You might also like
- Patty Brennan Homeopathic GuideDocument54 pagesPatty Brennan Homeopathic Guidepawajee0% (1)
- AAFCO Dog & Cat Nutrient ProfilesDocument5 pagesAAFCO Dog & Cat Nutrient Profilesjimbomack66No ratings yet
- AcndcbdahumanimDocument9 pagesAcndcbdahumanimandrecalfaroNo ratings yet
- Veterinary Drug Formulary2014 English PDFDocument19 pagesVeterinary Drug Formulary2014 English PDFSamuel LamNo ratings yet
- Effects of Zinc and Linoleic Acid Supplementation On The Skin and Coat Quality of Dogs Receiving A Complete and Balanced Diet (PagesDocument8 pagesEffects of Zinc and Linoleic Acid Supplementation On The Skin and Coat Quality of Dogs Receiving A Complete and Balanced Diet (PagesjenNo ratings yet
- FARAD Digest: Extralabel Use of Ivermectin and Moxidectin in Food AnimalsDocument4 pagesFARAD Digest: Extralabel Use of Ivermectin and Moxidectin in Food AnimalsJan SteinmanNo ratings yet
- WALTHAM International Science Symposium: Nature, Nurture, and The Case For NutritionDocument3 pagesWALTHAM International Science Symposium: Nature, Nurture, and The Case For NutritionDafne CoilaNo ratings yet
- bde04180-fff2-466f-8bc5-0a7fce4bb9b0Document11 pagesbde04180-fff2-466f-8bc5-0a7fce4bb9b0Khaleb SeraphimNo ratings yet
- Otter Care Manual 2009 NAG EDITDocument36 pagesOtter Care Manual 2009 NAG EDITMarvin MonterrosoNo ratings yet
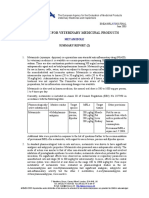
- Metamizole Summary Report 2 Committee Veterinary Medicinal Products enDocument10 pagesMetamizole Summary Report 2 Committee Veterinary Medicinal Products enReni Ika CahyantiNo ratings yet
- Plumb's VDH Errata Landing Page Final - v2Document5 pagesPlumb's VDH Errata Landing Page Final - v2nino.bullonNo ratings yet
- Flubendazole Extension Turkeys Summary Report Committee Veterinary Medicinal Products - enDocument2 pagesFlubendazole Extension Turkeys Summary Report Committee Veterinary Medicinal Products - enAhmed Ali EissaNo ratings yet
- Imidocarb Summary Report 2 Committee Veterinary Medicinal Products enDocument6 pagesImidocarb Summary Report 2 Committee Veterinary Medicinal Products enGilsson FigueroaNo ratings yet
- Chemical Composition of Lipids Isolated From Selected Organs and Tissues of The Raccoon Dog (Nyctereutes Procyonoides)Document7 pagesChemical Composition of Lipids Isolated From Selected Organs and Tissues of The Raccoon Dog (Nyctereutes Procyonoides)phungthuongNo ratings yet
- FEDIAF Reglementari EuropeneDocument9 pagesFEDIAF Reglementari EuropeneAndreiNo ratings yet
- Technical Data Sheet and Trial Protocol - TeamCAT - FINALDocument21 pagesTechnical Data Sheet and Trial Protocol - TeamCAT - FINALLaurenz James De MattaNo ratings yet
- Leptin Secretion in Horses: Effects of Dexamethasone, Gender, and TestosteroneDocument14 pagesLeptin Secretion in Horses: Effects of Dexamethasone, Gender, and TestosteroneLaviniaMenicucciNo ratings yet
- HepatoprotectiveDocument6 pagesHepatoprotectiveSujith KuttanNo ratings yet
- 12 Perkembangan Sistem Pencernaan Pernafasan 2011Document20 pages12 Perkembangan Sistem Pencernaan Pernafasan 2011Fauzi ChandraNo ratings yet
- 2004 Lebas WRC Revue Sources Matiere Premieres PueblaDocument51 pages2004 Lebas WRC Revue Sources Matiere Premieres PueblaCarlos DiazNo ratings yet
