You might also like
- Benign Prostatic HyperplasiaDocument6 pagesBenign Prostatic HyperplasiaAnonymous 9OkFvNzdsNo ratings yet
- Oju 2018042516183181Document10 pagesOju 2018042516183181ArsyaFirdausNo ratings yet
- Surgical Treatment of BPH: Technique and ResultsDocument9 pagesSurgical Treatment of BPH: Technique and ResultsAdi WijayantoNo ratings yet
- 0671Document5 pages0671prashanthNo ratings yet
- Jurnal Urologi 234Document8 pagesJurnal Urologi 234Muhammad Rezi RamdanniNo ratings yet
- An Update On Transurethral Surgery For Benign Prostatic ObstructionDocument4 pagesAn Update On Transurethral Surgery For Benign Prostatic ObstructionprashanthNo ratings yet
- Journal ReadingDocument7 pagesJournal ReadingcharissabibilNo ratings yet
- BPH-Diagnosis and TreatmentDocument7 pagesBPH-Diagnosis and TreatmentMedissa MothNo ratings yet
- Intravesical Prostate ProtrusionDocument9 pagesIntravesical Prostate ProtrusionFelly FelixNo ratings yet
- KTP Laser vs Electroresection for BPHDocument5 pagesKTP Laser vs Electroresection for BPHcatur juliartiniNo ratings yet
- BPH 6Document9 pagesBPH 6nong danceNo ratings yet
- Arc BPH Chapter1Document8 pagesArc BPH Chapter1Civa NuhaNo ratings yet
- Bipolar Versus Monopolar Resection of Benign Prostate Hyperplasia: A Comparison of Plasma Electrolytes, Hemoglobin and TUR SyndromeDocument7 pagesBipolar Versus Monopolar Resection of Benign Prostate Hyperplasia: A Comparison of Plasma Electrolytes, Hemoglobin and TUR Syndromefabian arassiNo ratings yet
- BPH Guideline 2019Document10 pagesBPH Guideline 2019Nun AdeninNo ratings yet
- CombatDocument9 pagesCombatMIHAELANo ratings yet
- Comparison of Bipolar and Monopolar Cautry Use in Turp For Treatment of Enlarged ProstateDocument4 pagesComparison of Bipolar and Monopolar Cautry Use in Turp For Treatment of Enlarged ProstatebreadfanNo ratings yet
- PEER Stage2 10.1038 Pcan.2011.13 PDFDocument22 pagesPEER Stage2 10.1038 Pcan.2011.13 PDFMIHAELANo ratings yet
- Benign Prostatic Hypertrophy Comprehensive Management Guide 2Document9 pagesBenign Prostatic Hypertrophy Comprehensive Management Guide 2Thanakorn WongsombutNo ratings yet
- PaeDocument10 pagesPaeMr. LNo ratings yet
- 1Document10 pages1Ade Triansyah EmsilNo ratings yet
- Medical Therapy For Benign Prostatic Hyperplasia: A ReviewDocument11 pagesMedical Therapy For Benign Prostatic Hyperplasia: A ReviewEfson Sustera IrawanNo ratings yet
- 2920-Article Text-12062-3-10-20211018Document4 pages2920-Article Text-12062-3-10-20211018Jenny LauvitaNo ratings yet
- Turp Rtup Tecnica UrologiaDocument6 pagesTurp Rtup Tecnica UrologiaImmer Noyola AvilaNo ratings yet
- The Current RoleDocument11 pagesThe Current RoleDian Permata PutraNo ratings yet
- Carmignani Et Al. - 2013 - A Prospective Evaluation of 200 Patients Undergoing ThuLEP at Our InstitutionDocument2 pagesCarmignani Et Al. - 2013 - A Prospective Evaluation of 200 Patients Undergoing ThuLEP at Our InstitutionNicolas FarkasNo ratings yet
- A2 (Comparison of Prostatic Artery Embolisation (PAE) Versus Transurethral Resection of The Prostate (TURP) For Benign Prostatic Hyperplasia Randomised, Open Label, Non-Inferiority Trial)Document10 pagesA2 (Comparison of Prostatic Artery Embolisation (PAE) Versus Transurethral Resection of The Prostate (TURP) For Benign Prostatic Hyperplasia Randomised, Open Label, Non-Inferiority Trial)NadanNadhifahNo ratings yet
- Faris Akbar Ashari 30101407181Document25 pagesFaris Akbar Ashari 30101407181Fariseilaa PurakbarNo ratings yet
- The TUNA Procedure For BPHDocument5 pagesThe TUNA Procedure For BPHMedissa MothNo ratings yet
