You might also like
- HepatomaDocument33 pagesHepatomaRozen RyuhaNo ratings yet
- Mcu Siloam & ProdiaDocument2 pagesMcu Siloam & ProdiaWidyaM putriNo ratings yet
- Hepatitis B Dan C - PresentasiDocument31 pagesHepatitis B Dan C - PresentasiRatu anisa Fadila balgisNo ratings yet
- Child-Pugh Score: Patient Name: - DateDocument3 pagesChild-Pugh Score: Patient Name: - DateGede Eka Putra NugrahaNo ratings yet
- Clinical Manifestations, Medical Diagnosis, Diagnostic Test: Ocon Elmarie BDocument9 pagesClinical Manifestations, Medical Diagnosis, Diagnostic Test: Ocon Elmarie BAbcd TolibasNo ratings yet
- ASCP Recalls 5Document9 pagesASCP Recalls 5Cristina Vergel De DiosNo ratings yet
- Hepatitis B & C, Alamanda GarutDocument43 pagesHepatitis B & C, Alamanda GarutAndi Putra RegardboyNo ratings yet
- Liver Lesions Guide and Multiple Liver Nodule CaseDocument13 pagesLiver Lesions Guide and Multiple Liver Nodule CaseRozen RyuhaNo ratings yet
- Theme 2Document12 pagesTheme 2KunduzNo ratings yet
- Pre Employment Medical Examination Form - RS - pt.FIDocument3 pagesPre Employment Medical Examination Form - RS - pt.FINooB GAMING100% (1)
- Cookeville Regional Medical Center Severe Sepsis/Septic Shock Clinical PathwayDocument4 pagesCookeville Regional Medical Center Severe Sepsis/Septic Shock Clinical PathwayArnelli HutagalungNo ratings yet
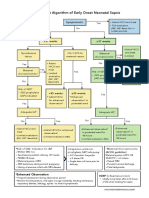
- Neonatal Sepsis Algorithm2Document1 pageNeonatal Sepsis Algorithm2CHIERBEENo ratings yet
- The HBV Pipeline and What The SIG Can OfferDocument29 pagesThe HBV Pipeline and What The SIG Can OfferTran Thanh NamNo ratings yet
- Heptits Chronic BDocument31 pagesHeptits Chronic BNicko Junior FakdawerNo ratings yet
- Form RR Nakes HorisonDocument13 pagesForm RR Nakes HorisondedehNo ratings yet
- Yerevan APASL STC: Future of Hepatology Treatment Indications and Therapeutic End-PointsDocument33 pagesYerevan APASL STC: Future of Hepatology Treatment Indications and Therapeutic End-PointsChristopher Surya SuwitaNo ratings yet
- Lab Ping BaruDocument1 pageLab Ping Baruaset asetNo ratings yet
- NavelbinDocument48 pagesNavelbinanang atmojoNo ratings yet
- MLS (ASCPi) Recall Questions: June 2017Document11 pagesMLS (ASCPi) Recall Questions: June 2017Astrud Labrador100% (3)
- RFP Calculator - v3.1 - 15 Jul 2021Document70 pagesRFP Calculator - v3.1 - 15 Jul 2021saanju87No ratings yet
- NCP IntravenaDocument12 pagesNCP Intravenawulan NurfaddilahNo ratings yet
- EASL 2017 Hepatitis B PowerpointDocument25 pagesEASL 2017 Hepatitis B Powerpointiq_dianaNo ratings yet
- Liver Disease: Understanding Cirrhosis Causes, Stages and TreatmentDocument48 pagesLiver Disease: Understanding Cirrhosis Causes, Stages and TreatmentNuthahai SimangernNo ratings yet
- Hepatitis Virus, Liver Cirrhosis and Hepatoma (HCCDocument61 pagesHepatitis Virus, Liver Cirrhosis and Hepatoma (HCCYun ZhaNo ratings yet