- Nutritional Management of Equine Diseases and Special CasesFrom EverandNutritional Management of Equine Diseases and Special CasesBryan M. WaldridgeNo ratings yet
- Eline Paediatric Medicine: Clinical Nutrition in KittensDocument12 pagesEline Paediatric Medicine: Clinical Nutrition in KittensNarcisa Zambrano Loor MVZNo ratings yet
- Professional Diploma in Sports Nutrition: Lesson 7Document28 pagesProfessional Diploma in Sports Nutrition: Lesson 7Jomari ServanoNo ratings yet
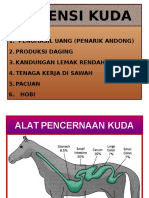
- Pakan KudaDocument20 pagesPakan KudaAndini NurfitrieNo ratings yet
- BhringrajDocument5 pagesBhringrajAmit patelNo ratings yet
- Feeding Dogs: Taxonomic ClassificationDocument8 pagesFeeding Dogs: Taxonomic Classificationfreak009No ratings yet
- The Carnivore Connection To Nutrition in Cats - Feeding Your CatDocument0 pagesThe Carnivore Connection To Nutrition in Cats - Feeding Your CatringpieceNo ratings yet
- Large RuminantDocument36 pagesLarge RuminantMelynda KartjitoNo ratings yet
- Chapter Three: Maned Wolf Nutritional ManagementDocument5 pagesChapter Three: Maned Wolf Nutritional ManagementCarolyne Assis Eigenheer Pinke TestaNo ratings yet
- Badiang Chapter 4 (Latest)Document9 pagesBadiang Chapter 4 (Latest)Alna JaeNo ratings yet
- Product Portofolio Powder Line AminoMaxDocument12 pagesProduct Portofolio Powder Line AminoMaxMohamed GhalebNo ratings yet
- 12 2012 TriclabendazoleDocument16 pages12 2012 Triclabendazolenia suwartiningsihNo ratings yet
- Copy 6Document3 pagesCopy 6Putri NafrianiiNo ratings yet
- Glyph Os AteDocument91 pagesGlyph Os Atejose robledoNo ratings yet
- Formulation of Dog Food Using Locally Available IngredientsDocument5 pagesFormulation of Dog Food Using Locally Available Ingredientsarmaan aliNo ratings yet
- Equine Production AND Health Management: College of Veterinary MedicineDocument14 pagesEquine Production AND Health Management: College of Veterinary MedicineHermione MalfoyNo ratings yet
- Course: B.V.SC &A.H.: Soluble Non-Starch PolysachharidesDocument7 pagesCourse: B.V.SC &A.H.: Soluble Non-Starch Polysachharideskushal NeupaneNo ratings yet
- Effects of Multi-Enzyme Supplementation On Nutrient Digestibility in Broiler ChickensDocument6 pagesEffects of Multi-Enzyme Supplementation On Nutrient Digestibility in Broiler ChickensOliver TalipNo ratings yet
- Anxiolytic Activity of Fennel Fruit Soxhlet in MiceDocument3 pagesAnxiolytic Activity of Fennel Fruit Soxhlet in MiceOthman JerbiNo ratings yet
- Aafco Methods For Substantiating Nutritional Adequacy of Dog and Cat FoodsDocument24 pagesAafco Methods For Substantiating Nutritional Adequacy of Dog and Cat FoodsShahzad AshrafNo ratings yet
- AAFCO Nutrient ProfilesDocument24 pagesAAFCO Nutrient Profilesdoc brownNo ratings yet
- Rat, Mice and Guinea Pig FeedingDocument32 pagesRat, Mice and Guinea Pig Feeding1938 MANOJ R BHARADWAJNo ratings yet
- Nutrients: Krill Products: An Overview of Animal StudiesDocument22 pagesNutrients: Krill Products: An Overview of Animal StudiesAlbert EdoNo ratings yet
- Pyrantel Embonate Summary Report Committee Veterinary Medicinal Products enDocument4 pagesPyrantel Embonate Summary Report Committee Veterinary Medicinal Products enkrisniatiNo ratings yet
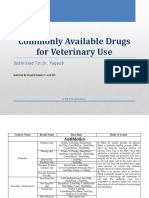
