You might also like
- Interpersonal SkillsDocument3 pagesInterpersonal Skillsluciana fardilaNo ratings yet
- International Journal of Nursing Sciences: Fateme Aghamohammadi, Behzad Imani, Mahnaz Moghadari KooshaDocument7 pagesInternational Journal of Nursing Sciences: Fateme Aghamohammadi, Behzad Imani, Mahnaz Moghadari Kooshaغادة العلوانيNo ratings yet
- Tugas 3Document6 pagesTugas 3La RikiNo ratings yet
- JFMPC 11 2828Document6 pagesJFMPC 11 2828Parth PatelNo ratings yet
- Interpersonal SkillsDocument2 pagesInterpersonal SkillsUmarameshKNo ratings yet
- 8 Quality Management in Health PDFDocument11 pages8 Quality Management in Health PDFFahim Ahmed TouqirNo ratings yet
- Assessment of Knowledge Attitude and Practices Regarding Awareness of Biomedical Waste Management Among Health Care Personnel A Cross-Sectional SurveyDocument5 pagesAssessment of Knowledge Attitude and Practices Regarding Awareness of Biomedical Waste Management Among Health Care Personnel A Cross-Sectional SurveyAms BeeNo ratings yet
- Waste Dental in IndiaDocument3 pagesWaste Dental in IndiaOktavia DewiNo ratings yet
- P 19-35 Liability and Quality Issues in Health Case Fifth EditionDocument30 pagesP 19-35 Liability and Quality Issues in Health Case Fifth EditionbillNo ratings yet
- Development and Psychometric Testing of A CompeteDocument6 pagesDevelopment and Psychometric Testing of A CompetethuongNo ratings yet
- Jurnal 4 PDFDocument19 pagesJurnal 4 PDFamaliaNo ratings yet
- Explaining Challenges of Obstetric Triage Structure: A Qualitative StudyDocument7 pagesExplaining Challenges of Obstetric Triage Structure: A Qualitative StudyEmy AstutiNo ratings yet
- Australian Critical Care: Research PaperDocument8 pagesAustralian Critical Care: Research PaperJaymi MacapagalNo ratings yet
- 1 Assessment 1 Instructions - Nursing Informatics in Health Care ..Document3 pages1 Assessment 1 Instructions - Nursing Informatics in Health Care ..Francois GonzalesNo ratings yet
- Hospital Management System Review ArticleDocument8 pagesHospital Management System Review ArticleriandhaniNo ratings yet
- A Study To Assess The Knowledge, Attitude and Practice of Undergraduate Nursing Students On Bio Medical Waste Management at Selected Nursing College in BhubaneswarDocument5 pagesA Study To Assess The Knowledge, Attitude and Practice of Undergraduate Nursing Students On Bio Medical Waste Management at Selected Nursing College in BhubaneswarEditor IJTSRDNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument8 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- IF004 Paper B Peter-Ilesanmi - EditedDocument6 pagesIF004 Paper B Peter-Ilesanmi - Editedhfecassignment solutionsNo ratings yet
- Evaluation of Nursing Information System: Nurses' PerspectivesDocument6 pagesEvaluation of Nursing Information System: Nurses' Perspectivesrobi kustiawanNo ratings yet
- Quality Tools and Strategy For Critical Alerts Process Improvements To Ensure Patient SafetyDocument8 pagesQuality Tools and Strategy For Critical Alerts Process Improvements To Ensure Patient SafetyMD LarasatiNo ratings yet
- AHM 540 - TestsDocument67 pagesAHM 540 - Testspraveen1510No ratings yet
- Multiple Choice Questions in Healthcare QualityFrom EverandMultiple Choice Questions in Healthcare QualityRating: 4 out of 5 stars4/5 (8)
- JFMPC 4 519Document6 pagesJFMPC 4 519yuniaNo ratings yet
- Knowledge, Attitude and Practice TowardsDocument19 pagesKnowledge, Attitude and Practice TowardsCory Artika ManurungNo ratings yet
- Ray2021 AssessmentOfTheirTrainingIngastroDocument11 pagesRay2021 AssessmentOfTheirTrainingIngastroNidhin MathewNo ratings yet
- BMATs Predictive Validity For Medical School Perf 230919 225056Document13 pagesBMATs Predictive Validity For Medical School Perf 230919 225056Thakoon TtsNo ratings yet
- JonqpsDocument8 pagesJonqpsShreya PurkaitNo ratings yet
- 1 s2.0 S0255085721001420 MainDocument3 pages1 s2.0 S0255085721001420 MainYosep SeptiawanNo ratings yet
