You might also like
- The Irrefutable Laws of Leadership SummaryDocument6 pagesThe Irrefutable Laws of Leadership Summarycoachersland100% (3)
- PlatyhelminthesDocument17 pagesPlatyhelminthesLuisa San SebastianNo ratings yet
- Sample Leopold MatrixDocument7 pagesSample Leopold Matrixshreeja07No ratings yet
- Animal Kingdom: Basis of ClassificationDocument15 pagesAnimal Kingdom: Basis of ClassificationChaitali Deshmukh100% (1)
- Jose Noel Meza-Perez, A029 269 568 (BIA Feb. 28, 2011)Document3 pagesJose Noel Meza-Perez, A029 269 568 (BIA Feb. 28, 2011)Immigrant & Refugee Appellate Center, LLCNo ratings yet
- Phylum NematodaDocument24 pagesPhylum NematodaKaten KyoukotsuNo ratings yet
- The Nematodes Nema: Thread, Oides: FormDocument20 pagesThe Nematodes Nema: Thread, Oides: FormChandra Adie100% (1)
- CESTODE - PPT MajorDocument92 pagesCESTODE - PPT MajorJOSEPH NDERITU100% (2)
- Animal Diversity SummaryDocument24 pagesAnimal Diversity SummaryAna Melissa BarsalloNo ratings yet
- Nationalism in India - PadhleNotes PDFDocument10 pagesNationalism in India - PadhleNotes PDFTejpal SinghNo ratings yet
- Injera Production and Export Business PlanDocument50 pagesInjera Production and Export Business PlanTumim84% (44)
- Difference Between Heat and TemperatureDocument8 pagesDifference Between Heat and TemperatureMarivic MirandaNo ratings yet
- Soil MechanicsDocument117 pagesSoil MechanicsChiranjaya HulangamuwaNo ratings yet
- ALS Metallurgy - Gold Extraction ProcessDocument8 pagesALS Metallurgy - Gold Extraction ProcessalxmalagaNo ratings yet
- Intestinal NematodesDocument88 pagesIntestinal NematodesVincent Manganaan100% (1)
- Math 7-4th QuarterDocument3 pagesMath 7-4th QuarterMarie Saren100% (2)
- R69 Sepulveda V PelaezDocument2 pagesR69 Sepulveda V PelaezfranceheartNo ratings yet
- Imam Mahdi and Jesus Christ - 2023 ADDocument290 pagesImam Mahdi and Jesus Christ - 2023 ADSyed AbidiNo ratings yet
- 6 Sigma 7 QC Tools Fmea DoeDocument19 pages6 Sigma 7 QC Tools Fmea Doeerkushagra100% (1)
- Major V Sem PracticalDocument12 pagesMajor V Sem Practicalmohitpatel18032003No ratings yet
- General Characteristics: NematodesDocument27 pagesGeneral Characteristics: NematodesJaica Mangurali Tumulak100% (1)
- 1111111111118th WeekDocument39 pages1111111111118th WeekayaamrsharfNo ratings yet
- Bio 320 Practical 7Document12 pagesBio 320 Practical 7MuhammadAsyraf50% (2)
- Acelomate Bilateral AnimalsDocument59 pagesAcelomate Bilateral AnimalsLiz HackettNo ratings yet
- Roundworms: An Introduction to the Phylum NematodaDocument35 pagesRoundworms: An Introduction to the Phylum Nematodabewildered-escapist-4301No ratings yet
- Entomology MergedDocument226 pagesEntomology MergedShanmathiNo ratings yet
- Platyhelminthes Flukes Trematoda Life CyclesDocument29 pagesPlatyhelminthes Flukes Trematoda Life CyclesRajkumar MandalNo ratings yet
- Phylum NematodaDocument5 pagesPhylum NematodaJara RogacionNo ratings yet
- Reproductive System Etc.Document29 pagesReproductive System Etc.Shadab HanafiNo ratings yet
- NemtodeGen 2023Document14 pagesNemtodeGen 2023Ming YanNo ratings yet
- TRIBLASTICADocument31 pagesTRIBLASTICAcircovaesterkaNo ratings yet
