You might also like
- (UPCAT) Result 2006 Fiona DLRDocument4 pages(UPCAT) Result 2006 Fiona DLRapi-37595710% (2)
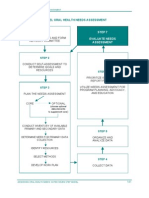
- Step 7Document9 pagesStep 7Abu Yussif AlaboodiNo ratings yet
- 8 Critical Change Management Models To Evolve and Survive - Process StreetDocument52 pages8 Critical Change Management Models To Evolve and Survive - Process StreetUJJWALNo ratings yet
- 039 Governance Assessment ToolDocument3 pages039 Governance Assessment ToolPedro GouveiaNo ratings yet
- SOBER Study Overview 2023-06-01Document13 pagesSOBER Study Overview 2023-06-01Joe WinstonNo ratings yet
- Equity and Monitoring Progress of The NSHDP in Nigeria - The PHC Reviews by DR Eboreime EjemaiDocument34 pagesEquity and Monitoring Progress of The NSHDP in Nigeria - The PHC Reviews by DR Eboreime EjemaiEjemai EboreimeNo ratings yet
- KAP Survey PDFDocument22 pagesKAP Survey PDFEssam MunirNo ratings yet
- Health Information System Literature ReviewDocument5 pagesHealth Information System Literature Reviewlsfxofrif100% (1)
- Safe Surgery 3Document12 pagesSafe Surgery 3Masrun FatanahNo ratings yet
- Optional TOR FileDocument24 pagesOptional TOR FileBabaiNo ratings yet
- Cur 528 Week 4 Signature Assignment Planning A Needs AssessmentDocument8 pagesCur 528 Week 4 Signature Assignment Planning A Needs Assessmentapi-528349363No ratings yet
- Every Newborn ToolsDocument6 pagesEvery Newborn ToolsArti NegiNo ratings yet
- Six strategic steps for conducting a situational assessmentDocument8 pagesSix strategic steps for conducting a situational assessmentLaimonas BartkusNo ratings yet
- Tugas Sistem Informasi KesehatanDocument37 pagesTugas Sistem Informasi Kesehatandewi shintaNo ratings yet
- Monitoring and Evaluation ToolsDocument53 pagesMonitoring and Evaluation ToolsJunu Hada100% (1)
- Art 3A10.1186 2Fs12912 015 0097 3Document13 pagesArt 3A10.1186 2Fs12912 015 0097 3S LaimeheriwaNo ratings yet
- A Proposal of A Mobile Health Data Collection and Reporting System For The Developing World - by Deo ShaoDocument2 pagesA Proposal of A Mobile Health Data Collection and Reporting System For The Developing World - by Deo ShaoDeo ShayoNo ratings yet
- The WHO Performance Assessment Tool For Quality Im PDFDocument7 pagesThe WHO Performance Assessment Tool For Quality Im PDFNii NgsNo ratings yet
- Evaluation of The Impact of The National Resource For Infection ControlDocument22 pagesEvaluation of The Impact of The National Resource For Infection ControlAkankshya GorkhaliNo ratings yet
- Logic Models For Planning EvaluationDocument21 pagesLogic Models For Planning EvaluationAji HandokoNo ratings yet
- Description: Tags: Section-IvDocument51 pagesDescription: Tags: Section-Ivanon-889981No ratings yet
- Poster iHEADocument1 pagePoster iHEANoel BañezNo ratings yet
- Health Management ProjectDocument56 pagesHealth Management ProjectAbhishek Kumar RamadhinNo ratings yet
- TanzaniaDocument10 pagesTanzaniahst939No ratings yet
- Seminar MiesDocument16 pagesSeminar Mieshannahashok0% (1)
- Matic Pablo Pantig Patungan Peralta Nursing Informatics Final Requirement Conduct of Research Writing Thru Scoping ReviewDocument11 pagesMatic Pablo Pantig Patungan Peralta Nursing Informatics Final Requirement Conduct of Research Writing Thru Scoping ReviewYuuki Chitose (tai-kun)No ratings yet