- International Journal of Nursing Sciences: Jung Hee Kim, Jung Lim Lee, Eun Man KimDocument7 pagesInternational Journal of Nursing Sciences: Jung Hee Kim, Jung Lim Lee, Eun Man KimAnna FadhilaNo ratings yet
- Research Paper 2Document2 pagesResearch Paper 2Kiran KawareNo ratings yet
- Workplace Silence BehaviorDocument12 pagesWorkplace Silence Behaviornaveed ahmadNo ratings yet
- Quality Assurance and Control FinalDocument37 pagesQuality Assurance and Control FinalManeta Linnys DzaumaNo ratings yet
- IPE Interprofessional EducationDocument10 pagesIPE Interprofessional EducationdewaNo ratings yet
- Modification of Calgary Cambridge For Indonesian Medical Students: Communication GuidelinesDocument9 pagesModification of Calgary Cambridge For Indonesian Medical Students: Communication GuidelinesIJPHSNo ratings yet
- Factors Affecting The Successful Implementation ofDocument13 pagesFactors Affecting The Successful Implementation ofCj AlmazanNo ratings yet
- Total Quality ImprovementDocument21 pagesTotal Quality ImprovementMar DiyanNo ratings yet
- Jurnal Week 8 - Usability EvaluationDocument7 pagesJurnal Week 8 - Usability EvaluationHaris FirmansyahNo ratings yet
- CRM Result Pre and PostDocument14 pagesCRM Result Pre and PostRaditya TaslimNo ratings yet
- Chapter 17: Evidence-Based Practice: Strategies For Nursing Leaders Huber: Leadership & Nursing Care Management, 6th EditionDocument9 pagesChapter 17: Evidence-Based Practice: Strategies For Nursing Leaders Huber: Leadership & Nursing Care Management, 6th EditionLauren FavelaNo ratings yet
- Articulo de PracticaDocument10 pagesArticulo de PracticaAndrea RamirezNo ratings yet
- Effectiveness of Video Assisted Teaching Program On Segregation and Handling of Biomedical Waste Among Health Care Workers.Document10 pagesEffectiveness of Video Assisted Teaching Program On Segregation and Handling of Biomedical Waste Among Health Care Workers.International Journal of Innovative Science and Research TechnologyNo ratings yet
- A Study To Assess The Effectiveness of Structure Teaching Programme On Knowledge Regarding Biomedical Waste Management Among First Year UG Nursing Students From Selected Nursing Colleges, ChandrapurDocument3 pagesA Study To Assess The Effectiveness of Structure Teaching Programme On Knowledge Regarding Biomedical Waste Management Among First Year UG Nursing Students From Selected Nursing Colleges, ChandrapurInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Declaración de Consenso Sobre El Contenido de Los Currículos de Razonamiento Clínico en La Educación Médica de Pregrado 2020 INGLESDocument9 pagesDeclaración de Consenso Sobre El Contenido de Los Currículos de Razonamiento Clínico en La Educación Médica de Pregrado 2020 INGLESjaldoquiNo ratings yet
- 2022 Article 898Document14 pages2022 Article 898Ivan MaximusNo ratings yet
- Medical Staff Satisfaction Survey in A Makeshift Emergency Pandemic Covid Hospital - September - 2022 - 2012312667 - 4023723Document3 pagesMedical Staff Satisfaction Survey in A Makeshift Emergency Pandemic Covid Hospital - September - 2022 - 2012312667 - 4023723sanjay yadavNo ratings yet
- Competence Assessment of Nursing Graduates of Jordanian UniversitiesDocument9 pagesCompetence Assessment of Nursing Graduates of Jordanian UniversitiessukrangNo ratings yet
- Kompetensi PerawatDocument7 pagesKompetensi Perawat們禮儀鐵No ratings yet
- Utility of Work Based Assessment Among Surgical Residents: A Systematic Literature ReviewDocument8 pagesUtility of Work Based Assessment Among Surgical Residents: A Systematic Literature ReviewUsama AzizNo ratings yet
- RelatórioDocument7 pagesRelatórioceciliapmcNo ratings yet
- Matrix Method Literature Review ExampleDocument5 pagesMatrix Method Literature Review Exampleafdtygyhk100% (1)
- Askep Jiwa Psikososial AnsietasDocument9 pagesAskep Jiwa Psikososial AnsietasDinny ApriliaNo ratings yet
- Protocol MasterDocument12 pagesProtocol MasterEsraa HassanNo ratings yet