- FORMS Reseta and All Forms 2022 PDFDocument16 pagesFORMS Reseta and All Forms 2022 PDFJessa MaeNo ratings yet
- Clinical Pathway DEMAM BERDARAHDocument2 pagesClinical Pathway DEMAM BERDARAHHilda FebriaNo ratings yet
- Brochure Canine Babesia AbDocument2 pagesBrochure Canine Babesia AbPatricia LupuNo ratings yet
- Quantitative HBcrAg and HBcAb versus HBsAg and HBV DNA in predicting liver fibrosis levels of chronic hepatitis B patientsDocument11 pagesQuantitative HBcrAg and HBcAb versus HBsAg and HBV DNA in predicting liver fibrosis levels of chronic hepatitis B patientsbread maniacNo ratings yet
- Surgery PearlsDocument2 pagesSurgery Pearlspatriciaatan1497No ratings yet
- Managing Chronic Hepatitis BDocument31 pagesManaging Chronic Hepatitis BRahmayantiYuliaNo ratings yet
- Puskesmas Bluto: Pemerintah Kabupaten Sumenep Dinas Kesehatan Jl. Raya Bluto No. 13 SumenepDocument4 pagesPuskesmas Bluto: Pemerintah Kabupaten Sumenep Dinas Kesehatan Jl. Raya Bluto No. 13 SumenepPurnomo WirawanNo ratings yet
- Hepatitis B Cases StudiesDocument53 pagesHepatitis B Cases Studiesrieza_huseinNo ratings yet
- Hematologi: Laboratorium Laboratorium Klinik Pratama Pmi Boyolali Klinik Pramita Pmi BoyolaliDocument1 pageHematologi: Laboratorium Laboratorium Klinik Pratama Pmi Boyolali Klinik Pramita Pmi BoyolaliniaNo ratings yet
- SEPSIS Rev 21092020Document46 pagesSEPSIS Rev 21092020rani asfiyaNo ratings yet
- Pemeriksaan Hasil: Hemoglobin Gula Darah Sewaktu Gula Darah Puasa Gula Darg 2 Jam PP Asam Urat Golongan DarahDocument3 pagesPemeriksaan Hasil: Hemoglobin Gula Darah Sewaktu Gula Darah Puasa Gula Darg 2 Jam PP Asam Urat Golongan Darahheni sundariNo ratings yet
- Emergency Case TemplateDocument16 pagesEmergency Case TemplateJacky JunaediNo ratings yet
- Hepatitis BUMIL, Materi DR - Emil, SP - Pd.Document36 pagesHepatitis BUMIL, Materi DR - Emil, SP - Pd.yuliyanto.efendiNo ratings yet
- Case DiscussionDocument29 pagesCase DiscussionTjendonohariantoNo ratings yet
- Diagnosis: HCC Dapat Didiagnosa Dengan Cara: - Presentasi Klinis - Investigation - StagingDocument10 pagesDiagnosis: HCC Dapat Didiagnosa Dengan Cara: - Presentasi Klinis - Investigation - Stagingnabil abdurrahmanNo ratings yet
- Diabetes Control PackageDocument1 pageDiabetes Control PackageAbdul Kalam AnsariNo ratings yet
- Management of Patients With Chronic Hepatitis BDocument70 pagesManagement of Patients With Chronic Hepatitis BluamsmarinsNo ratings yet
- L0. Detecting Hepatitis BDocument9 pagesL0. Detecting Hepatitis BAssary RivaNo ratings yet
- Characteristics of Liver Marker Indicators Cholecystokinin-8 and Gastrin-17 in Patients With V Virus Liver CirrhosisDocument5 pagesCharacteristics of Liver Marker Indicators Cholecystokinin-8 and Gastrin-17 in Patients With V Virus Liver CirrhosisCentral Asian StudiesNo ratings yet
- Blood TestDocument1 pageBlood TestJoshua UriNo ratings yet
- Child BDocument22 pagesChild BFabrizio RomanoNo ratings yet