- Effects of Performance Improvement Programs On Preparedness CapacitiesDocument9 pagesEffects of Performance Improvement Programs On Preparedness CapacitiesMathilda UllyNo ratings yet
- APHSA Roadmap To Capacity Building in Analytics White PaperDocument26 pagesAPHSA Roadmap To Capacity Building in Analytics White PaperShritam ShibashisNo ratings yet
- Community Health AssesmentDocument15 pagesCommunity Health AssesmentGudegna GemechuNo ratings yet
- Role of Health Surveys in National Health Information Systems: Best-Use ScenariosDocument28 pagesRole of Health Surveys in National Health Information Systems: Best-Use ScenariosazfarNo ratings yet
- Recommended Quality Control Standards: Washington State Research-Based Juvenile Offender ProgramsDocument6 pagesRecommended Quality Control Standards: Washington State Research-Based Juvenile Offender ProgramsWashington State Institute for Public PolicyNo ratings yet
- The Importance of Data Quality Assurance in Improving Grant Implementation - An Example From NigeriaDocument7 pagesThe Importance of Data Quality Assurance in Improving Grant Implementation - An Example From NigeriaAlexander DeckerNo ratings yet
- Standards For Maternal and Neonatal Care - WHODocument72 pagesStandards For Maternal and Neonatal Care - WHODharmendra PanwarNo ratings yet
- Community Health Center IT Assessment Final ReportDocument178 pagesCommunity Health Center IT Assessment Final ReportObby Syah YugamieNo ratings yet
- Ajol-File-Journals 56 Articles 251158 64b650fe991eeDocument12 pagesAjol-File-Journals 56 Articles 251158 64b650fe991eebezuayehu adaneNo ratings yet
- Basic & Clinical Biostatistics, 4th EditionDocument6 pagesBasic & Clinical Biostatistics, 4th EditionbencleeseNo ratings yet
- EDBADocument11 pagesEDBABilal SalamehNo ratings yet
- 01 Bio Med WastDocument33 pages01 Bio Med WastSp PpvNo ratings yet
- Demographic Surveillance: Call For Full ProposalsDocument11 pagesDemographic Surveillance: Call For Full ProposalsAmir MirNo ratings yet
- Clinical ResearchDocument2 pagesClinical ResearchEP YaredNo ratings yet
- Handout 10 1.2Document3 pagesHandout 10 1.2Miftah TemamNo ratings yet
- King County School-Based SBIRT Program Evaluation PlanDocument8 pagesKing County School-Based SBIRT Program Evaluation PlanMedium Team100% (1)
- Baseline Assessment of Primary Healthcare Delivery Through Subcenters of Northern IndiaDocument12 pagesBaseline Assessment of Primary Healthcare Delivery Through Subcenters of Northern IndiaAr. Libin K BabyNo ratings yet
- Health RecordsDocument36 pagesHealth RecordsMatthew NdetoNo ratings yet
- Patient CenteredDocument12 pagesPatient CenteredNina NaguyevskayaNo ratings yet
- IDSPDocument56 pagesIDSPitsdheeraj2002No ratings yet
- Evaluation of A National Telemedicine Initiative in The Veterans Health Administration: Factors Associated With Successful ImplementationDocument11 pagesEvaluation of A National Telemedicine Initiative in The Veterans Health Administration: Factors Associated With Successful ImplementationKarl Benedict OngNo ratings yet
- NSP Curriculum Outline v0Document12 pagesNSP Curriculum Outline v0ashakow8849No ratings yet
- 1 PBDocument7 pages1 PBqwerty masterNo ratings yet
- Critical Analysis of a Community Nursing Information SystemDocument5 pagesCritical Analysis of a Community Nursing Information SystemAgboola Ayobami AbiolaNo ratings yet
