You might also like
- Psych 2012123115115620Document6 pagesPsych 2012123115115620Rara QamaraNo ratings yet
- Understanding Generalized Anxiety Disorder and Social Anxiety DisorderDocument8 pagesUnderstanding Generalized Anxiety Disorder and Social Anxiety DisorderabuumaiyoNo ratings yet
- Articol 1 SPVDocument8 pagesArticol 1 SPVStroe EmmaNo ratings yet
- Understanding Depression: Causes, Symptoms, and Treatment OptionsFrom EverandUnderstanding Depression: Causes, Symptoms, and Treatment OptionsNo ratings yet
- Research EssayDocument10 pagesResearch Essayapi-509948413No ratings yet
- Psicology, depression and humor disturbility: Understanding the basic mechanismsFrom EverandPsicology, depression and humor disturbility: Understanding the basic mechanismsNo ratings yet
- Complex PTSD: Understanding PTSD's Effects on Body, Brain and Emotions - Includes Practical Strategies to Heal from TraumaFrom EverandComplex PTSD: Understanding PTSD's Effects on Body, Brain and Emotions - Includes Practical Strategies to Heal from TraumaNo ratings yet
- Psychopharmacology: Borderline Personality DisorderDocument7 pagesPsychopharmacology: Borderline Personality DisorderAwais FaridiNo ratings yet
- Overcoming Depression The Quick Guide to Leaving Depression to Cheerfulness in 2 HoursFrom EverandOvercoming Depression The Quick Guide to Leaving Depression to Cheerfulness in 2 HoursNo ratings yet
- 569927-Diagnostic Skill ApplicationDocument12 pages569927-Diagnostic Skill ApplicationMercyNo ratings yet
- Post-Traumatic Stress Disorder: A Guide for Primary Care Clinicians and TherapistsFrom EverandPost-Traumatic Stress Disorder: A Guide for Primary Care Clinicians and TherapistsNo ratings yet
- EMDR in The Treatment of BPD Literature ReviewDocument13 pagesEMDR in The Treatment of BPD Literature ReviewSidney OxboroughNo ratings yet
- Essay 3 Final RevisedDocument8 pagesEssay 3 Final Revisedapi-643399894No ratings yet
- Gale Researcher Guide for: Depressive Disorders and Their TreatmentFrom EverandGale Researcher Guide for: Depressive Disorders and Their TreatmentNo ratings yet
- Fear and Sadness TMA 1Document3 pagesFear and Sadness TMA 1Shameem DesaiNo ratings yet
- Research Paper On Post Traumatic Stress DisorderDocument8 pagesResearch Paper On Post Traumatic Stress Disorderegvhzwcd100% (1)
- Understanding Anxiety: A Guide for Patients, Family, and FriendsFrom EverandUnderstanding Anxiety: A Guide for Patients, Family, and FriendsNo ratings yet
- Antidepressants in Bipolar Depression An Enduring ControversyDocument6 pagesAntidepressants in Bipolar Depression An Enduring ControversyIzzyinOzzieNo ratings yet
- Trauma Reactivation Under The InfluenceDocument9 pagesTrauma Reactivation Under The InfluenceHypnotica FranceNo ratings yet
- The Mental Mirror: Reflections on Psychiatry: Beyond the Looking Glass: The Enigmatic Odyssey of the MindFrom EverandThe Mental Mirror: Reflections on Psychiatry: Beyond the Looking Glass: The Enigmatic Odyssey of the MindNo ratings yet
- Psychedelics PaperDocument7 pagesPsychedelics PaperJanne AerdtsNo ratings yet
- Mindfulness-Based Treatment For Bipolar Disorder: A Systematic Review of The LiteratureDocument27 pagesMindfulness-Based Treatment For Bipolar Disorder: A Systematic Review of The LiteratureFilza RamdhaniNo ratings yet
- PSY403 - Ivon Sagita - 1Document8 pagesPSY403 - Ivon Sagita - 1Muhammad Isnaeni Rizqi WijayaNo ratings yet
- How Do Mindfulness-Based Programmes Improve Anxiety, Depression and Psychological Distress? A Systematic ReviewDocument23 pagesHow Do Mindfulness-Based Programmes Improve Anxiety, Depression and Psychological Distress? A Systematic ReviewHoang AnhNo ratings yet
- Fuel Minds: Unleash Your Potential with Mind and Body WellnessFrom EverandFuel Minds: Unleash Your Potential with Mind and Body WellnessNo ratings yet
