You might also like
- Guyton and Hall Textbook of Medical PhysiologyDocument13 pagesGuyton and Hall Textbook of Medical PhysiologyRobert StevenNo ratings yet
- Valvular Heart DiseaseDocument27 pagesValvular Heart DiseaseOwen J. WieseNo ratings yet
- Cardiac AsthmaDocument12 pagesCardiac AsthmaNeupane KsabNo ratings yet
- The Spectrum of TBDocument174 pagesThe Spectrum of TBcmolina84No ratings yet
- InflammationDocument59 pagesInflammationKarthik KumarNo ratings yet
- Vascular Complication of Injectable FillerDocument17 pagesVascular Complication of Injectable Fillerahmed100% (1)
- Valvular Heart DiseaseDocument2 pagesValvular Heart DiseaseAnonymous TVk12eX4No ratings yet
- Fontan Operation: DR Hussain BuxDocument62 pagesFontan Operation: DR Hussain BuxMujeeb Ur RehmanNo ratings yet
- Cardiogenic Pulmonary EdemaDocument1 pageCardiogenic Pulmonary EdemaAirish LimNo ratings yet
- Sepsis: PathophysiologyDocument8 pagesSepsis: PathophysiologyDonald NashNo ratings yet
- Asthma and Rhinitis During PregnancyDocument175 pagesAsthma and Rhinitis During PregnancyAndika Wima PratamaNo ratings yet
- Cardiac AssessmentDocument48 pagesCardiac AssessmentRatheesh NathNo ratings yet
- Anat FisioDocument653 pagesAnat Fisiodenydeniche388No ratings yet
- Sepsis WhoDocument36 pagesSepsis WholcycrlnNo ratings yet
- Diagnostic Thoracoscopy (VATS) in Lung CancerDocument18 pagesDiagnostic Thoracoscopy (VATS) in Lung CancerlmdarlongNo ratings yet
- Idiopathic Pulmonary Fibrosis: Optimizing The Diagnosis and Multi-Disciplinary Decision MakingDocument4 pagesIdiopathic Pulmonary Fibrosis: Optimizing The Diagnosis and Multi-Disciplinary Decision MakingAnna LiachenkoNo ratings yet
- Drenaj LimfaticDocument71 pagesDrenaj LimfaticGugiu Bogdan Ștefan90% (20)
- BronchoPulmonary Hygiene TechniquesDocument88 pagesBronchoPulmonary Hygiene Techniques私 シャーロットNo ratings yet
- Interstitial Lung DiseaseDocument26 pagesInterstitial Lung DiseaseEnimia ShyNo ratings yet
- Lung Mechanics and Ventilation-Lecture NotesDocument16 pagesLung Mechanics and Ventilation-Lecture NotesCarlos Eduardo LinaresNo ratings yet
- Cardiac Risk AssessmentDocument4 pagesCardiac Risk Assessmentmonir61No ratings yet
- Restrictive Lung DiseaseDocument32 pagesRestrictive Lung DiseaseSalman Khan100% (1)
- The PERT Concept Q1 A Step-By-Step Approach To Managing Pulmonary EmbolismDocument9 pagesThe PERT Concept Q1 A Step-By-Step Approach To Managing Pulmonary EmbolismntnquynhproNo ratings yet
- Textbook of Surgery For Dental Students-smile4DrDocument400 pagesTextbook of Surgery For Dental Students-smile4DrRotariu Ana Maria100% (8)
- Arterial Line Arterial LineDocument13 pagesArterial Line Arterial LineLinamaria Lozano100% (1)
- Sepsis and Septic ShockDocument70 pagesSepsis and Septic ShockLily SolNo ratings yet
- Chronic Obstructive Pulmonary DiseaseFrom EverandChronic Obstructive Pulmonary DiseaseRobert A. StockleyNo ratings yet
- Ultrasonography of the Lung: Understanding the BLUE, FALLS and SESAME ProtocolsDocument12 pagesUltrasonography of the Lung: Understanding the BLUE, FALLS and SESAME ProtocolsMauricio Tapia100% (1)
- Unstable Angina, STEMI, NSTEMI Diagnosis and ManagementDocument21 pagesUnstable Angina, STEMI, NSTEMI Diagnosis and ManagementNabil Mosharraf Hossain100% (2)
- Recent TB Treatment GuidelinesDocument28 pagesRecent TB Treatment GuidelinesDr venkatesh jalluNo ratings yet
- 9D NLBA Illustrated Glossary 2015Document141 pages9D NLBA Illustrated Glossary 2015galante81No ratings yet
- Refractory Septic ShockDocument5 pagesRefractory Septic ShockBrian Antonio Veramatos LopezNo ratings yet
- BLUE-Protocol and FALLS-Protocol: Two Applications of Lung Ultrasound in The Critically IllDocument12 pagesBLUE-Protocol and FALLS-Protocol: Two Applications of Lung Ultrasound in The Critically IllChristiaan CordovaNo ratings yet