- Health-Care Waste Management - Rapid Assessment Tool: For Country Level ContentDocument33 pagesHealth-Care Waste Management - Rapid Assessment Tool: For Country Level ContentArpo MukherjeeNo ratings yet
- The Audit Process and How To Ensure A Successful AuditDocument19 pagesThe Audit Process and How To Ensure A Successful AuditRudy surya 08No ratings yet
- Community Need AssessmentDocument6 pagesCommunity Need AssessmentCynthia WilsonNo ratings yet
- HIS Strategic Plan 2009-2014, 05.08Document58 pagesHIS Strategic Plan 2009-2014, 05.08Majiva100% (3)
- Strengthening MCH His PicDocument21 pagesStrengthening MCH His PicGuntiar RachmadDiansyahNo ratings yet
- Published Researches in The Year 2010Document16 pagesPublished Researches in The Year 2010hsrimediaNo ratings yet
- UNICEF SanitationMonitoring Toolkit 2Document90 pagesUNICEF SanitationMonitoring Toolkit 2Ulil RukmanaNo ratings yet
- WHO MBHSS 2010 Section3 WebDocument16 pagesWHO MBHSS 2010 Section3 WebAn Nisa Akhlaqul KarimahNo ratings yet
- Philippines Influencing PolicyDocument32 pagesPhilippines Influencing PolicyjericsmomNo ratings yet
- Mobile Based Community Monitoring SystemDocument22 pagesMobile Based Community Monitoring SystemOneEyedCanineNo ratings yet
- Developing a common framework for international mental healthcare quality indicatorsDocument6 pagesDeveloping a common framework for international mental healthcare quality indicatorsCarl FisherNo ratings yet
- Healthy Babies Are Worth The Wait: A Partnership to Reduce Preterm Births in Kentucky through Community-based Interventions 2007 - 2009From EverandHealthy Babies Are Worth The Wait: A Partnership to Reduce Preterm Births in Kentucky through Community-based Interventions 2007 - 2009No ratings yet
- HLA ALLELES AND RHEUMATOID ARTHRITISDocument4 pagesHLA ALLELES AND RHEUMATOID ARTHRITISsunilpkumar18No ratings yet
- 01-Bionature 2004Document6 pages01-Bionature 2004sunilpkumar18No ratings yet
- 02 - Hav 2006Document6 pages02 - Hav 2006sunilpkumar18No ratings yet
- 08 - IjmrDocument5 pages08 - Ijmrsunilpkumar18No ratings yet
- 05 - CL Bioch 2008Document7 pages05 - CL Bioch 2008sunilpkumar18No ratings yet
- Does Mutation of Hepatitis A Virus Exist in North IndiaDocument5 pagesDoes Mutation of Hepatitis A Virus Exist in North Indiasunilpkumar18No ratings yet
- PCR Tiling of Sars Cov 2 Virus With Rapid Barcoding SQK rbk110 PCTR - 9125 - v110 - Revh - 24mar2021 MinionDocument40 pagesPCR Tiling of Sars Cov 2 Virus With Rapid Barcoding SQK rbk110 PCTR - 9125 - v110 - Revh - 24mar2021 Minionsunilpkumar18No ratings yet
- HBV Mutations and Genotypes Linked to Hepatocellular Carcinoma Risk in IndiaDocument11 pagesHBV Mutations and Genotypes Linked to Hepatocellular Carcinoma Risk in Indiasunilpkumar18No ratings yet
- A Pilot Study of Expanded Newborn Screening For 573 Genes Related To Severe Inherited Disorders in China: Results From 1,127 NewbornsDocument10 pagesA Pilot Study of Expanded Newborn Screening For 573 Genes Related To Severe Inherited Disorders in China: Results From 1,127 Newbornssunilpkumar18No ratings yet
- Ijns 07 00074Document13 pagesIjns 07 00074sunilpkumar18No ratings yet
- 5081 PDFDocument159 pages5081 PDFTemp PersonNo ratings yet
- Week 5 Edtpa Class LessonsDocument18 pagesWeek 5 Edtpa Class Lessonsapi-510714748No ratings yet
- USAID Conference - Beyond The Usual Suspects-EdDocument4 pagesUSAID Conference - Beyond The Usual Suspects-EdInterActionNo ratings yet
