleep Deprivation and Academic Performance Among Senior High School Students of UM Digos CollegeDocument11 pagesSleep Deprivation and Academic Performance Among Senior High School Students of UM Digos CollegeMarc Ian Dela Peña75% (4)
- 7 Enemies of SurvivalDocument2 pages7 Enemies of SurvivalNasri Bin Rifin100% (1)
- Phobic Postural Vertigo: A Cognitive-Behavior ApproachDocument2 pagesPhobic Postural Vertigo: A Cognitive-Behavior ApproachVa RissaNo ratings yet
- The First Nursing School in The Philippines, 1906: Nursing@cpu - Edu.phDocument9 pagesThe First Nursing School in The Philippines, 1906: Nursing@cpu - Edu.phKoleen Lhyte T. UYNo ratings yet
- Depression Lets TalkDocument68 pagesDepression Lets TalkImon PaulNo ratings yet
- Major Depression - Dysthymic DisorderDocument27 pagesMajor Depression - Dysthymic DisorderCay SevillaNo ratings yet
- Anxiety and Panic DisordersDocument6 pagesAnxiety and Panic DisordersNo OneNo ratings yet
- Generalized Anxiety Disorder: by William A. Kehoe, Pharm.D., MA, FCCP, BCPSDocument21 pagesGeneralized Anxiety Disorder: by William A. Kehoe, Pharm.D., MA, FCCP, BCPSAgungPermataNo ratings yet
- Mood Disorders2Document73 pagesMood Disorders2Crisia GungobNo ratings yet
- Pshciatry in BriefDocument18 pagesPshciatry in BriefSelim TarekNo ratings yet
- Anxiety GAD ACSAP 2017 StudentDocument18 pagesAnxiety GAD ACSAP 2017 StudentRenaldi KristianNo ratings yet
- Psychosomatic Dis PediatricsDocument7 pagesPsychosomatic Dis PediatricsLuiza AbreuNo ratings yet
- Major Depression - Dysthymic DisorderDocument28 pagesMajor Depression - Dysthymic Disorderapi-3797941No ratings yet
- Somatization: Diagnosing It Sooner Through Emotion-Focused InterviewingDocument10 pagesSomatization: Diagnosing It Sooner Through Emotion-Focused Interviewingscribd4kmhNo ratings yet
- Chronic Fatigue Syndrome.Document3 pagesChronic Fatigue Syndrome.jagdeepNo ratings yet
- Mental Health DisordersDocument7 pagesMental Health DisorderskgjtertijNo ratings yet
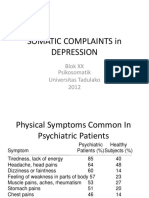
- Somatic Complaints in Depression Psikosomatik Untad 2012Document19 pagesSomatic Complaints in Depression Psikosomatik Untad 2012Muhammad mukramNo ratings yet
- Beyond Sadness PowerpointDocument12 pagesBeyond Sadness PowerpointJoanne BlancoNo ratings yet
- Depression Ad Cerebral PalsyDocument2 pagesDepression Ad Cerebral PalsyReinhaMaeDaduyaNo ratings yet
- Depression: May) Fall (September To November)Document5 pagesDepression: May) Fall (September To November)Dhen MarcNo ratings yet
- Mood Disorders SuicideDocument67 pagesMood Disorders Suicidethe lousy donutNo ratings yet
- Pain Perception and ManagementDocument3 pagesPain Perception and ManagementAlec Xavier MirandaNo ratings yet
- Somatic Symptom and Related Disorders and Dissociative DisordersDocument3 pagesSomatic Symptom and Related Disorders and Dissociative DisordersCalli AndersonNo ratings yet
- Depressive Disorders Mood DisorderDocument20 pagesDepressive Disorders Mood DisorderJade CentinoNo ratings yet
- Neurological AssessmentDocument10 pagesNeurological AssessmentmatsumotoNo ratings yet
- Stress MX in CapfDocument36 pagesStress MX in CapfHemant KatariaNo ratings yet