- Metazoa Phylogeny and ClassificationDocument105 pagesMetazoa Phylogeny and ClassificationMohamed TharwatNo ratings yet
- Invertebrate: Second Stage 2020-2021Document37 pagesInvertebrate: Second Stage 2020-2021Shaker MahmoodNo ratings yet
- Animal KingdomDocument47 pagesAnimal KingdomMeenal MeshramNo ratings yet
- Morphological Adaptation in Parasitic HelminthesDocument17 pagesMorphological Adaptation in Parasitic HelminthesVp SinghNo ratings yet
- Module 3 PDFDocument6 pagesModule 3 PDFLittle Miss CeeNo ratings yet
- Helminth ParasitesDocument95 pagesHelminth ParasitesAngieNo ratings yet
- Ascaris LumbricoidesDocument60 pagesAscaris Lumbricoidesobuekwechukwuemeka100% (2)
- Vermes 1platyhelminthesDocument36 pagesVermes 1platyhelminthessolifaNo ratings yet
- Phylum Platyhelminthes Phylum Nematoda Phylum MolluscaDocument44 pagesPhylum Platyhelminthes Phylum Nematoda Phylum MolluscaAngel FebiolaNo ratings yet
- Week 15Document4 pagesWeek 15DELOS SANTOS JESSIECAHNo ratings yet
- Helminthes: / Medical Laboratory TechnologyDocument17 pagesHelminthes: / Medical Laboratory Technologyصفا رياض محمد /مسائيNo ratings yet
- Phylum CtenophoraDocument23 pagesPhylum CtenophoramsnidanusratNo ratings yet
- Reviewer NematodaDocument4 pagesReviewer NematodaCarlo MendozaNo ratings yet
- Invertebrate: Second Stage 2020-2021Document37 pagesInvertebrate: Second Stage 2020-2021Shaker MahmoodNo ratings yet
- Phylum PlatyhelmenthisDocument3 pagesPhylum PlatyhelmenthisMA. LYN CASIPENo ratings yet
- Diversity Among Animals WisegotDocument36 pagesDiversity Among Animals WisegotDheera Nand100% (1)
- Cestodes NotesDocument27 pagesCestodes NotesShanmathiNo ratings yet
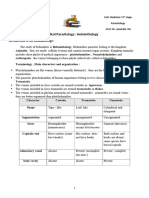
- Parasitology Dr Amal Helminthology Lec 1Document8 pagesParasitology Dr Amal Helminthology Lec 1Cosplay AccountNo ratings yet
- Parasitology Cestodes LectureDocument19 pagesParasitology Cestodes Lectureميمونه عبدالرحيم مصطفىNo ratings yet
- PLATYHELMINYHESDocument23 pagesPLATYHELMINYHESAnisa Kapti HanawiNo ratings yet
- Cestoidea:: CharactersDocument20 pagesCestoidea:: CharactersConNo ratings yet
- AttachmentDocument15 pagesAttachmentMamila TadNo ratings yet
- LACTURE 4 Nematodes and CestodesDocument25 pagesLACTURE 4 Nematodes and CestodesmuskanbakaliNo ratings yet
- CNIDARIADocument14 pagesCNIDARIAVanessa DacerNo ratings yet
- NematodaDocument30 pagesNematodaTagonna Di RaizelNo ratings yet
- Phylum PlatyhelminthesDocument6 pagesPhylum Platyhelminthesjuancho de mesa100% (2)
- Invertebrate ZoologyDocument16 pagesInvertebrate ZoologyRenz Francis SasaNo ratings yet
- Flatworms 1Document63 pagesFlatworms 1Budi AfriyansyahNo ratings yet
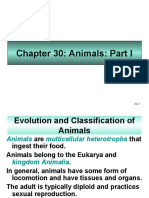
- Animals: Evolution and ClassificationDocument63 pagesAnimals: Evolution and ClassificationCassio RamosNo ratings yet
- Knowledge ReviewDocument81 pagesKnowledge ReviewAmr EldemardashNo ratings yet
- TapewormsDocument18 pagesTapewormsirish xNo ratings yet
- Nematodes: We're Everywhere!Document13 pagesNematodes: We're Everywhere!panks.79No ratings yet
- T. Parasitology Lec 4 CestodesDocument21 pagesT. Parasitology Lec 4 CestodesAbdalrhmanNo ratings yet