- Jurnal ForensikDocument10 pagesJurnal ForensikAlexandria Firdaus Al-farisyNo ratings yet
- Mcvary 2011 Update On AUA Guideline BPHDocument11 pagesMcvary 2011 Update On AUA Guideline BPHFoxglove83No ratings yet
- Transurethral Resection of The Prostate: Urologic SurgeryDocument4 pagesTransurethral Resection of The Prostate: Urologic SurgeryCarolina SidabutarNo ratings yet
- Theimpactofprostatesizemedianlobeandpriorbenignprostatichyperplasiainterventiononrobot Assistedlaparoscopicprostatectomy TechniqueandoutcomesDocument9 pagesTheimpactofprostatesizemedianlobeandpriorbenignprostatichyperplasiainterventiononrobot Assistedlaparoscopicprostatectomy TechniqueandoutcomesGordana PuzovicNo ratings yet
- Interstitial Laser Photocoagulation For Treatment of Benign Prostatic Hypertrophy: Outcomes and Cost EffectivenessDocument8 pagesInterstitial Laser Photocoagulation For Treatment of Benign Prostatic Hypertrophy: Outcomes and Cost Effectivenessmutya yulindaNo ratings yet
- 1 s2.0 S2590280622000079 MainDocument10 pages1 s2.0 S2590280622000079 MainDimas Bintoro KyhNo ratings yet
- Management of AROUDocument6 pagesManagement of AROUAung Ko HtetNo ratings yet
- Application of Embolization Microspheres in Interventional Therapy of Malignant Non-Hypervascular Tumor of Liver (Niu - 2017)Document7 pagesApplication of Embolization Microspheres in Interventional Therapy of Malignant Non-Hypervascular Tumor of Liver (Niu - 2017)Julio OrtegaNo ratings yet
- Tuna Vs TurpDocument5 pagesTuna Vs TurpDimas Aditya Wahyu PamujiNo ratings yet
- Role of TIPS in Managing Liver Transplant CandidatesDocument8 pagesRole of TIPS in Managing Liver Transplant CandidatesgigibesiNo ratings yet
- Is Early Surgical Treatment For Benign Prostatic Hyperplasia Preferable Medical Therapy - Pros and ConsDocument11 pagesIs Early Surgical Treatment For Benign Prostatic Hyperplasia Preferable Medical Therapy - Pros and ConsClaudia FreyonaNo ratings yet
- Surgical Management For Upper Urinary Tr20161125 25958 5bbgsr With Cover Page v2Document11 pagesSurgical Management For Upper Urinary Tr20161125 25958 5bbgsr With Cover Page v2Diogo EmanuelNo ratings yet
- Pancreaticoduodenectomy or Whipple Procedure: Overview: by Dr. Sreeremya.S Faculty of BiologyDocument11 pagesPancreaticoduodenectomy or Whipple Procedure: Overview: by Dr. Sreeremya.S Faculty of BiologyKhuvindra Kevin Matai100% (1)
- mkp012Document5 pagesmkp012Aprilia WNo ratings yet
- Class Presentation ON BPH: Presented By: Ruchika Kaushal M.Sc. Nursing 1 YearDocument31 pagesClass Presentation ON BPH: Presented By: Ruchika Kaushal M.Sc. Nursing 1 YearRuchika KaushalNo ratings yet
- Anesthesia For TurpDocument5 pagesAnesthesia For Turptnim.dsNo ratings yet
- Correlation Between Penile Cuff Test and Pressure-Flow Study in Patients Candidates For Trans-Urethral Resection of ProstateDocument6 pagesCorrelation Between Penile Cuff Test and Pressure-Flow Study in Patients Candidates For Trans-Urethral Resection of ProstatemelianyNo ratings yet
- ID Prostatektomi Radikal Morbiditas Dan MorDocument6 pagesID Prostatektomi Radikal Morbiditas Dan MorarikamanjayaNo ratings yet
- HOW DrBarkinDocument6 pagesHOW DrBarkinMaya LarasNo ratings yet
- Tips Vs BrtoDocument11 pagesTips Vs BrtoCsiszár MártonNo ratings yet
- Monopolar Enucleation Vs Transurethral Resection of The ProstateDocument7 pagesMonopolar Enucleation Vs Transurethral Resection of The ProstateAbraham WilliamNo ratings yet
- Prostataarterienembolisation: Indikation, Technik Und Klinische ErgebnisseDocument9 pagesProstataarterienembolisation: Indikation, Technik Und Klinische ErgebnisseEliana Solange FouzNo ratings yet