- Systemic Couple Therapy and DepressionDocument3 pagesSystemic Couple Therapy and DepressionAna MoraisNo ratings yet
- PTSD Symptoms and DiagnosisDocument5 pagesPTSD Symptoms and DiagnosisAndrew GrimesNo ratings yet
- The Efficacy of Lysergic Acid Diethylamide For Psychological Assisted Therapy: Systematic Review and Metaanalysis of Randomized Controlled TrialsDocument10 pagesThe Efficacy of Lysergic Acid Diethylamide For Psychological Assisted Therapy: Systematic Review and Metaanalysis of Randomized Controlled TrialsIJAR JOURNALNo ratings yet
- Format. Hum - Managing Psychological Distress With Situational Humour in Young AdultsDocument19 pagesFormat. Hum - Managing Psychological Distress With Situational Humour in Young AdultsImpact JournalsNo ratings yet
- Howard 1Document6 pagesHoward 1api-509696528No ratings yet
- The MindBody Workbook: a thirty day program of insight/ awareness for backpain and other disordersFrom EverandThe MindBody Workbook: a thirty day program of insight/ awareness for backpain and other disordersRating: 5 out of 5 stars5/5 (4)
- DBT Vs CBT On Emotion Regulation and Minfduness in Patients With Generalized Anxiety DisorderDocument8 pagesDBT Vs CBT On Emotion Regulation and Minfduness in Patients With Generalized Anxiety DisorderRAQUEL MENDOZA LOPEZNo ratings yet
- 1 s2.0 S0887618522000330 MainDocument7 pages1 s2.0 S0887618522000330 MainNinoska Benites RamosNo ratings yet
- Alexander H. Jordan2014Document8 pagesAlexander H. Jordan2014Alexandra OanaNo ratings yet
- Depresie Reglarea Emotiilor 2Document20 pagesDepresie Reglarea Emotiilor 2Mălina CorlătianuNo ratings yet
- An Integrative Paradigm for Mental Health Care: Ideas and Methods Shaping the FutureFrom EverandAn Integrative Paradigm for Mental Health Care: Ideas and Methods Shaping the FutureNo ratings yet
- BulimiaDocument20 pagesBulimiaLauraLoaizaNo ratings yet
- BackgroundDocument2 pagesBackgroundGiovanni Carlo LuacanNo ratings yet
- Gale Researcher Guide for: Overview of Behavioral and Mental Disorders in PsychologyFrom EverandGale Researcher Guide for: Overview of Behavioral and Mental Disorders in PsychologyNo ratings yet
- Learning Journal Week 2Document3 pagesLearning Journal Week 2lesleyNo ratings yet
- Running Head: Impact of Ethnicity On Antidepressant Therapy 1Document4 pagesRunning Head: Impact of Ethnicity On Antidepressant Therapy 1Annah AnnNo ratings yet
- Jordan & Litz - Prolonged Grief DisorderDocument8 pagesJordan & Litz - Prolonged Grief Disorderaripla100% (1)
- Discover Effective Strategies to Eliminate Stress and Depression: Your Ultimate Guide to Overcoming Mental Health ChallengesFrom EverandDiscover Effective Strategies to Eliminate Stress and Depression: Your Ultimate Guide to Overcoming Mental Health ChallengesNo ratings yet
- UntitledDocument4 pagesUntitledClinton MandelaNo ratings yet
- Discussion 6.1: Transitioning Into The APRN RoleDocument3 pagesDiscussion 6.1: Transitioning Into The APRN RoleClinton MandelaNo ratings yet
- UntitledDocument4 pagesUntitledClinton MandelaNo ratings yet
- UntitledDocument4 pagesUntitledClinton MandelaNo ratings yet
- Discussion 9.1 - Psychosomatic Disorders in MediaDocument4 pagesDiscussion 9.1 - Psychosomatic Disorders in MediaClinton MandelaNo ratings yet
- Tibia and Fibula Fracture PhysiotherapyDocument31 pagesTibia and Fibula Fracture Physiotherapyunknown unknown100% (1)
- List of Allianz Efu Network (Panel) Hospitals: Hospital Name Address Telephone # KarachiDocument6 pagesList of Allianz Efu Network (Panel) Hospitals: Hospital Name Address Telephone # KarachiFaizan BasitNo ratings yet
- SBFP Form 1 2021 Cebu Province Tubod Elementary SchoolDocument23 pagesSBFP Form 1 2021 Cebu Province Tubod Elementary SchoolJane Rodriguez LumacangNo ratings yet
- Ey Work SampleDocument10 pagesEy Work SampleKris ANo ratings yet