- Invertebrates of Medical and Veterinarary ImportanceDocument25 pagesInvertebrates of Medical and Veterinarary ImportanceobuekwechukwuemekaNo ratings yet
- Larva AssignmentDocument26 pagesLarva Assignmentnarendra singhNo ratings yet
- The Smaller Lophotrochozoan Phyla: Jasmin Godoy-Dela CruzDocument42 pagesThe Smaller Lophotrochozoan Phyla: Jasmin Godoy-Dela Cruzbread genieNo ratings yet
- EarthwormDocument11 pagesEarthwormFabian GuadarramaNo ratings yet
- Platheminthes. CestoideaDocument11 pagesPlatheminthes. CestoideaAdnan SosiNo ratings yet
- Phylum PlatyhelminthesDocument11 pagesPhylum PlatyhelminthesasajumuthmainahNo ratings yet
- Camp's Zoology by the Numbers: A comprehensive study guide in outline form for advanced biology courses, including AP, IB, DE, and college courses.From EverandCamp's Zoology by the Numbers: A comprehensive study guide in outline form for advanced biology courses, including AP, IB, DE, and college courses.No ratings yet
- Guide Number 5 My City: You Will Learn To: Describe A Place Tell Where You in The CityDocument7 pagesGuide Number 5 My City: You Will Learn To: Describe A Place Tell Where You in The CityLUIS CUELLARNo ratings yet
- Clustered File Systems With de Series ProductsDocument28 pagesClustered File Systems With de Series ProductsRaulcb1No ratings yet
- Book ReviewDocument3 pagesBook ReviewEilegnaNo ratings yet
- Assignment Article 2Document14 pagesAssignment Article 2Trend on Time0% (1)
- RelativeResourceManager PDFDocument113 pagesRelativeResourceManager PDFMuhammad Irfan SalahuddinNo ratings yet
- Assessment in Learning 1 Report (Formative Assessment)Document4 pagesAssessment in Learning 1 Report (Formative Assessment)Sampaga, Lovely Grace FerraroNo ratings yet
- AtropineDocument6 pagesAtropineNiluh Komang Putri PurnamantiNo ratings yet
- Long Term Recommendation Bata India LTD.: The Growth SprintDocument38 pagesLong Term Recommendation Bata India LTD.: The Growth SprintPANo ratings yet
- NEW GENERATION INTERNATIONAL SCHOOL SECOND UNIT TESTDocument4 pagesNEW GENERATION INTERNATIONAL SCHOOL SECOND UNIT TESTElmy ARNo ratings yet
- 01 Lezione 1 Working LifeDocument18 pages01 Lezione 1 Working LifeVincenzo Di PintoNo ratings yet
- Netflix PPT by OopsieanieeDocument12 pagesNetflix PPT by OopsieanieeAdhimurizkyrNo ratings yet
- Reaction to Bonifacio: Ang Unang Pangulo (2014) filmDocument2 pagesReaction to Bonifacio: Ang Unang Pangulo (2014) filmJose Mari King0% (1)
- English Language Communication Skills Lab Manual: Name Roll No. Branch SectionDocument39 pagesEnglish Language Communication Skills Lab Manual: Name Roll No. Branch SectionSurendrakumar ThotaNo ratings yet
- Readme P006Document7 pagesReadme P006paras99No ratings yet
- Theories of LearningDocument19 pagesTheories of LearningIndu GuptaNo ratings yet
- PalosliosDocument12 pagesPalosliossuwijak76797679No ratings yet
- Cover/ Application Letter: Preparing TheDocument14 pagesCover/ Application Letter: Preparing TheDiane Joy Fojas PanganibanNo ratings yet
- Caglar Araz CVDocument1 pageCaglar Araz CVAnonymous hSKPlVPNo ratings yet