You might also like
- Mediterranean Diet Cookbook for Beginners: Unlock the Health Benefits of the Mediterranean Diet with Easy and Delicious Recipes for Everyday Eating!From EverandMediterranean Diet Cookbook for Beginners: Unlock the Health Benefits of the Mediterranean Diet with Easy and Delicious Recipes for Everyday Eating!No ratings yet
- Migraine Diet: A 4-Week Step-by-Step Guide for Women, With Recipes and a Meal PlanFrom EverandMigraine Diet: A 4-Week Step-by-Step Guide for Women, With Recipes and a Meal PlanNo ratings yet
- Hypocalcemia, (Low Blood Calcium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHypocalcemia, (Low Blood Calcium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Esophageal Motility Disorder, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandEsophageal Motility Disorder, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Hypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandHypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- A Simple Guide to Pick Disease, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Pick Disease, Diagnosis, Treatment and Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Vasculitis Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandVasculitis Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Complete Guide to the Very Low-Calorie Diet: Lose Excess Body Weight While Enjoying Your Favorite Foods.From EverandComplete Guide to the Very Low-Calorie Diet: Lose Excess Body Weight While Enjoying Your Favorite Foods.No ratings yet
- The Harvard Volunteers In Europe Personal Records Of Experience In Military, Ambulance, And Hospital ServiceFrom EverandThe Harvard Volunteers In Europe Personal Records Of Experience In Military, Ambulance, And Hospital ServiceNo ratings yet
- Vegetarian Nutrition 101: The Science Behind a Plant-Based Diet: The Vegetarian Kitchen Series, #3From EverandVegetarian Nutrition 101: The Science Behind a Plant-Based Diet: The Vegetarian Kitchen Series, #3No ratings yet
- Breast Cancer: Melatonin Helps to: Prevent Cancer, Avoid Drug Resistance, Stop MetastasisFrom EverandBreast Cancer: Melatonin Helps to: Prevent Cancer, Avoid Drug Resistance, Stop MetastasisNo ratings yet
- Paleo Diet Made Easy: Paleo Diet Recipes For Burn Fat Fast, Remove Cellulite, Eliminate Toxins & Feel GreatFrom EverandPaleo Diet Made Easy: Paleo Diet Recipes For Burn Fat Fast, Remove Cellulite, Eliminate Toxins & Feel GreatNo ratings yet
- Guidelines for Measuring Household and Individual Dietary DiversityFrom EverandGuidelines for Measuring Household and Individual Dietary DiversityNo ratings yet
- Introduction to Fats and Oils: Cooking Fats and Oils for Good HealthFrom EverandIntroduction to Fats and Oils: Cooking Fats and Oils for Good HealthRating: 3 out of 5 stars3/5 (1)
- Lactose IntoleranceDocument19 pagesLactose IntolerancehafeezmmlNo ratings yet
- Chap1 Introduction To Nutritional AssessmentDocument32 pagesChap1 Introduction To Nutritional AssessmentAbdi Khalaq Ali Hashi100% (1)
- Nutrition and Renal DiseaseDocument6 pagesNutrition and Renal DiseasefranzcatchieNo ratings yet
- Wheat Gluten and Health Powerpoint PresentationDocument22 pagesWheat Gluten and Health Powerpoint PresentationCeliaNo ratings yet
- Diabetes: Causes, Symptoms and TreatmentsDocument4 pagesDiabetes: Causes, Symptoms and TreatmentsAbdullah BazryNo ratings yet
- Type 2 DiabetesDocument543 pagesType 2 DiabetesSofija VukadinovićNo ratings yet
- Diet Therapy 2019Document7 pagesDiet Therapy 2019R-Chian Jose GermanpNo ratings yet
- Grave'S Disease: Farida Ulfa 1510211057Document11 pagesGrave'S Disease: Farida Ulfa 1510211057farida ulfaNo ratings yet
- DMDocument20 pagesDMKC PalattaoNo ratings yet
- Australian Dietary Guidelines SummaryDocument10 pagesAustralian Dietary Guidelines SummaryRNo ratings yet
- "Senza Il Pane Tutto Diventa Orfano": Gluten Sensitivity, Coeliac DiseaseDocument87 pages"Senza Il Pane Tutto Diventa Orfano": Gluten Sensitivity, Coeliac DiseaseAmy Ruskoski HendersonNo ratings yet