- CP HivDocument2 pagesCP Hivmelania sea kedangNo ratings yet
- Neonatology Guide for Maternal and Newborn CareDocument8 pagesNeonatology Guide for Maternal and Newborn Caremymamym100% (1)
- 1 s2.0 S201325141500022X MainDocument8 pages1 s2.0 S201325141500022X MainSri Widia NingsihNo ratings yet
- HBV GP PerspectiveDocument42 pagesHBV GP PerspectivePankaj IngleNo ratings yet
- CH - Khairi Ghani/ 5 y.o/MR 1.43.50.96 Admitted On July 27 2019 at 10.00 PMDocument10 pagesCH - Khairi Ghani/ 5 y.o/MR 1.43.50.96 Admitted On July 27 2019 at 10.00 PMmonyet65No ratings yet
- UK Biologics Checklist May 2014Document2 pagesUK Biologics Checklist May 2014Dr Sneha's Skin and Allergy Clinic IndiaNo ratings yet
- Formulir LabDocument1 pageFormulir LabADMEN PAGELARANNo ratings yet
- Serological Markers For Viral HepatitisDocument29 pagesSerological Markers For Viral HepatitisMariah ValdehuezaNo ratings yet
- Nama Pasien: Kelamin: CM: Tanggal Lahir: BBL (GR) : Telp: Tanggal Masuk: DPJP: Tanggal Operasi I: II III IV DiagnosaDocument3 pagesNama Pasien: Kelamin: CM: Tanggal Lahir: BBL (GR) : Telp: Tanggal Masuk: DPJP: Tanggal Operasi I: II III IV DiagnosaArief Tirtana PutraNo ratings yet
- Case Studies - Chronic Hepatitis B: Barbara Leggett RBWHDocument26 pagesCase Studies - Chronic Hepatitis B: Barbara Leggett RBWHalia eltayebNo ratings yet
- Management of Type 2 Diabetes Mellitus: Quick Reference Guide For Healthcare ProfessionalsDocument8 pagesManagement of Type 2 Diabetes Mellitus: Quick Reference Guide For Healthcare ProfessionalsAqilah SyafiqahNo ratings yet
- RAD RLE Guide -Written RequirementsDocument19 pagesRAD RLE Guide -Written RequirementsRoswell Almodiel EscaranNo ratings yet
- EASL 2017 Clinical Practice Guidelines on Managing Hepatitis BDocument34 pagesEASL 2017 Clinical Practice Guidelines on Managing Hepatitis BSabrinaQurrotaayunNo ratings yet
- Blood Banking Case StudyDocument7 pagesBlood Banking Case StudyStephanie Kate ArriolaNo ratings yet
- Zheng - 2022tacrolimus en NKLDocument14 pagesZheng - 2022tacrolimus en NKLOscar SanchezNo ratings yet
- 352 22 PDFDocument14 pages352 22 PDFAhmad JazmiNo ratings yet
- CHT Lfa Girls Z 6 2 PDFDocument1 pageCHT Lfa Girls Z 6 2 PDFAhmad JazmiNo ratings yet
- CHT Wfa Girls P 6 2Document1 pageCHT Wfa Girls P 6 2Ahmad JazmiNo ratings yet
- Acute Diverticulitis-GcpDocument85 pagesAcute Diverticulitis-Gcpkuro hanabusaNo ratings yet
- Short Bowel Syndrome: A Review of LiteratureDocument19 pagesShort Bowel Syndrome: A Review of LiteratureZakirNo ratings yet
- MukosaDocument3 pagesMukosaMarf PennyNo ratings yet
- (23008733 - Annals of Animal Science) Effect of Sodium Butyrate On Intestinal Health of Poultry - A ReviewDocument13 pages(23008733 - Annals of Animal Science) Effect of Sodium Butyrate On Intestinal Health of Poultry - A ReviewJesus CameroNo ratings yet