- Anxiety and Anxiety Disorders - RosalesDocument12 pagesAnxiety and Anxiety Disorders - RosalesDacillo GailleNo ratings yet
- Nelson en Ingles Capitulos 16 A 20Document81 pagesNelson en Ingles Capitulos 16 A 20Mario TurichNo ratings yet
- Agot Rle Case Study 3Document17 pagesAgot Rle Case Study 3Angel May P AgotNo ratings yet
- Reaction To Severe Stress and Adjustment DisorderDocument22 pagesReaction To Severe Stress and Adjustment DisorderTulika SarkarNo ratings yet
- Family Medicine FinalDocument90 pagesFamily Medicine FinalPeter MichaelNo ratings yet
- ModuleC - Lesson 4 - Gr11Document16 pagesModuleC - Lesson 4 - Gr11Tutti AmoresNo ratings yet
- Unipolar DepressionDocument21 pagesUnipolar DepressionJingen maNo ratings yet
- Advanced Abnormal Psychology: (Somatic Symptoms and Related Disorders)Document19 pagesAdvanced Abnormal Psychology: (Somatic Symptoms and Related Disorders)Rosemary LandanNo ratings yet
- Mild Depressive TreatmentDocument5 pagesMild Depressive Treatmentpan donNo ratings yet
- Clinical Psychology: Mood Disorders: What Is Abnormality?Document6 pagesClinical Psychology: Mood Disorders: What Is Abnormality?Alexandra Adina RădescuNo ratings yet
- MHN 17Document14 pagesMHN 17Vaishali SinghNo ratings yet
- DepressionDocument3 pagesDepressionPolash RoyNo ratings yet
- Duloxetina 3Document10 pagesDuloxetina 3Robert MovileanuNo ratings yet
- Major Depression Disorder: Mars Hervie S. Cuchapin, RPH NeurologyDocument8 pagesMajor Depression Disorder: Mars Hervie S. Cuchapin, RPH NeurologyLoren SangalangNo ratings yet
- Depressive EpisodeDocument33 pagesDepressive EpisodeKp ANo ratings yet
- Exam 1 BlueprintDocument6 pagesExam 1 BlueprintMindiNo ratings yet
- Ies RDocument2 pagesIes RJohn PrestonNo ratings yet
- Pain Management For NursesDocument42 pagesPain Management For Nursesblacknurse100% (1)
- (PSYCH) Neurocognitive DisordersDocument14 pages(PSYCH) Neurocognitive DisordersThesa TagalogNo ratings yet
- برزنتيشن هديك١Document22 pagesبرزنتيشن هديك١Abdallah AlquranNo ratings yet
- Department of Family Medicine Fpe Headache Syndrome: - Vanaveera Pandian SwethaDocument106 pagesDepartment of Family Medicine Fpe Headache Syndrome: - Vanaveera Pandian SwethaSuba Saravanan 12No ratings yet
- 269 - PPT Modul 3Document18 pages269 - PPT Modul 3NirwanaNo ratings yet
- N11 Nursing Foundations IiDocument4 pagesN11 Nursing Foundations IiAlec Xavier MirandaNo ratings yet
- 3 Somatic and DissociativeDocument7 pages3 Somatic and DissociativeMarian AlinoodNo ratings yet
- Chapter 7Document8 pagesChapter 7Ellyza EvangelistaNo ratings yet
- 3-Anxiety DisordersDocument57 pages3-Anxiety DisordersVidya BalaNo ratings yet
- Chapter 7 Mood DisordersDocument47 pagesChapter 7 Mood DisordersAngela Abigail AbingNo ratings yet
- Neurologic Evaluation DR TsionDocument100 pagesNeurologic Evaluation DR Tsionzelalemmekonnen823No ratings yet
- Abram Hoffer - Prousky - Orthomolecular Treatment of Anxiety DisordersDocument7 pagesAbram Hoffer - Prousky - Orthomolecular Treatment of Anxiety DisordersEbook PDFNo ratings yet
- ABNORMAL PSYCHOLOGY (Chapters 1-7)Document35 pagesABNORMAL PSYCHOLOGY (Chapters 1-7)Fiona Zoe AbellaNo ratings yet
- Calm and Centered: Overcoming Anxiety and Panic Attacks NaturallyFrom EverandCalm and Centered: Overcoming Anxiety and Panic Attacks NaturallyNo ratings yet