- An Assignment ON: Bronchial HygieneDocument12 pagesAn Assignment ON: Bronchial Hygienesoniya joseph100% (1)
- Pulmonary SequestrationDocument15 pagesPulmonary SequestrationEmily EresumaNo ratings yet
- IntroductionDocument13 pagesIntroductionSiyara AntonyNo ratings yet
- DO /VO Relationships: J. L. VincentDocument8 pagesDO /VO Relationships: J. L. VincentLucas Cárcamo SaavedraNo ratings yet
- Clinical Case Study Guide - Cardiopulmonary Physical Therapy 3ed PDFDocument245 pagesClinical Case Study Guide - Cardiopulmonary Physical Therapy 3ed PDFraquelbibi0% (1)
- Pneumonia Management ProtocolDocument2 pagesPneumonia Management Protocolsky nuts100% (1)
- Suctioning Artificial Airways - AdultsDocument27 pagesSuctioning Artificial Airways - AdultssdaNo ratings yet
- CABG Case Study ReportDocument83 pagesCABG Case Study ReportSherena NicolasNo ratings yet
- Heart FailureDocument6 pagesHeart FailureNatasha MarksNo ratings yet
- Atrial Fibrillation: Discussed by - DR Kunwar Sidharth SaurabhDocument45 pagesAtrial Fibrillation: Discussed by - DR Kunwar Sidharth SaurabhKunwar Sidharth SaurabhNo ratings yet
- Epid COPDDocument9 pagesEpid COPDAgung WistaraNo ratings yet
- Anesthesia for Congenital Heart DiseaseFrom EverandAnesthesia for Congenital Heart DiseaseStephen A. StayerNo ratings yet
- Abdominal TuberculosisDocument28 pagesAbdominal TuberculosisNajezita Sachenka CH CNo ratings yet
- A Prospective Study of Prescribing Pattern in The Management of Stroke at A Tertiary Care HospitalDocument6 pagesA Prospective Study of Prescribing Pattern in The Management of Stroke at A Tertiary Care HospitalInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Clinical ECG RoundsDocument2 pagesClinical ECG RoundsKai Siang ChanNo ratings yet
- Abdominal TuberculosisDocument35 pagesAbdominal TuberculosisAWw LieyaNo ratings yet
- CNS Tuberculosis Pathogenesis, Diagnosis and TreatmentDocument19 pagesCNS Tuberculosis Pathogenesis, Diagnosis and TreatmentFabricio NuñezNo ratings yet
- Ventricular Septal DefectsDocument7 pagesVentricular Septal DefectsMuhammadAldoGiansyahNo ratings yet
- End-Stage Heart Disease Management and Palliative Care GuidelinesDocument44 pagesEnd-Stage Heart Disease Management and Palliative Care GuidelinesCyrille AgnesNo ratings yet
- Left-Sided Congestive Heart Failure Case PresentationDocument64 pagesLeft-Sided Congestive Heart Failure Case PresentationNicole Villanueva, BSN - Level 3ANo ratings yet
- Pulmonary HypertensionDocument9 pagesPulmonary HypertensionDesriani Anisa YakubNo ratings yet
- Lung Protective Mechanical Ventilation StrategiesDocument4 pagesLung Protective Mechanical Ventilation StrategiesAnne Julia AgustinNo ratings yet
- Ventilator-Associated Pneumonia Prevention: We Still Have A Long Way To Go!Document2 pagesVentilator-Associated Pneumonia Prevention: We Still Have A Long Way To Go!AzmachamberAzmacareNo ratings yet
- DR Sandeep - EISENMENGER SYNDROMEDocument81 pagesDR Sandeep - EISENMENGER SYNDROMEAlexandrescuNo ratings yet
- Drug Compliance Among Hypertensive PatientsDocument5 pagesDrug Compliance Among Hypertensive PatientsSyifa MunawarahNo ratings yet
- Anti T.B DrugsDocument120 pagesAnti T.B DrugsromalaramNo ratings yet
- Disorders of AortaDocument25 pagesDisorders of Aortavani reddyNo ratings yet
- Scape Vs FospeDocument5 pagesScape Vs FospeDr. FarhanNo ratings yet
- Cardiogenic ShockDocument6 pagesCardiogenic ShockhamadaelgenNo ratings yet
- Causes, Symptoms and Nursing Care of AtherosclerosisDocument16 pagesCauses, Symptoms and Nursing Care of AtherosclerosisSAZZY ASHLEY GADDANGNo ratings yet
- Primer On Clinical Acid-Base Problem Solving - DisAMon 2004Document41 pagesPrimer On Clinical Acid-Base Problem Solving - DisAMon 2004Ashley100% (1)