- wjmh-33-88Document7 pageswjmh-33-88cjmrioNo ratings yet
- Ha SsDocument7 pagesHa SsSowmya ChitraNo ratings yet
- Uti 14 80Document7 pagesUti 14 80patrickNo ratings yet
- Ecografía ProstaticaDocument9 pagesEcografía ProstaticadynachNo ratings yet
- Hepatocellular CADocument6 pagesHepatocellular CAPatrick JohnNo ratings yet
- Ju 0000000000001298Document6 pagesJu 0000000000001298Cirugía Residentes AjuscoNo ratings yet
- BPH DefinitionDocument5 pagesBPH DefinitionMadhu Sudhan PandeyaNo ratings yet
- Benign Prostatic HyperplasiaDocument34 pagesBenign Prostatic Hyperplasiaanwar jabariNo ratings yet
- Rezecția Bipolară - o Tehnică Mereu Actuală: Geavlete B, Geavlete PDocument2 pagesRezecția Bipolară - o Tehnică Mereu Actuală: Geavlete B, Geavlete PAsproiu EricNo ratings yet
- Lower Urinary Tract Symptoms and BPH TreatmentDocument1 pageLower Urinary Tract Symptoms and BPH TreatmentStefan SaerangNo ratings yet
- Nutrients 14 01684Document11 pagesNutrients 14 01684Stefan SaerangNo ratings yet
- Treatment Options for LUTS and BPHDocument1 pageTreatment Options for LUTS and BPHStefan SaerangNo ratings yet
- 9360 - Catatan Coass Orto - 230226 - 201227Document60 pages9360 - Catatan Coass Orto - 230226 - 201227Stefan SaerangNo ratings yet
- Copyright Ucl PDFDocument1 pageCopyright Ucl PDFStefan SaerangNo ratings yet
- Final Clinical Value of Methycobalamin As A Drug For Peripheral Neuropathy TreatmentDocument21 pagesFinal Clinical Value of Methycobalamin As A Drug For Peripheral Neuropathy TreatmentStefan SaerangNo ratings yet
- Contributors Ucl PDFDocument2 pagesContributors Ucl PDFStefan SaerangNo ratings yet
- Index Ucl PDFDocument5 pagesIndex Ucl PDFStefan SaerangNo ratings yet
- KLP - PBL Kedokteran TropisDocument16 pagesKLP - PBL Kedokteran TropisStefan SaerangNo ratings yet
- E-boarding pass for UPG to CGK flightDocument4 pagesE-boarding pass for UPG to CGK flightStefan SaerangNo ratings yet
- Plasmodium. Leishmania, TripanosomaDocument48 pagesPlasmodium. Leishmania, TripanosomaStefan SaerangNo ratings yet
- Jadwal Kuliah Blok Siklus Hidup Semester Akhir 2020 2021Document9 pagesJadwal Kuliah Blok Siklus Hidup Semester Akhir 2020 2021Stefan SaerangNo ratings yet
- CGK UPG: RZN Regular / 20kg Regular EconomyDocument4 pagesCGK UPG: RZN Regular / 20kg Regular EconomyStefan SaerangNo ratings yet
- Homocystein and NeuropathyDocument25 pagesHomocystein and NeuropathyhanartoajiNo ratings yet
- Haemoflagellates: Leishmaniasis, Trypanosomiasis & MoreDocument69 pagesHaemoflagellates: Leishmaniasis, Trypanosomiasis & Moreheni arisNo ratings yet
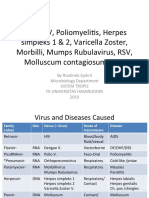
- DHF, HIV, Poliomyeli/s, Herpes Simpleks 1 & 2, Varicella Zoster, Morbilli, Mumps Rubulavirus, RSV, Molluscum Contagiosum, HPVDocument153 pagesDHF, HIV, Poliomyeli/s, Herpes Simpleks 1 & 2, Varicella Zoster, Morbilli, Mumps Rubulavirus, RSV, Molluscum Contagiosum, HPVStefan SaerangNo ratings yet
- 7E. Rabies (Prof Dr. Mochammad Hatta PH.D, SP - MK (K)Document11 pages7E. Rabies (Prof Dr. Mochammad Hatta PH.D, SP - MK (K)Stefan SaerangNo ratings yet
- Botulisme: DR Satriawan Abadi SP - PD KicDocument17 pagesBotulisme: DR Satriawan Abadi SP - PD KicStefan SaerangNo ratings yet
- TestDocument1 pageTestStefan SaerangNo ratings yet
- 7A. Leptospira (Prof Dr. Mochammad Hatta PH.D, SP - MK (K)Document20 pages7A. Leptospira (Prof Dr. Mochammad Hatta PH.D, SP - MK (K)Stefan SaerangNo ratings yet
- DEPKES RI NEW Pedoman Nasional Penanggulangan TBC 2011Document110 pagesDEPKES RI NEW Pedoman Nasional Penanggulangan TBC 2011familyman8091% (11)
