You might also like
- 06.itinerery in Japan RevisiDocument1 page06.itinerery in Japan RevisiMulia Andara0% (1)
- 3 Jurnal Sri Wahyuni Mudrikah - Ebm B LindaDocument11 pages3 Jurnal Sri Wahyuni Mudrikah - Ebm B LindaAyoek Iku WahyuniNo ratings yet
- Sars-Cov-2 Infection During Pregnancy and Risk of Preeclampsia: A Systematic Review and Meta-AnalysisDocument25 pagesSars-Cov-2 Infection During Pregnancy and Risk of Preeclampsia: A Systematic Review and Meta-AnalysisErik SusantoNo ratings yet
- Hubungan Derajat Covid Saat HamilDocument7 pagesHubungan Derajat Covid Saat HamilRian AmertaNo ratings yet
- Maternal & Perinatal Outcome of Fever in Pregnancy in The Context of DengueDocument5 pagesMaternal & Perinatal Outcome of Fever in Pregnancy in The Context of DengueLola del carmen RojasNo ratings yet
- Maternal and Neonatal Outcomes of Pregnant Patients WithDocument8 pagesMaternal and Neonatal Outcomes of Pregnant Patients Withdini kusmaharaniNo ratings yet
- Articolo Pubmed Fattori Di RischioDocument17 pagesArticolo Pubmed Fattori Di RischioIltramonto Casa VacanzaNo ratings yet
- Maternal and Perinatal Outcomes of Pregnant WomenDocument11 pagesMaternal and Perinatal Outcomes of Pregnant Womenida husenNo ratings yet
- Section 44Document5 pagesSection 44Mark Christian GlindroNo ratings yet
- Gestational Diabetes Mellitus and COVID-19 (CRONOS)Document19 pagesGestational Diabetes Mellitus and COVID-19 (CRONOS)Diana MontoyaNo ratings yet
- Journal Pre-Proof: American Journal of Obstetrics & Gynecology MFMDocument28 pagesJournal Pre-Proof: American Journal of Obstetrics & Gynecology MFMLuciana PietroNo ratings yet
- Jurnal Sri Wahyuni Mudrikah - Ebm B LindaDocument11 pagesJurnal Sri Wahyuni Mudrikah - Ebm B LindaAyoek Iku WahyuniNo ratings yet
- DownloadDocument6 pagesDownloadKai GgNo ratings yet
- COVID-19 and Pregnancy: An Umbrella Review of Clinical Presentation, Vertical Transmission, and Maternal and Perinatal OutcomesDocument27 pagesCOVID-19 and Pregnancy: An Umbrella Review of Clinical Presentation, Vertical Transmission, and Maternal and Perinatal OutcomesFauzi AhmadNo ratings yet
- 10 1111@aogs 13867 PDFDocument19 pages10 1111@aogs 13867 PDFbrenda elielNo ratings yet
- COVID-19 and Pregnancy: A Review of Clinical Characteristics, Obstetric Outcomes and Vertical TransmissionDocument20 pagesCOVID-19 and Pregnancy: A Review of Clinical Characteristics, Obstetric Outcomes and Vertical TransmissionDra Sandra VèlezNo ratings yet
- COVID-19 Vaccination During Pregnancy: Coverage and Safety: ObstetricsDocument14 pagesCOVID-19 Vaccination During Pregnancy: Coverage and Safety: ObstetricsErik SusantoNo ratings yet
- Jurnal 1 CovidDocument5 pagesJurnal 1 CovidAyoek Iku WahyuniNo ratings yet
- Correlation Between Pregnancy Outcome and PlacentalDocument5 pagesCorrelation Between Pregnancy Outcome and PlacentalnskhldNo ratings yet
- Preeclampsia and COVID-19: Results From The INTERCOVID Prospective Longitudinal StudyDocument17 pagesPreeclampsia and COVID-19: Results From The INTERCOVID Prospective Longitudinal Studyulfa primadhaniNo ratings yet
- Pandemic and Impact of Covid/ Infectious DiseasesDocument5 pagesPandemic and Impact of Covid/ Infectious DiseasessamiaNo ratings yet
- Maternal and Perinatal Characteristics and Outcomes of Pregnancies Complicated With COVID-19 in KuwaitDocument22 pagesMaternal and Perinatal Characteristics and Outcomes of Pregnancies Complicated With COVID-19 in KuwaitSherlyNo ratings yet