- Approach to Chronic DiarrheaDocument40 pagesApproach to Chronic DiarrheaJheng-Dao YangNo ratings yet
- GI Assessment Diagnosis and Case StudiesDocument66 pagesGI Assessment Diagnosis and Case StudiesCarla CalsadoNo ratings yet
- ZOOLOGyDocument144 pagesZOOLOGytemp93630No ratings yet
- Digestion 14 MariebDocument69 pagesDigestion 14 Mariebapi-285078865No ratings yet
- Managing The Bladder and Bowel in Spina BifidaDocument77 pagesManaging The Bladder and Bowel in Spina BifidaSeptinaAyuSamsiati100% (1)
- Defecation ReflexDocument31 pagesDefecation ReflexNayyer Khan100% (1)
- Accuracy of ASGE Criteria For The Prediction of Choledocholithiasis 2016Document6 pagesAccuracy of ASGE Criteria For The Prediction of Choledocholithiasis 2016DannyNo ratings yet
- Zollinger EllisonDocument2 pagesZollinger EllisonFrama Intan MiguelNo ratings yet
- Appendicitis Case StudyDocument6 pagesAppendicitis Case StudyKimxi Chiu LimNo ratings yet
- @ (White Paper - Cut-Off) RS85 - S-Shearwave Imaging LiverDocument10 pages@ (White Paper - Cut-Off) RS85 - S-Shearwave Imaging LiverHajjab AnasNo ratings yet
- Cholecystectomy 4 PrintingDocument19 pagesCholecystectomy 4 PrintingKyle Punzalan100% (2)
- Nutrition in Animals: DigestionDocument13 pagesNutrition in Animals: DigestionKalpavriksha1974No ratings yet
- Constipation 508Document12 pagesConstipation 508Shishir Kumar SinghNo ratings yet
- Chapter 16 The Gastrointestinal and Renal SystemDocument4 pagesChapter 16 The Gastrointestinal and Renal SystemKhanh HoangNo ratings yet
- GI Answer Key Part 1Document5 pagesGI Answer Key Part 1Nom NomNo ratings yet
- Cross-Sectional Imaging of Intrahepatic Cholangiocarcinoma: Development, Growth, Spread, and PrognosisDocument12 pagesCross-Sectional Imaging of Intrahepatic Cholangiocarcinoma: Development, Growth, Spread, and PrognosisNikos SerifisNo ratings yet
- Modul Bronkoesofagologi - 6. Disfagia OrofaringDocument31 pagesModul Bronkoesofagologi - 6. Disfagia OrofaringNi Putu Apriliantini Arleni Putri 1802511045No ratings yet
- Hepatobiliary SystemDocument18 pagesHepatobiliary SystemBinita ShresthaNo ratings yet
- Diagnosis and Management of Benign Gastric and Duodenal DiseaseDocument16 pagesDiagnosis and Management of Benign Gastric and Duodenal DiseaseMaría Lourdes Rodríguez ZavalaNo ratings yet
- Digestion and Absorption Class 11 Notes Biology Chapter 16 SummaryDocument6 pagesDigestion and Absorption Class 11 Notes Biology Chapter 16 SummaryBrijesh BalachandranNo ratings yet
- History Made Easy NotesDocument3 pagesHistory Made Easy NotesTahir AliNo ratings yet
- Obs JauDocument22 pagesObs JauRavi GuptaNo ratings yet
- Journey Through DigestionDocument4 pagesJourney Through DigestionJoy JonesNo ratings yet
- CLONORCHISDocument23 pagesCLONORCHISodysseyfairy2739No ratings yet
- Antaomy of GITDocument5 pagesAntaomy of GITMike GNo ratings yet
- Barium MealDocument19 pagesBarium MealHamzeh AlmasriNo ratings yet