- Use Bloom's Taxonomy to Achieve Learning GoalsDocument61 pagesUse Bloom's Taxonomy to Achieve Learning GoalsSouvik DasNo ratings yet
- Stiletto - Spring 2015Document24 pagesStiletto - Spring 2015TGI Justice ProjectNo ratings yet
- ACUTE KIDNEY INJURY SIGNS, SYMPTOMS, AND CAUSESDocument10 pagesACUTE KIDNEY INJURY SIGNS, SYMPTOMS, AND CAUSESYanti TandjungNo ratings yet
- Lesson 1:: Introduction To Science, Technology and SocietyDocument17 pagesLesson 1:: Introduction To Science, Technology and SocietyAlexis A. AguilarNo ratings yet
- Meaning and Definition of Management DevelopmentDocument7 pagesMeaning and Definition of Management DevelopmentRiteshTirkey100% (2)
- Physical Education and Health 2 - Grade 11 NotesDocument6 pagesPhysical Education and Health 2 - Grade 11 NotesPedro HampaslupaNo ratings yet
- Runner Ru4rxDocument45 pagesRunner Ru4rxfcdypmsbssNo ratings yet
- Immediate Dentures ExplainedDocument64 pagesImmediate Dentures ExplainedDHANASRI MOTAPARTHYNo ratings yet
- Effects of A Capacitive-Resistive Electric Transfer Therapy OnDocument8 pagesEffects of A Capacitive-Resistive Electric Transfer Therapy OnAnna Lygia LunardiNo ratings yet
- Traits of A Healthy Nuclear Safety Culture INPO 12 012 AddendumII Rev.1 A pr2013 PDFDocument70 pagesTraits of A Healthy Nuclear Safety Culture INPO 12 012 AddendumII Rev.1 A pr2013 PDFFirman BhaktiwinayaNo ratings yet
- Obstetric Emergency and Anesthetic ManagementDocument11 pagesObstetric Emergency and Anesthetic ManagementmichaelNo ratings yet
- Hospital departments, medical terms, and anatomyDocument18 pagesHospital departments, medical terms, and anatomyThanh ToànNo ratings yet
- Essential Attitudes, Personal Qualities, and Professional Behaviors Required in NursingDocument27 pagesEssential Attitudes, Personal Qualities, and Professional Behaviors Required in NursingshirleyNo ratings yet
- Bionic Final PDFDocument4 pagesBionic Final PDFJasmine RaoNo ratings yet
- Madre de Cacao With Lemon Scent As Hand Sanitizer: By: Johnro P. LustadoDocument20 pagesMadre de Cacao With Lemon Scent As Hand Sanitizer: By: Johnro P. LustadoJamailla MelendrezNo ratings yet
- MAPEH 7 Weekly Home Learning Plan 2nd QuarterDocument13 pagesMAPEH 7 Weekly Home Learning Plan 2nd QuarterAngelica SantomeNo ratings yet
- Community Engagement, Solidarity and Citizenship: Module 5 - Quarter 1Document28 pagesCommunity Engagement, Solidarity and Citizenship: Module 5 - Quarter 1Benjamin Fernandez Jr.67% (3)
- Zimmer Cemented CPTDocument20 pagesZimmer Cemented CPTJayjeet BhoiteNo ratings yet
- Misrak FeyissaDocument41 pagesMisrak FeyissaN SNo ratings yet
- A Detailed Lesson Plan in TeachingDocument9 pagesA Detailed Lesson Plan in TeachingTetchie GonzalesNo ratings yet
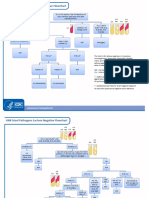
- GNR Stool Pathogens Lactose Negative FlowchartDocument2 pagesGNR Stool Pathogens Lactose Negative FlowchartKeithNo ratings yet
- Strengthening Mental Health and Psychosocial Support Systems and ServicesDocument116 pagesStrengthening Mental Health and Psychosocial Support Systems and ServicesPan PanNo ratings yet
- TOS g78 Crop ProductionDocument1 pageTOS g78 Crop ProductionRommel Lim BasalloteNo ratings yet
- Filipino Help Seeking For Mental Health Problems and Associated Barriers and Facilitators: A Systematic ReviewDocument17 pagesFilipino Help Seeking For Mental Health Problems and Associated Barriers and Facilitators: A Systematic ReviewYuvenn YV Cajilig CanutoNo ratings yet
- Vague X The Skateboard Physiotherapist - Isolation GuideDocument12 pagesVague X The Skateboard Physiotherapist - Isolation GuideKiko Lorman AlvarezNo ratings yet
- Nursing Care of The Older Adult in Wellness: Geriatric Nursing AssessmentDocument36 pagesNursing Care of The Older Adult in Wellness: Geriatric Nursing AssessmentRuby Corazon Ediza100% (6)