- Covid-19 Vaccination in Pregnancy - The BMJDocument12 pagesCovid-19 Vaccination in Pregnancy - The BMJrichardonNo ratings yet
- JMRH - Volume 9 - Issue 4 - Pages 2883-2891Document9 pagesJMRH - Volume 9 - Issue 4 - Pages 2883-2891Chellyani Chantika DamayantiNo ratings yet
- Vaccines 08 00124 PDFDocument21 pagesVaccines 08 00124 PDFSaúl Alberto Kohan BocNo ratings yet
- Risk of Severe Maternal Morbidity Associated With Cesarean Delivery and The Role of Maternal Age: A Population-Based Propensity Score AnalysisDocument9 pagesRisk of Severe Maternal Morbidity Associated With Cesarean Delivery and The Role of Maternal Age: A Population-Based Propensity Score AnalysisJanainaNo ratings yet
- Journal Pre-Proof: American Journal of Obstetrics & Gynecology MFMDocument37 pagesJournal Pre-Proof: American Journal of Obstetrics & Gynecology MFMDinorah MarcelaNo ratings yet
- Lancet 170122 Effect of Maternal SarsCov2 Infection Timing On Birth OutcomesDocument10 pagesLancet 170122 Effect of Maternal SarsCov2 Infection Timing On Birth OutcomesqmfddnhdjmNo ratings yet
- 1 s2.0 S2468784722000587 MainDocument6 pages1 s2.0 S2468784722000587 Mainabatasa jahahoNo ratings yet
- Covid 19 Prematur Meta AnalisisDocument17 pagesCovid 19 Prematur Meta AnalisisRian AmertaNo ratings yet
- 3.english ISH MuliaDocument2 pages3.english ISH MuliaMulia AndaraNo ratings yet
- English ISH MuliaDocument2 pagesEnglish ISH MuliaMulia AndaraNo ratings yet
- Predictive Factors For Preeclampsia in Pregnant Women: A Unvariate and Multivariate Logistic Regression AnalysisDocument5 pagesPredictive Factors For Preeclampsia in Pregnant Women: A Unvariate and Multivariate Logistic Regression AnalysisTiti Afrida SariNo ratings yet
- Nihss PDFDocument11 pagesNihss PDFJidanNo ratings yet
- 1 s2.0 S204908012200471X MainDocument6 pages1 s2.0 S204908012200471X Mainafri pakalessyNo ratings yet
- R. Irvian1Document5 pagesR. Irvian1Ermawati RohanaNo ratings yet
- Maternal Periodontitis and Risk of Preterm Low Birth Weight Infants-Case Control Study Inindian PopulationDocument9 pagesMaternal Periodontitis and Risk of Preterm Low Birth Weight Infants-Case Control Study Inindian PopulationSmitha Kapani gowdaNo ratings yet
- 1 s2.0 S1028455919300178 Main PDFDocument5 pages1 s2.0 S1028455919300178 Main PDFRadinal PrayitnoNo ratings yet
- Pregnancy HypertensionDocument9 pagesPregnancy Hypertensionabi tehNo ratings yet
- Nidhi Thesis PresentationDocument25 pagesNidhi Thesis Presentationujjwal souravNo ratings yet
- Clinical Presentation and Outcomes of Pregnant Women With Coronavirus Disease 2019: A Systematic Review and Meta-AnalysisDocument13 pagesClinical Presentation and Outcomes of Pregnant Women With Coronavirus Disease 2019: A Systematic Review and Meta-AnalysisanggipuspaNo ratings yet
- Journal Reading Feto BORDocument27 pagesJournal Reading Feto BORbobbyrianto2210No ratings yet
- Jamapediatrics Dumitriu 2020 Oi 200070 1611604165.97231Document11 pagesJamapediatrics Dumitriu 2020 Oi 200070 1611604165.97231JeeNo ratings yet
- Outcome of Coronavirus Spectrum Infections (SARS, MERS, COVID-19) During Pregnancy: A Systematic Review and Meta-AnalysisDocument9 pagesOutcome of Coronavirus Spectrum Infections (SARS, MERS, COVID-19) During Pregnancy: A Systematic Review and Meta-AnalysisyukihannaNo ratings yet