- 9 Diabetes Mellitus PHYSIOLOGYDocument22 pages9 Diabetes Mellitus PHYSIOLOGYEman KhammasNo ratings yet
- Hyperlipidemia: Revised: October 4, 2019Document7 pagesHyperlipidemia: Revised: October 4, 2019HannaNo ratings yet
- Psychiatric Effects of ThyroidDocument9 pagesPsychiatric Effects of ThyroidJosetta WhitneyNo ratings yet
- Antiphospholipid SyndromeDocument16 pagesAntiphospholipid Syndrometal26No ratings yet
- Course 4 2019 Hypoglicemia HyperuricemiaDocument57 pagesCourse 4 2019 Hypoglicemia HyperuricemiaAmelia PricopNo ratings yet
- 5: Diarrhea and Constipation: MedicineDocument7 pages5: Diarrhea and Constipation: MedicineDia DimayugaNo ratings yet
- ProlactinDocument2 pagesProlactinOlivera VukovicNo ratings yet
- Thyroid Disease AlgorithmsDocument29 pagesThyroid Disease AlgorithmsGoh Chong Aik100% (2)
- Celiac DiseaseDocument53 pagesCeliac DiseaseAndrew Fong100% (1)
- PeripheralDocument25 pagesPeripheralMans FansNo ratings yet
- Stress and HormonesDocument5 pagesStress and HormonesDiana Espinoza SegoviaNo ratings yet
- Basic Concept of Human RightDocument15 pagesBasic Concept of Human RightDwika HerdykiawanNo ratings yet
- Liver Function Testing PDFDocument2 pagesLiver Function Testing PDFRajesh KumarNo ratings yet
- Pituitary Tumors Engleza 2Document89 pagesPituitary Tumors Engleza 2Achmad Harun MuchsinNo ratings yet
- Metabolism and AtpDocument20 pagesMetabolism and AtpAbdul Rafay ShaikhNo ratings yet
- BPH by SamuelDocument33 pagesBPH by SamuelIan Smith AkampuriraNo ratings yet
- Breast Pain - History TakingDocument6 pagesBreast Pain - History TakingValencia FooNo ratings yet
- Ped Gi Handbook For Doctor, Medical Student, NurseDocument62 pagesPed Gi Handbook For Doctor, Medical Student, NurseLikoh TimothyNo ratings yet
- Human and Health Rights in Relation To Sustainable2Document17 pagesHuman and Health Rights in Relation To Sustainable2ptkabworldNo ratings yet
- Insulin HandbookDocument67 pagesInsulin HandbookThits SarNo ratings yet
- 16 - Hypo and HyperthyroidismDocument58 pages16 - Hypo and HyperthyroidismRouda Abdulla100% (1)
- Metabolic Syndrome For PublishingDocument18 pagesMetabolic Syndrome For PublishingSatyendra Ojha100% (3)
- Ebs3 - Electronic Braking SystemDocument111 pagesEbs3 - Electronic Braking SystemIslam ShoukryNo ratings yet
- Orbitrol Repairing 2Document14 pagesOrbitrol Repairing 2Islam ShoukryNo ratings yet
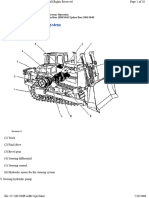
- Service Manual D8R 9EM Halaman 893 910Document11 pagesService Manual D8R 9EM Halaman 893 910Islam ShoukryNo ratings yet
- Priorety and Orbitrol CircuitDocument8 pagesPriorety and Orbitrol CircuitIslam ShoukryNo ratings yet
- EUROPART Inter Catalog BaDocument2 pagesEUROPART Inter Catalog BaIslam ShoukryNo ratings yet
- Orbitrol Repairing 2Document25 pagesOrbitrol Repairing 2Islam ShoukryNo ratings yet
- Char-Lynn: Steering Control UnitsDocument4 pagesChar-Lynn: Steering Control UnitsIslam ShoukryNo ratings yet
- Orbitrol Repairing1Document30 pagesOrbitrol Repairing1Islam ShoukryNo ratings yet
- Service Manual D8R 9EM Halaman 893 910Document18 pagesService Manual D8R 9EM Halaman 893 910Islam ShoukryNo ratings yet
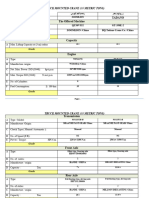
- Truck Mounted Crane (30 Metric Tons) : مصر ك مي ل سوي ورز ت رجب مو Tadano The Offered MachineDocument6 pagesTruck Mounted Crane (30 Metric Tons) : مصر ك مي ل سوي ورز ت رجب مو Tadano The Offered MachineIslam ShoukryNo ratings yet
- Two All Terrain CraneDocument13 pagesTwo All Terrain CraneIslam ShoukryNo ratings yet
- معدل one truck 60Document13 pagesمعدل one truck 60Islam ShoukryNo ratings yet
- Two All Terrain CraneDocument24 pagesTwo All Terrain CraneIslam ShoukryNo ratings yet
- Grade: The Offered MachineDocument15 pagesGrade: The Offered MachineIslam ShoukryNo ratings yet
- SEMIDocument2 pagesSEMIIslam ShoukryNo ratings yet
- معدل two truck 30Document14 pagesمعدل two truck 30Islam ShoukryNo ratings yet
- SEMIDocument4 pagesSEMIIslam ShoukryNo ratings yet
- KONECRANESDocument3 pagesKONECRANESIslam ShoukryNo ratings yet
- KALMARDocument2 pagesKALMARIslam ShoukryNo ratings yet