- Soal PTS Kelas 6 B. INGGRIS 2022Document3 pagesSoal PTS Kelas 6 B. INGGRIS 2022SITI NUR'ARIYANINo ratings yet
- SAP Certified FICO Consultant ResumeDocument12 pagesSAP Certified FICO Consultant Resumeஆக்ஞா கிருஷ்ணா ஷர்மாNo ratings yet
- Spatial Trauma/Desire: A Postmodern Sociocultural PhenomenonDocument0 pagesSpatial Trauma/Desire: A Postmodern Sociocultural PhenomenonLesleigh Ochavillo ManginsayNo ratings yet
- Resume - Telecom Trainer, 3g Live Jobs, Tunis, Tunisia, AfricaDocument2 pagesResume - Telecom Trainer, 3g Live Jobs, Tunis, Tunisia, AfricaDiwakar MishraNo ratings yet
- Data Encryption: Encryption Technologies For Data Protection On The Now Platform®Document21 pagesData Encryption: Encryption Technologies For Data Protection On The Now Platform®Rocco BurocoNo ratings yet
- IMICS Graduate Handbook 2014Document31 pagesIMICS Graduate Handbook 2014greenglassNo ratings yet
- Undertaking Form For Shifters and TransfereesDocument1 pageUndertaking Form For Shifters and TransfereesAngela JingcoNo ratings yet
- Punjab National Bank Punjab National Bank Punjab National BankDocument1 pagePunjab National Bank Punjab National Bank Punjab National BankHarsh ChaudharyNo ratings yet
- Communion With The Goddess Priestesses PDFDocument30 pagesCommunion With The Goddess Priestesses PDFAtmageet KaurNo ratings yet
- Identification Parade AssignmentDocument10 pagesIdentification Parade AssignmentAbdul Rehman100% (1)
- Mythology and FolkloreDocument6 pagesMythology and FolkloreSampaga, Lovely Grace FerraroNo ratings yet
- Aeronautical Office Media KitDocument18 pagesAeronautical Office Media Kitapi-655212626No ratings yet
- All 18 QSS in One-1 PDFDocument314 pagesAll 18 QSS in One-1 PDFkishan23100% (1)
- ESwitching PTAct 6 5 1Document4 pagesESwitching PTAct 6 5 1Wayne E. BollmanNo ratings yet
- Multi Q!Document112 pagesMulti Q!collinmandersonNo ratings yet
- Electrical Engineering Portal - Com Substation Fire ProtectionDocument4 pagesElectrical Engineering Portal - Com Substation Fire ProtectionJaeman ParkNo ratings yet
- Security Valuations - Stocks EZDocument9 pagesSecurity Valuations - Stocks EZAakash RegmiNo ratings yet
- Module 6 - Fabm2-MergedDocument37 pagesModule 6 - Fabm2-MergedJaazaniah S. PavilionNo ratings yet
- Nobody Does It Better and Indian Hospitality Will Leave You Feeling Better Too.Document2 pagesNobody Does It Better and Indian Hospitality Will Leave You Feeling Better Too.Abhijeet UmatheNo ratings yet
- Manchester Devt. Corp. vs. CA, GR No. 75919Document3 pagesManchester Devt. Corp. vs. CA, GR No. 75919Rodel Cadorniga Jr.No ratings yet
- Shakespearean LanguageDocument52 pagesShakespearean LanguageBailey HarrisonNo ratings yet
- All Hands Naval Bulletin - Nov 1942Document56 pagesAll Hands Naval Bulletin - Nov 1942CAP History Library0% (1)
- Notification No.54/2021 - Customs (N.T.) : Schedule-IDocument3 pagesNotification No.54/2021 - Customs (N.T.) : Schedule-Ianil nayakanahattiNo ratings yet
- INDIAN WAR OF INDEPENDENCE 1857 - ORIGINAL PUBLISHERs NoteDocument19 pagesINDIAN WAR OF INDEPENDENCE 1857 - ORIGINAL PUBLISHERs NoteBISWAJIT MOHANTYNo ratings yet
- Relationship Between Cigarette Smoking and Novel Risk Factors For Cardiovascular DiseaseDocument4 pagesRelationship Between Cigarette Smoking and Novel Risk Factors For Cardiovascular DiseaseInternational Medical PublisherNo ratings yet