- Commonly Available Drugs For Veterinary Use: Submitted To: Dr. YaqoobDocument21 pagesCommonly Available Drugs For Veterinary Use: Submitted To: Dr. YaqoobUbaid HassanNo ratings yet
- Committee For Veterinary Medicinal Products: Summary ReportDocument9 pagesCommittee For Veterinary Medicinal Products: Summary ReportNatasha ImanuelleNo ratings yet
- Influence of Feed Intake On Blood Chemistry Parameters in Kacang GoatsDocument4 pagesInfluence of Feed Intake On Blood Chemistry Parameters in Kacang GoatsHazim Azmi Al-QadryNo ratings yet
- Fenpipramide Hydrochloride Summary Report Committee Veterinary Medicinal Products - en PDFDocument2 pagesFenpipramide Hydrochloride Summary Report Committee Veterinary Medicinal Products - en PDFAdriana TrandafirNo ratings yet
- LipDocument2 pagesLiphazel100% (2)
- Intake of Minerals Trace Elements and Vitamins in Bone and Raw Food Rations in Adult DogsDocument4 pagesIntake of Minerals Trace Elements and Vitamins in Bone and Raw Food Rations in Adult DogsKarl MedinaNo ratings yet
- Kalori SUFORDocument9 pagesKalori SUFORmarselyagNo ratings yet
- Final Paper For NSAP 2020 by Saheed SaobanDocument4 pagesFinal Paper For NSAP 2020 by Saheed SaobanSaheed SaobanNo ratings yet
- Fascetti, 2010 - Nutritional Management and Disease Prevention in Healthy Dogs and CatsDocument10 pagesFascetti, 2010 - Nutritional Management and Disease Prevention in Healthy Dogs and CatsLetícia PachecoNo ratings yet
- Nutrition - General Feeding Guidelines For DogsDocument5 pagesNutrition - General Feeding Guidelines For DogsFlorin B.No ratings yet
- Potassium BromideDocument2 pagesPotassium Bromidetaner_soysuren100% (1)
- Protein and Amino AcidsDocument11 pagesProtein and Amino AcidsArpit AmitansuNo ratings yet
- Nutrigenomic Study: Igf-1 Inhibition in Adipogenesis of Visceral Adipose Tissue of Rat Using Rambutan Peel ExtractDocument2 pagesNutrigenomic Study: Igf-1 Inhibition in Adipogenesis of Visceral Adipose Tissue of Rat Using Rambutan Peel ExtractlarasatiNo ratings yet
- 1b - DiabetesDocument102 pages1b - DiabetesNelson Quispe MaraniNo ratings yet
- Nutrient Requirement For Cattle and BuffaloeDocument31 pagesNutrient Requirement For Cattle and BuffaloeSHYLESH BNo ratings yet
- Performance of Free-Range Broiler ChickensDocument8 pagesPerformance of Free-Range Broiler ChickensOliver TalipNo ratings yet
- Canine Nutrition: And Performance, Medical Issues, Lifestages, Ethical Considerations, and MoreFrom EverandCanine Nutrition: And Performance, Medical Issues, Lifestages, Ethical Considerations, and MoreRating: 5 out of 5 stars5/5 (1)
- Caso Clinico CompressedDocument18 pagesCaso Clinico CompressedNatalia BarbosaNo ratings yet
- Ishak 2020Document11 pagesIshak 2020Natalia BarbosaNo ratings yet
- Först 2003 Persistent-Anovulatory-Follicles-In-The-MareDocument3 pagesFörst 2003 Persistent-Anovulatory-Follicles-In-The-MareNatalia BarbosaNo ratings yet
- Speaking Exam Level Vi 40Document2 pagesSpeaking Exam Level Vi 40Natalia BarbosaNo ratings yet
- Module 7 Taking Vital SignsDocument7 pagesModule 7 Taking Vital SignsMary Joy CejalboNo ratings yet
- Health Assessment Made Incredibly Visual Incredibly Easy Series 2nd Edition PDFDrive 9 18Document10 pagesHealth Assessment Made Incredibly Visual Incredibly Easy Series 2nd Edition PDFDrive 9 18mianpenarandaNo ratings yet