- SEMIDocument2 pagesSEMIIslam ShoukryNo ratings yet
- DTFR Liste EnglishDocument12 pagesDTFR Liste EnglishIslam ShoukryNo ratings yet
- DTFR Liste EnglishDocument3 pagesDTFR Liste EnglishIslam ShoukryNo ratings yet
- Maintenance Schedule Hilux 2016 PresentDocument1 pageMaintenance Schedule Hilux 2016 PresentIslam ShoukryNo ratings yet
- DTFR Liste EnglishDocument3 pagesDTFR Liste EnglishIslam ShoukryNo ratings yet
- Maintenance Schedule Hilux 2016 PresentDocument1 pageMaintenance Schedule Hilux 2016 PresentIslam ShoukryNo ratings yet
- Electrical Graphic SymbolDocument5 pagesElectrical Graphic SymbolIslam ShoukryNo ratings yet
- Sample TCP - GraceGuitguitenDocument4 pagesSample TCP - GraceGuitguitenLauren JalandoniNo ratings yet
- Nursing Care PlanDocument2 pagesNursing Care Planmjoie_baby6568470100% (6)
- PhilHealth Circular No. 0035, s.2013 Annex 1 List of Medical Case RatesDocument111 pagesPhilHealth Circular No. 0035, s.2013 Annex 1 List of Medical Case RatesChrysanthus Herrera80% (5)
- Homeo-11 RrUBRICSDocument32 pagesHomeo-11 RrUBRICSRashid MahmoodNo ratings yet
- Sexton 2011Document19 pagesSexton 2011koushikNo ratings yet
- Urology1 UPDATEDDocument44 pagesUrology1 UPDATEDmarwanNo ratings yet
- Health History by Gordon's Functional Health PatternDocument7 pagesHealth History by Gordon's Functional Health PatternAveriAlonzoNo ratings yet
- Hospital Pharmacy Activity 6, 7Document9 pagesHospital Pharmacy Activity 6, 7Alyssa Marie Petonio BialaNo ratings yet
- Neuropathy and DMDocument41 pagesNeuropathy and DMsheryl yangNo ratings yet
- Urinary Catheterization PPT LectureDocument43 pagesUrinary Catheterization PPT LectureSusan MaglaquiNo ratings yet
- Katz Index of Independence in Activities of Daily LivingDocument1 pageKatz Index of Independence in Activities of Daily LivingGEN ERIGBUAGASNo ratings yet
- Group 1 Nursing Diagnosis FinalDocument59 pagesGroup 1 Nursing Diagnosis FinalChristian Angelo LeonorNo ratings yet
- Phinma Cagayan de Oro CollegeDocument14 pagesPhinma Cagayan de Oro CollegeYasmin MagsaysayNo ratings yet
- Medical Facts and Mcq's Urology MCQDocument14 pagesMedical Facts and Mcq's Urology MCQSmart Urosurgeon100% (2)
- Evidence Statement Anal Incontinence Flowchart PDFDocument2 pagesEvidence Statement Anal Incontinence Flowchart PDFsilkofosNo ratings yet
- Operative Vaginal DeliveryDocument26 pagesOperative Vaginal DeliveryZurya UdayanaNo ratings yet
- Full Paper - PUBLIC HEALTH CHALLENGES DUE TO INSUFFICIENT PUBLIC TOILET IN DHAKA CITY OF BANGLADESHDocument19 pagesFull Paper - PUBLIC HEALTH CHALLENGES DUE TO INSUFFICIENT PUBLIC TOILET IN DHAKA CITY OF BANGLADESHTanvir RezaNo ratings yet
- Lower Urinary Tract CancerDocument18 pagesLower Urinary Tract CancerFábio RanyeriNo ratings yet
- ABC Dictionary of Urinary SystemDocument26 pagesABC Dictionary of Urinary Systemaby_romero9750% (2)
- LearnerGuide 1 - CHCCCS015 - CHCCCS023 - HLTAAP001Document145 pagesLearnerGuide 1 - CHCCCS015 - CHCCCS023 - HLTAAP001Raju Subedi80% (5)
- Micturition 2022Document20 pagesMicturition 2022Mohammad zreadNo ratings yet
- Preboard Nursing ExamsDocument91 pagesPreboard Nursing ExamsJimmalyn Santos100% (1)
- The Psychological Study of The Sonnet 129Document8 pagesThe Psychological Study of The Sonnet 129SARWALNo ratings yet
- Urine Dribbling PDFDocument3 pagesUrine Dribbling PDFAslam MemonNo ratings yet
- Katz Index of I.A.D.L - SalimbagatDocument1 pageKatz Index of I.A.D.L - SalimbagatChristine Pialan SalimbagatNo ratings yet
- 10 1 1 115Document151 pages10 1 1 115Angela TorrenteNo ratings yet
- Benign Prostatic Hyperplasia: A Clinical ReviewDocument5 pagesBenign Prostatic Hyperplasia: A Clinical Reviewexpired monkeyNo ratings yet
- BPH NCPDocument8 pagesBPH NCPJan Michael ArtiagaNo ratings yet
- Botox Best Practices Ebook PDFDocument19 pagesBotox Best Practices Ebook PDFSuhair F Diebes0% (1)
- On The Viewbox: Dermoid Cyst in The Lumbosacral Region: Radiographic FindingsDocument6 pagesOn The Viewbox: Dermoid Cyst in The Lumbosacral Region: Radiographic FindingsWildaHanimNo ratings yet