- Primary and Secondary CV Prevention - Iman EvanDocument104 pagesPrimary and Secondary CV Prevention - Iman EvanFikriYTNo ratings yet
- Acute Respiratory Distress SyndromeDocument30 pagesAcute Respiratory Distress SyndromeNikhil GhubadeNo ratings yet
- Tetralogy of FallotDocument24 pagesTetralogy of FallotjustinahorroNo ratings yet
- 2015 Chest - Blue & Falls ProtocolsDocument12 pages2015 Chest - Blue & Falls ProtocolsWilmer Yanquen VillarrealNo ratings yet
- Definition, Classification, Etiology, and Pathophysiology of Shock in Adults - UpToDateDocument16 pagesDefinition, Classification, Etiology, and Pathophysiology of Shock in Adults - UpToDatevara prasadNo ratings yet
- Pathophysiology of Cardiogenic Pulmonary EdemaDocument13 pagesPathophysiology of Cardiogenic Pulmonary EdemaIrina DuceacNo ratings yet
- Initial Assessment and Management of Acute StrokeDocument49 pagesInitial Assessment and Management of Acute StrokeIrina DuceacNo ratings yet
- Clostridioides Difficile Infection in AdultsDocument28 pagesClostridioides Difficile Infection in AdultsIrina DuceacNo ratings yet
- AdrenalineDocument6 pagesAdrenalineIrina DuceacNo ratings yet
- Acute Pulmonary OdemaDocument9 pagesAcute Pulmonary OdemaAnonymous ysrxggk21cNo ratings yet
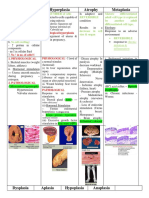
- Hypertrophy Hyperplasia Atrophy MetaplasiaDocument20 pagesHypertrophy Hyperplasia Atrophy MetaplasiaYunQingTanNo ratings yet
- Arterial HyperemyDocument10 pagesArterial HyperemyRohit NaiduNo ratings yet
- Int Endodontic J - 2020 - Zhan - Dental Nerves A Neglected Mediator of PulpitisDocument15 pagesInt Endodontic J - 2020 - Zhan - Dental Nerves A Neglected Mediator of PulpitisDevin KwanNo ratings yet
- Cerebral Perfusion Simulation Using Realistically Generated Synthetic TreesDocument9 pagesCerebral Perfusion Simulation Using Realistically Generated Synthetic Treessunhao13287710014No ratings yet
- Circulatory System REVIEWERDocument6 pagesCirculatory System REVIEWERClyde BaltazarNo ratings yet
- Sindrom Multiple Disfungsi OrganDocument8 pagesSindrom Multiple Disfungsi OrganAdi Nugroho MelyanaNo ratings yet
- Lecture 6 Cardiovascular: Vascular System - The HemodynamicsDocument61 pagesLecture 6 Cardiovascular: Vascular System - The HemodynamicsAndreea ŞtefănescuNo ratings yet
- PubMed Links 20171119Document2 pagesPubMed Links 20171119Scott BermanNo ratings yet
- Cvs BdsDocument142 pagesCvs BdsDr Dhiren Kumar PandaNo ratings yet
- Relationship Between Endogenous Hydrogen Sulfide and Blood Stasis Syndrome Based On The Qi-Blood Theory of Chinese MedicineDocument6 pagesRelationship Between Endogenous Hydrogen Sulfide and Blood Stasis Syndrome Based On The Qi-Blood Theory of Chinese MedicineleonieNo ratings yet
- Human Anat 2 Year Volume 4Document122 pagesHuman Anat 2 Year Volume 4HARSHINI PANDIANNo ratings yet
- Gelofusine®: Stop Infusion andDocument2 pagesGelofusine®: Stop Infusion andRudy Arindra WijayaNo ratings yet
- Dry Cupping Therapy Reduces Cellulite in WomenDocument7 pagesDry Cupping Therapy Reduces Cellulite in WomenDorothee RosarioNo ratings yet
- Charny - Mathematical Models of Bioheat TransferDocument137 pagesCharny - Mathematical Models of Bioheat TransferMadalena PanNo ratings yet
- 2019 Raynaud's PhenomenonDocument21 pages2019 Raynaud's PhenomenonGerman Gustavo Salgado TapiaNo ratings yet
- 1b-Physio-1m-Cvs 4Document12 pages1b-Physio-1m-Cvs 4urvashi rao rajputNo ratings yet
- Acute Inflammation (Vascular Changes) - 1Document33 pagesAcute Inflammation (Vascular Changes) - 1Ramesh KumarNo ratings yet
- High performance BodyWave tanning and beauty machineDocument11 pagesHigh performance BodyWave tanning and beauty machinetranspotNo ratings yet
- Dermatitits StasisDocument11 pagesDermatitits StasisRiyan TjahyaNo ratings yet