You might also like
- Xdue6378 2Document2 pagesXdue6378 2S Abedi50% (2)
- Lab Report 2157646 20210113110650Document3 pagesLab Report 2157646 20210113110650marlon molinaNo ratings yet
- 1 - Japji (Gurmukhi) PDFDocument37 pages1 - Japji (Gurmukhi) PDFsalaharami100% (6)
- Senior's Medical Test ResultsDocument9 pagesSenior's Medical Test Resultssandeep singh cheemaNo ratings yet
- LabReportNewDocument12 pagesLabReportNewoneoceannetwork3No ratings yet
- Mrs. Kirpal Kaur: Test Name Value Unit Bio Ref - IntervalDocument9 pagesMrs. Kirpal Kaur: Test Name Value Unit Bio Ref - IntervalAmanpreet SinghNo ratings yet
- Report - SUMATHI (230380015090)Document5 pagesReport - SUMATHI (230380015090)anumolusumathiNo ratings yet
- File - Report (1665892839610)Document2 pagesFile - Report (1665892839610)Sameer KauraNo ratings yet
- Haematology Test Name Results Biological Reference Interval Units Specimen Test Method CBC - Complete Blood CountDocument8 pagesHaematology Test Name Results Biological Reference Interval Units Specimen Test Method CBC - Complete Blood CountArun DheekshahNo ratings yet
- Report 74a76 1705235769760Document5 pagesReport 74a76 1705235769760aahan2610No ratings yet
- LDSPLDocument8 pagesLDSPLSoham DattaNo ratings yet
- 02 Mar 2021 PDFDocument8 pages02 Mar 2021 PDFVaibhav RamNo ratings yet
- DownloadDocument4 pagesDownloadPradipNo ratings yet
- Lab Report 15034428 20231101060734Document7 pagesLab Report 15034428 20231101060734surangaramesh123No ratings yet
- Mrs Anar DeviDocument14 pagesMrs Anar DeviM.DNo ratings yet
- 0afc33cc Aee6 11ee A7f8 7c1e520e223c HeaderDocument21 pages0afc33cc Aee6 11ee A7f8 7c1e520e223c Headerpparmar871No ratings yet
- ReportDocument19 pagesReportpparmar871No ratings yet
- Pathology 22.04.2020 02.46.58.984Document1 pagePathology 22.04.2020 02.46.58.984Small WondersNo ratings yet
- Lab Report 11867593 20230221104918Document3 pagesLab Report 11867593 20230221104918dineshyadav19900312No ratings yet
- 283185_25262Lab_reportDocument3 pages283185_25262Lab_reportsayand2001No ratings yet
- GOR2208631Document6 pagesGOR2208631SakshiNo ratings yet
- Good Health Package PDFDocument8 pagesGood Health Package PDFRatan Swami SrivastavaNo ratings yet
- Lab Report NewDocument2 pagesLab Report NewCCNo ratings yet
- Report - IRFAN HUSSAIN SYED (230710038227)Document4 pagesReport - IRFAN HUSSAIN SYED (230710038227)cpcxsdqjy9No ratings yet
- Report - LESHAI LAKKAVAJJALA (240700003556)Document4 pagesReport - LESHAI LAKKAVAJJALA (240700003556)Vijay KumarNo ratings yet
- Complete Blood Count: Name DR Chetanbhai MojidaraDocument2 pagesComplete Blood Count: Name DR Chetanbhai Mojidarachetan mojidraNo ratings yet
- 240510002154_Report (1)Document2 pages240510002154_Report (1)darsheel SinghNo ratings yet
- Complete Haemogram (Hemogram & Esr) Haemoglobin Total RBC CountDocument5 pagesComplete Haemogram (Hemogram & Esr) Haemoglobin Total RBC Countrohit bharadwazNo ratings yet
- R8830560 Srijith 151021193600Document7 pagesR8830560 Srijith 151021193600Tyrion LannisterNo ratings yet
- ReportDocument4 pagesReportakash.santhosh22No ratings yet
- Lab Report 16873531 20240314110437Document5 pagesLab Report 16873531 20240314110437tahiraysel23No ratings yet
- Lab Report 11881649 20230221061747Document3 pagesLab Report 11881649 20230221061747azzadari0555No ratings yet
- Lab Report 13747633 20230722013611Document5 pagesLab Report 13747633 20230722013611FazilNo ratings yet
- HeaderDocument4 pagesHeaderatul kumarNo ratings yet
- PET ROMEO-Male05 Years-3749Document1 pagePET ROMEO-Male05 Years-3749rishikeshkallaNo ratings yet
- PHLB1400496733 PDFDocument15 pagesPHLB1400496733 PDFurmobilehacked123No ratings yet
- HeaderDocument13 pagesHeaderKamal KantNo ratings yet
- Mrs. V.dhana LakshmiDocument1 pageMrs. V.dhana LakshmiAnonymous lSZ9JVNo ratings yet