- Journal Pre-Proof: American Journal of Obstetrics and GynecologyDocument43 pagesJournal Pre-Proof: American Journal of Obstetrics and GynecologySyabrina DindaNo ratings yet
- 1 PBDocument6 pages1 PBArjuna MedagamaNo ratings yet
- Early Predictors For Hypertensive Disorders of Pregnancy in Developing CountriesDocument12 pagesEarly Predictors For Hypertensive Disorders of Pregnancy in Developing CountriesBayna Lestari LubisNo ratings yet
- Asociacion Funcion Renal Materna y Resultados Embarazo DM 1 y 2.seah.2020Document8 pagesAsociacion Funcion Renal Materna y Resultados Embarazo DM 1 y 2.seah.2020Andrés Gaviria CNo ratings yet
- Low Birth Weight As Risk Factor of Pneumonia Child in Primary Health Care of SurabayaDocument3 pagesLow Birth Weight As Risk Factor of Pneumonia Child in Primary Health Care of SurabayaAyu Eka SetiawatiNo ratings yet
- Pengetahuan Dan Praktik Bidan Tentang Standar Pelayanan Kehamilan Di Era Pandemi Covid-19Document6 pagesPengetahuan Dan Praktik Bidan Tentang Standar Pelayanan Kehamilan Di Era Pandemi Covid-19Meysifa NNo ratings yet
- Reappraisal of Guidelines For Management of Neonates With Suspected Early-Onset SepsisDocument5 pagesReappraisal of Guidelines For Management of Neonates With Suspected Early-Onset SepsisMarco Antonio Mendoza OjedaNo ratings yet
- Incidence and Risk Factors of Pre-Eclampsia in The Paropakar Maternity and Women's Hospital, Nepal: A Retrospective StudyDocument8 pagesIncidence and Risk Factors of Pre-Eclampsia in The Paropakar Maternity and Women's Hospital, Nepal: A Retrospective StudyJod BellNo ratings yet
- Sonnykalangi,+13 +ok+ (13) +sudarman+68-80Document21 pagesSonnykalangi,+13 +ok+ (13) +sudarman+68-80Nandini Permata SariNo ratings yet
- Zika Virus Infection and Pregnancy: Guidelines in FocusDocument8 pagesZika Virus Infection and Pregnancy: Guidelines in FocusMarlon SoselisaNo ratings yet
- Ijogr 3 (4) 407-409Document3 pagesIjogr 3 (4) 407-409Yuni Astuti DjoyomiharjoNo ratings yet
- Coronavirus in Pregnancy and Delivery Rapid ReviewDocument16 pagesCoronavirus in Pregnancy and Delivery Rapid Reviewluisemisasc1990No ratings yet
- Perinatal Outcomes in Acute Respiratory Viral Infection in Pregnant WomenDocument3 pagesPerinatal Outcomes in Acute Respiratory Viral Infection in Pregnant WomenCentral Asian StudiesNo ratings yet
- Placental Sars Cov 2 in A Pregnant Woman With Mild Covid 19 DiseaseDocument7 pagesPlacental Sars Cov 2 in A Pregnant Woman With Mild Covid 19 Diseaseumbu anandaNo ratings yet
- Bakker 2012Document10 pagesBakker 2012ieoNo ratings yet
- Routine Screening For SARS CoV-2 in EnglishDocument13 pagesRoutine Screening For SARS CoV-2 in EnglishAffah MustafaNo ratings yet
- Living on the Frontline of COVID-19 in MCO And CMCOFrom EverandLiving on the Frontline of COVID-19 in MCO And CMCONo ratings yet
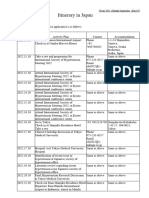
- ItineraryDocument1 pageItineraryMulia AndaraNo ratings yet
- English ISH MuliaDocument2 pagesEnglish ISH MuliaMulia AndaraNo ratings yet
- KarakteristikDocument3 pagesKarakteristikMulia AndaraNo ratings yet
- Manajemen Jalan Nafas Pada Pasien Dengan Tumor Mandibula: Laporan KasusDocument27 pagesManajemen Jalan Nafas Pada Pasien Dengan Tumor Mandibula: Laporan KasusMulia AndaraNo ratings yet