- How to Fight Depression - 9 Case Studies: Self-Help Series, #2From EverandHow to Fight Depression - 9 Case Studies: Self-Help Series, #2Rating: 4 out of 5 stars4/5 (1)
- DEGAM LL Schlaganfall EN Kurz RZ 25820Document2 pagesDEGAM LL Schlaganfall EN Kurz RZ 25820Someonelse47No ratings yet
- DEGAM LL Schlaganfall EN Kurz RZ 25820Document2 pagesDEGAM LL Schlaganfall EN Kurz RZ 25820Someonelse47No ratings yet
- 053-013 - Anhang A Leitliniensynopsis - Akuter Und Chronischer Husten - FinalDocument11 pages053-013 - Anhang A Leitliniensynopsis - Akuter Und Chronischer Husten - FinalSomeonelse47No ratings yet
- TMTF Report 2Document13 pagesTMTF Report 2Someonelse47No ratings yet
- Technical Consultation To Assess Evidence On Community-Based Delivery of Intermittent Preventive Treatment in Pregnancy For MalariaDocument52 pagesTechnical Consultation To Assess Evidence On Community-Based Delivery of Intermittent Preventive Treatment in Pregnancy For MalariaSomeonelse47No ratings yet
- Eye Annual Highlights 2022Document6 pagesEye Annual Highlights 2022Someonelse47No ratings yet
- WHO Guidelines On Parenting Interventions To Prevent Maltreatment and Enhance Parent-Child Relationships With Children Aged 0-17 YearsDocument70 pagesWHO Guidelines On Parenting Interventions To Prevent Maltreatment and Enhance Parent-Child Relationships With Children Aged 0-17 YearsSomeonelse47No ratings yet
- BTitle VI AssurancesDocument3 pagesBTitle VI AssurancesSomeonelse47No ratings yet
- NEU GuidanceDocument8 pagesNEU GuidanceSomeonelse47No ratings yet
- BSLFRF Compliance and Reporting GuidanceDocument50 pagesBSLFRF Compliance and Reporting GuidanceSomeonelse47No ratings yet
- CJuly 2022 PE Report User GuideDocument142 pagesCJuly 2022 PE Report User GuideSomeonelse47No ratings yet
- CNEU Non UGLG Agreements and Supporting DocumentsDocument15 pagesCNEU Non UGLG Agreements and Supporting DocumentsSomeonelse47No ratings yet
- CApril 2022 PE Report User GuideDocument119 pagesCApril 2022 PE Report User GuideSomeonelse47No ratings yet
- CACEE Report User GuideDocument9 pagesCACEE Report User GuideSomeonelse47No ratings yet
- BSLFRF Final Rule WebinarDocument25 pagesBSLFRF Final Rule WebinarSomeonelse47No ratings yet
- NEU Award Terms and ConditionsDocument5 pagesNEU Award Terms and ConditionsSomeonelse47No ratings yet
- NEU Checklist For Requesting Initial PaymentDocument2 pagesNEU Checklist For Requesting Initial PaymentSomeonelse47No ratings yet
- List of Local GovernmentsDocument1,797 pagesList of Local GovernmentsSomeonelse47No ratings yet
- ASLFRF Final Rule OverviewDocument44 pagesASLFRF Final Rule OverviewSomeonelse47No ratings yet
- OlxDocument2 pagesOlxSomeonelse47No ratings yet
- Status State NEU DistributionDocument3 pagesStatus State NEU DistributionSomeonelse47No ratings yet
- Federal Register / Vol. 87, No. 18 / Thursday, January 27, 2022 / Rules and RegulationsDocument117 pagesFederal Register / Vol. 87, No. 18 / Thursday, January 27, 2022 / Rules and RegulationsSomeonelse47No ratings yet
- TalDocument1 pageTalSomeonelse47No ratings yet
- World Health Organization (WHO) Analgesic LadderDocument1 pageWorld Health Organization (WHO) Analgesic LadderPaula Nakamura GläserNo ratings yet