- Systematic NewDocument15 pagesSystematic Newshontech proNo ratings yet
- HBMSU Health Conference 2014Document147 pagesHBMSU Health Conference 2014GvsZahidNoorNo ratings yet
- AmericanJournalofMedicalQuality 2015 McGuckin 1062860615611228Document8 pagesAmericanJournalofMedicalQuality 2015 McGuckin 1062860615611228Andy PratamaNo ratings yet
- Technologies As Tools For Quality Management in Health ServicesDocument4 pagesTechnologies As Tools For Quality Management in Health ServicesIJAERS JOURNALNo ratings yet
- Hee Kim, Yeon. Effects of A Work-Based Critical Reflection Program For Novice NursesDocument6 pagesHee Kim, Yeon. Effects of A Work-Based Critical Reflection Program For Novice Nursescantoni1No ratings yet
- 3 Manuscript FinalDocument11 pages3 Manuscript FinalBiomedica INMFRNo ratings yet
- Post Covid StrategyDocument12 pagesPost Covid Strategyadei667062No ratings yet
- Daikin LXE10E-A - Service Manual (TR 01-09B) PDFDocument238 pagesDaikin LXE10E-A - Service Manual (TR 01-09B) PDFmail4ksnNo ratings yet
- Dubai Holding FactsheetDocument2 pagesDubai Holding FactsheetHarley soulNo ratings yet
- International Journal of Agricultural ExtensionDocument6 pagesInternational Journal of Agricultural Extensionacasushi ginzagaNo ratings yet
- Present Simple Present ContinuousDocument3 pagesPresent Simple Present ContinuousFernando SabinoNo ratings yet
- ISO 27001 Gap Analysis ChecklistDocument6 pagesISO 27001 Gap Analysis Checklistlijo jacob70% (10)
- Winsome Hin-Shin LEE CV (Feb 2017)Document5 pagesWinsome Hin-Shin LEE CV (Feb 2017)Winsome LeeNo ratings yet
- P16mba7 1Document4 pagesP16mba7 1Vishalatchi MNo ratings yet
- DAC AnalysisDocument19 pagesDAC Analysisమురళీధర్ ఆది ఆంధ్రుడుNo ratings yet
- Solar Water Heater MOU LaodiceaDocument2 pagesSolar Water Heater MOU LaodiceaZeeshan YasinNo ratings yet
- Avanti II 04-05Document137 pagesAvanti II 04-05Donald SimsNo ratings yet
- Ipcrf Core Values 2019 - FinalDocument23 pagesIpcrf Core Values 2019 - FinalFrendelyn p. Gador100% (4)
- EE 720 - HW Set 3 - 1Document2 pagesEE 720 - HW Set 3 - 1Abdullah AL-RazemNo ratings yet
- Stylus - Pro - 4400 201 300 (067 100)Document34 pagesStylus - Pro - 4400 201 300 (067 100)Joso CepuranNo ratings yet
- Uenr0997 12 00 - Manuals Service Modules - Testing & AdjustingDocument90 pagesUenr0997 12 00 - Manuals Service Modules - Testing & Adjustingmostafa aliNo ratings yet
- Purposive Communication NotesDocument33 pagesPurposive Communication NotesAlexis DapitoNo ratings yet
- Extenso MeterDocument8 pagesExtenso MeterVijayanandh Raja100% (1)
- 3393 - Supervision of Concrete Construction Volume 2Document271 pages3393 - Supervision of Concrete Construction Volume 2Oum ChhayNoy100% (11)
- Cibse TM65 (2020)Document67 pagesCibse TM65 (2020)Reli Hano100% (1)
- TA-Modulator EN LowDocument16 pagesTA-Modulator EN Lowkap4enijNo ratings yet
- Spring 2010 MidTerm OPKST CS101 Bc100200572Document6 pagesSpring 2010 MidTerm OPKST CS101 Bc100200572cs619finalproject.comNo ratings yet
- Land SurveyingDocument174 pagesLand SurveyingArifulmakrif Hailee100% (2)
- The Effect of The Gastrocnemius On The Plantar Fascia: Javier Pascual HuertaDocument18 pagesThe Effect of The Gastrocnemius On The Plantar Fascia: Javier Pascual HuertamarcelonorisNo ratings yet
- Checklist For Rebar and Concrete WorkDocument4 pagesChecklist For Rebar and Concrete WorkDwinto RachmadNo ratings yet
- SeptalkanDocument5 pagesSeptalkanReniNo ratings yet
- TGA Interpretation of Data, Sources of ErrorDocument28 pagesTGA Interpretation of Data, Sources of ErrorUsman GhaniNo ratings yet
- Module - 5Document92 pagesModule - 5Anand ANo ratings yet
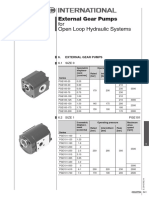
- External Gear Pumps For Open Loop Hydraulic SystemsDocument2 pagesExternal Gear Pumps For Open Loop Hydraulic SystemsBlashko GjorgjievNo ratings yet
- Refinery Workbook ExerciseDocument54 pagesRefinery Workbook ExerciseHarshit SharmaNo ratings yet