- 3.english ISH MuliaDocument2 pages3.english ISH MuliaMulia AndaraNo ratings yet
- JurnalDocument2 pagesJurnalMulia AndaraNo ratings yet
- Health Education LM Week 1 and 2Document8 pagesHealth Education LM Week 1 and 2Joice LenteriaNo ratings yet
- Patient Centerd CareDocument42 pagesPatient Centerd Care21910589No ratings yet
- Fundamentals of Nursing Letter AnswersDocument1 pageFundamentals of Nursing Letter AnswersEpaphras Joel MilitarNo ratings yet
- PLPF PDFDocument88 pagesPLPF PDFmaxNo ratings yet
- IPSGDocument16 pagesIPSGNyimas Milka Ayu NabilaNo ratings yet
- Global Health Benefits: Policy Holder: Policy #: Effective Date: Insured: Member #Document1 pageGlobal Health Benefits: Policy Holder: Policy #: Effective Date: Insured: Member #youtube clapzzyNo ratings yet
- Nursing ResumeDocument3 pagesNursing Resumeapi-313972870No ratings yet
- NCM 102Document8 pagesNCM 102lemuel_que100% (2)
- Paper PresentationDocument5 pagesPaper PresentationSamjaisheel SamsonNo ratings yet
- Evidence Based Medicine: What It Is and What It Isn'tDocument3 pagesEvidence Based Medicine: What It Is and What It Isn'tCristian EstradaNo ratings yet
- Midterms NCM 104 Rle CHNDocument7 pagesMidterms NCM 104 Rle CHNVince SicangcoNo ratings yet
- Higher Education of RizalDocument3 pagesHigher Education of RizaltrinabagueNo ratings yet
- Case History Final PDFDocument16 pagesCase History Final PDFRameshNo ratings yet
- Report of Medicare Multispeciality Hospital and Trauma CentreDocument5 pagesReport of Medicare Multispeciality Hospital and Trauma CentremuskanNo ratings yet
- Cardiology BrochureDocument2 pagesCardiology Brochureong251183No ratings yet
- Biopharmaceutics IntroductionDocument46 pagesBiopharmaceutics IntroductionMinal NadeemNo ratings yet
- JMIR Med Edu - Response To Letter To Editor - USMLE Step 1 Pass Fail ChangeDocument3 pagesJMIR Med Edu - Response To Letter To Editor - USMLE Step 1 Pass Fail ChangeAhmad OzairNo ratings yet
- Nosocomial Infection?Document4 pagesNosocomial Infection?Sara ANo ratings yet
- Oet Writing FormatDocument6 pagesOet Writing FormatRosselini EspinedaNo ratings yet
- Vero DoxDocument61 pagesVero DoxMWANGINo ratings yet
- My Fitness Journal - BarbaDocument18 pagesMy Fitness Journal - BarbaCj AranteNo ratings yet
- Peter Dickinson: Return To The CaseDocument5 pagesPeter Dickinson: Return To The Casebella swanNo ratings yet
- Grade 10 Health 1ST QuarterDocument32 pagesGrade 10 Health 1ST QuarterKristela Mae ColomaNo ratings yet
- Tooth Implant Supported Prosthesis: A Literature ReviewDocument8 pagesTooth Implant Supported Prosthesis: A Literature ReviewTung Thanh NguyenNo ratings yet
- APA - DSM5 - WHODAS 2 Proxy Administered PDFDocument6 pagesAPA - DSM5 - WHODAS 2 Proxy Administered PDFrazvNo ratings yet
- Health Assure Insurance POLICYDocument2 pagesHealth Assure Insurance POLICYRISHAB CHETRINo ratings yet
- Improving Patient Safety in Hospitals-A Resource List ForDocument25 pagesImproving Patient Safety in Hospitals-A Resource List FormurvinandNo ratings yet
- Enteric BacteriaDocument16 pagesEnteric BacteriaBernie QuepNo ratings yet
- Anatomi Berorientasi Klinis: A. Sentot Suropati. Dr. SPPD, FinasimDocument47 pagesAnatomi Berorientasi Klinis: A. Sentot Suropati. Dr. SPPD, FinasimYudhistira NugrahaNo ratings yet
- Straight WireDocument1 pageStraight Wiresvetaine.ltNo ratings yet