- University of Northern PhilippinesDocument4 pagesUniversity of Northern PhilippinesCatherine PradoNo ratings yet
- About DysphoriaDocument5 pagesAbout DysphoriaCarolina GómezNo ratings yet
- Nitrous Oxide Sedation DentistryDocument16 pagesNitrous Oxide Sedation DentistryAnonymous k8rDEsJsU1100% (1)
- BSC in Neonatal NursingDocument14 pagesBSC in Neonatal NursingsmsmdsdsffNo ratings yet
- Assessment Questions (Assessment Criteria)Document2 pagesAssessment Questions (Assessment Criteria)sujanaNo ratings yet
- Laparoscopic Course: General Principles of Laparoscopy: Specific Aspects of Transperitoneal Access (R.Bollens)Document4 pagesLaparoscopic Course: General Principles of Laparoscopy: Specific Aspects of Transperitoneal Access (R.Bollens)Anuj MisraNo ratings yet
- Adrenal Gland: Bardelosa, Jesse Gale M. Barretto, Alyssa Nicole 3MT1Document88 pagesAdrenal Gland: Bardelosa, Jesse Gale M. Barretto, Alyssa Nicole 3MT1Alyssa Nicole BarrettoNo ratings yet
- Shock SepticDocument35 pagesShock SepticAkbar SyarialNo ratings yet
- What Are NightmaresDocument2 pagesWhat Are NightmaresCharlie BalucanNo ratings yet
- Report ViewerDocument1 pageReport Viewervoldemort killerNo ratings yet
- Daftar Obat Apotek KumaraDocument36 pagesDaftar Obat Apotek Kumaraigd ponekNo ratings yet
- NCP AppendicitisDocument8 pagesNCP AppendicitisAaron_Kim_Vela_4636No ratings yet
- Interpreting Iron StudiesDocument1 pageInterpreting Iron StudiesfahadNo ratings yet
- OSPE DU MedicineDocument101 pagesOSPE DU MedicinesaifNo ratings yet
- Etiology, Classification and Clinical Approach: EndophthalmitisDocument42 pagesEtiology, Classification and Clinical Approach: EndophthalmitisHieLdaJanuariaNo ratings yet
- Tshwane Update 2023 3rd EditionDocument6 pagesTshwane Update 2023 3rd EditionGaming With Mr frostNo ratings yet
- Anesthesia Management For Pulmonary Hypertension PatientsDocument18 pagesAnesthesia Management For Pulmonary Hypertension PatientsAliNasrallahNo ratings yet
- Final Report Sero Survey0409Document160 pagesFinal Report Sero Survey0409BSL-2No ratings yet
- Management of Acne Scarring, Part II: A Comparative Review of Non-Laser-Based, Minimally Invasive ApproachesDocument10 pagesManagement of Acne Scarring, Part II: A Comparative Review of Non-Laser-Based, Minimally Invasive ApproachesShintaNo ratings yet
- Endobutton Family BrochureDocument6 pagesEndobutton Family BrochureRicardo Chaconbenjumea100% (1)
- Tension Pneumothorax: Modifiable FactorsDocument3 pagesTension Pneumothorax: Modifiable FactorsJustin MaverickNo ratings yet
- Practice: Non-Steroidal Anti-Inflammatory Drugs (Nsaids)Document7 pagesPractice: Non-Steroidal Anti-Inflammatory Drugs (Nsaids)Via IndriNo ratings yet
- Knowledge, Attitude and Practice (Kap) Study OnDocument52 pagesKnowledge, Attitude and Practice (Kap) Study OnQazi Muhammad IqbalNo ratings yet
- NifedipineDocument3 pagesNifedipineNovi YulianaNo ratings yet
- Trichuris TrichiuraDocument16 pagesTrichuris TrichiuraPaul Avila SorianoNo ratings yet
- Injury Patterns in Danish Competitive SwimmingDocument5 pagesInjury Patterns in Danish Competitive SwimmingSebastian VicolNo ratings yet
- Diabetic NephropathyDocument10 pagesDiabetic NephropathySindi Nabila PutriNo ratings yet