- Module 1Document190 pagesModule 1Zheen JawadNo ratings yet
- The Dog Hyde Was Left Behind Cause His Owner Matt Wanted A CatDocument1 pageThe Dog Hyde Was Left Behind Cause His Owner Matt Wanted A CatSomeonelse47No ratings yet
- The Constitution of The United StatesDocument21 pagesThe Constitution of The United StatesJeff PrattNo ratings yet
- WHO Guideline On The Prevention of DrowningDocument124 pagesWHO Guideline On The Prevention of DrowningSomeonelse47No ratings yet
- Module 1Document190 pagesModule 1Zheen JawadNo ratings yet
- Ergo ThesisDocument10 pagesErgo ThesisJohnny RamonNo ratings yet
- Pre Game & Post Game RoutinesDocument22 pagesPre Game & Post Game Routinesgelsa dragonNo ratings yet
- NCP For PneumoniaDocument3 pagesNCP For PneumoniaLeogalvez BedanoNo ratings yet
- Cross-Cultural Conflict AdjustmentDocument27 pagesCross-Cultural Conflict Adjustmenttapdew 25No ratings yet
- Tancet Model Question and AnswerDocument16 pagesTancet Model Question and Answerveeramanikandans100% (3)
- Chemo NCPDocument2 pagesChemo NCPJustin Eduardo100% (1)
- Lab ReportDocument3 pagesLab ReportlinziyiNo ratings yet
- Mark HymanDocument14 pagesMark HymanMax meNo ratings yet
- 55 Ways To Get More Energy - Zen HabitsDocument13 pages55 Ways To Get More Energy - Zen HabitsTapan Kumar MohantaNo ratings yet
- Land Transportation Safety Recommended Practice, Journey ManagementDocument22 pagesLand Transportation Safety Recommended Practice, Journey Managementwahyu nugrohoNo ratings yet
- Yoga Sudha Apr 2014Document44 pagesYoga Sudha Apr 2014Belle NgNo ratings yet
- Bài Reading B Sung HP SauDocument23 pagesBài Reading B Sung HP SauTrangNo ratings yet
- Ramadan Safety 2017Document17 pagesRamadan Safety 2017Rajesh MNo ratings yet
- Manda Rag atDocument6 pagesManda Rag atlapNo ratings yet
- Stretch-Shortening Cycle: A Powerful Model To Study Normal and Fatigued MuscleDocument10 pagesStretch-Shortening Cycle: A Powerful Model To Study Normal and Fatigued MuscleNuta Marius AlexandruNo ratings yet
- Physical Assessment For Patient With DM Type1Document4 pagesPhysical Assessment For Patient With DM Type1Mae AzoresNo ratings yet
- UntitledDocument150 pagesUntitledApoorvaNo ratings yet
- Heat IndexDocument2 pagesHeat IndexFrancis Enriquez TanNo ratings yet
- Stress Management NotesDocument15 pagesStress Management NotesYash MittalNo ratings yet
- Chapter 8 - Prosocial Behavior, Cooperation, Conflict and StressDocument15 pagesChapter 8 - Prosocial Behavior, Cooperation, Conflict and StressDiane RossNo ratings yet
- Workplace Health - Nurse Fatigue - StudentDocument47 pagesWorkplace Health - Nurse Fatigue - StudentKimberly AvendanoNo ratings yet
- Đề Thi Khảo Sát Chất Lượng Môn Tiếng AnhDocument50 pagesĐề Thi Khảo Sát Chất Lượng Môn Tiếng AnhVân Minh ThiNo ratings yet
- Fatigue Assessment Scale (FAS)Document2 pagesFatigue Assessment Scale (FAS)Kiss JózsefNo ratings yet
- Physioex Lala PDFDocument5 pagesPhysioex Lala PDFNamira alifahNo ratings yet
- NCP - Alteration in ComfortDocument2 pagesNCP - Alteration in ComfortPatricia CastroNo ratings yet
- Work PhysiologyDocument4 pagesWork PhysiologyMahir MalikNo ratings yet