- DEPKES RI NEW Pedoman Nasional Penanggulangan TBC 2011Document110 pagesDEPKES RI NEW Pedoman Nasional Penanggulangan TBC 2011familyman8091% (11)
- Engineering Mathematics For Gate Chapter1Document1 pageEngineering Mathematics For Gate Chapter1Sai VeerendraNo ratings yet
- SI 410 Weighing Indicator User ManualDocument64 pagesSI 410 Weighing Indicator User ManualShehab100% (2)
- Honeywell TH6210U2001 Install InstructionsDocument44 pagesHoneywell TH6210U2001 Install Instructionsdarwin jose palacioNo ratings yet
- Meng 2nd Year Death Anniversary MassDocument6 pagesMeng 2nd Year Death Anniversary Massjoy in the spirit of the lordNo ratings yet
- Deltopectoral Approach to the ShoulderDocument28 pagesDeltopectoral Approach to the ShoulderChrysi TsiouriNo ratings yet
- Viral Skin Infections Caused by Herpesviridae and PoxviridaeDocument55 pagesViral Skin Infections Caused by Herpesviridae and PoxviridaeGita RizkiNo ratings yet
- Water Cycle Cer 002Document2 pagesWater Cycle Cer 002api-434008934No ratings yet
- Wood Turning NotesDocument36 pagesWood Turning Notestheodrosyo0% (1)
- 2) Inequality GraphsDocument14 pages2) Inequality Graphsmanobilli30No ratings yet
- DAPUS TINPUS - WPS OfficeDocument3 pagesDAPUS TINPUS - WPS OfficeSilvana NurulfauziyyahNo ratings yet
- Ch.2 Case and Duct SystemDocument11 pagesCh.2 Case and Duct Systemcpt.ghostNo ratings yet
- Despiece Motor Mono PDFDocument55 pagesDespiece Motor Mono PDFGabriel OyagaNo ratings yet
- Treatment of Acid-Related Disorders - SeminarDocument40 pagesTreatment of Acid-Related Disorders - SeminarZana Mohammed0% (1)
- 18.national Forestry Act 1984Document92 pages18.national Forestry Act 1984Sudhir A K KumarenNo ratings yet
- Fault Codes: Brake (DSC/DXC (Dynamic Stability Control) - Bosch 8.0 - Tyre Pressure Monitoring)Document5 pagesFault Codes: Brake (DSC/DXC (Dynamic Stability Control) - Bosch 8.0 - Tyre Pressure Monitoring)zacarias NiquiceNo ratings yet
- Company ProfileDocument10 pagesCompany Profile1anupma0No ratings yet
- Banaba Tea Aids Weight LossDocument5 pagesBanaba Tea Aids Weight LossAveriAlonzoNo ratings yet
- Agile Final Exam - Answer TranscriptDocument12 pagesAgile Final Exam - Answer TranscriptMehwish GauriNo ratings yet
- Overview of Metal Forming ProcessesDocument19 pagesOverview of Metal Forming ProcessesAnonymous 7yN43wjlNo ratings yet
- Tle 9 DLL Q3 W1 1Document3 pagesTle 9 DLL Q3 W1 1Joanne GodezanoNo ratings yet
- Cascade Control: 25.1 Master and Slave LoopsDocument10 pagesCascade Control: 25.1 Master and Slave Loopsdeepak pandeyNo ratings yet
- Polish Words Minimum To Learn DictionaryDocument69 pagesPolish Words Minimum To Learn DictionaryAndras KondratNo ratings yet
- HeavyMetalLimits For Leachability PROP 65 PB and CDDocument3 pagesHeavyMetalLimits For Leachability PROP 65 PB and CDspades24kNo ratings yet
- Aryatech Brochure IndiaDocument12 pagesAryatech Brochure IndiaHari RamNo ratings yet
- DR 38312-011Document33 pagesDR 38312-011Julio Csar da SilvaNo ratings yet
- Predicting Iron Losses in Soft Magnetic Materials With Arbitrary Voltage Supply An Engineering ApproachDocument9 pagesPredicting Iron Losses in Soft Magnetic Materials With Arbitrary Voltage Supply An Engineering Approachmayur isameNo ratings yet
- SR-21 SniperDocument6 pagesSR-21 SniperBaba HeadquaterNo ratings yet
- Vasco Da GamaDocument17 pagesVasco Da GamaxxrawkneeNo ratings yet
- Comprehension Y9aDocument9 pagesComprehension Y9angwenping5No ratings yet
- Suvarnaprashan Sanskar EnglishDocument4 pagesSuvarnaprashan Sanskar EnglishLifecare Ayurveda Drnikul PatelNo ratings yet