- Complete Blood Count and Biochemistry Panel ResultsDocument8 pagesComplete Blood Count and Biochemistry Panel Resultsgunjan pratapNo ratings yet
- Hematology: KongamdanaDocument1 pageHematology: KongamdanaShariqNo ratings yet
- Hematology: KongamdanaDocument1 pageHematology: KongamdanaShariqNo ratings yet
- MR Santosh Rai: Method: CalculatedDocument10 pagesMR Santosh Rai: Method: CalculatedSantosh RaiNo ratings yet
- Report 220719 195623Document11 pagesReport 220719 195623Abdullah AlviNo ratings yet
- Thyrocare Processed atDocument3 pagesThyrocare Processed atKarim SirNo ratings yet
- Kgmu Trauma 22092200943 7355326825Document2 pagesKgmu Trauma 22092200943 7355326825Ravi KumarNo ratings yet
- 0bf9cc6e-0b76-4a1f-90e3-30efef7d50eaDocument5 pages0bf9cc6e-0b76-4a1f-90e3-30efef7d50eaJay Deep GhoshNo ratings yet
- Chest X-Ray Report for Devansh MehraDocument6 pagesChest X-Ray Report for Devansh MehraShobhitNo ratings yet
- Header-1Document5 pagesHeader-1Sanchit NigamNo ratings yet
- PS325781Document9 pagesPS325781Uchiha ItachiNo ratings yet
- .trashed-1716374771-RHP2308415 (3)Document4 pages.trashed-1716374771-RHP2308415 (3)Anita DwivediNo ratings yet
- Report 1698921174276Document5 pagesReport 1698921174276rajesh.sr92No ratings yet
- Complete Blood Picture (CBP) : Lbnagar - 87Document3 pagesComplete Blood Picture (CBP) : Lbnagar - 87likhith.dsmlNo ratings yet
- Alka Pandey-Female54 Years-53200Document1 pageAlka Pandey-Female54 Years-53200Shantanu PandeyNo ratings yet
- yukti-Female18Document1 pageyukti-Female18officialr66No ratings yet
- Shephali Das-85Document3 pagesShephali Das-85Sanjoy DasNo ratings yet
- Test ReportsDocument4 pagesTest ReportsGreen EWasteNo ratings yet
- Oxy Patho Sample ReportDocument12 pagesOxy Patho Sample ReportWycliffe AnshulNo ratings yet
- Lab Report 15592615 20231208104711Document3 pagesLab Report 15592615 20231208104711gemdos07No ratings yet
- Billwise-Reportstoken eyJhbGciOiJIUzI1NiIsInR5cCI6IkpXVCJ9 eyJwdWJsaWNfa2V5IjoiOGE0MDg0N2QtMTk4MCDocument2 pagesBillwise-Reportstoken eyJhbGciOiJIUzI1NiIsInR5cCI6IkpXVCJ9 eyJwdWJsaWNfa2V5IjoiOGE0MDg0N2QtMTk4MCsaurav dasNo ratings yet
- Download (5)Document3 pagesDownload (5)Rajan MathurNo ratings yet
- CMM hearing details in Gurjit Kaur vs Gurdeep Singh caseDocument1 pageCMM hearing details in Gurjit Kaur vs Gurdeep Singh casesandeep singh cheemaNo ratings yet
- Women in the Military: Arguments For and Against Allowing Women to Join the Armed ForcesDocument5 pagesWomen in the Military: Arguments For and Against Allowing Women to Join the Armed Forcessandeep singh cheemaNo ratings yet
- CRM 9997 2023 24 04 2023 Interim Order PDFDocument1 pageCRM 9997 2023 24 04 2023 Interim Order PDFsandeep singh cheemaNo ratings yet
- Display pdf-2Document1 pageDisplay pdf-2sandeep singh cheemaNo ratings yet
- Cra-S 508 2023 21 02 2023 Interim Order PDFDocument1 pageCra-S 508 2023 21 02 2023 Interim Order PDFsandeep singh cheemaNo ratings yet
- I68033 PDFDocument4 pagesI68033 PDFsandeep singh cheemaNo ratings yet
- Examples 1 PDFDocument4 pagesExamples 1 PDFsandeep singh cheemaNo ratings yet
- KB Ielts AugDocument84 pagesKB Ielts AugRohit patelNo ratings yet
- Nanny 15Document92 pagesNanny 15sandeep singh cheemaNo ratings yet
- Parminder Singh-1 PDFDocument2 pagesParminder Singh-1 PDFsandeep singh cheemaNo ratings yet
- Old Age Booklet RechcedDocument26 pagesOld Age Booklet Rechcedsandeep singh cheemaNo ratings yet
- 1200 Commonly Repeated Spellings or Words in IELTSDocument5 pages1200 Commonly Repeated Spellings or Words in IELTSsandeep singh cheemaNo ratings yet
- VA Ijapsbs Agbogidi 8-29-15 With Cover Page v2Document8 pagesVA Ijapsbs Agbogidi 8-29-15 With Cover Page v2sandeep singh cheemaNo ratings yet
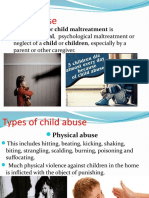
- Child Abuse or Child Maltreatment IsDocument13 pagesChild Abuse or Child Maltreatment Issandeep singh cheemaNo ratings yet
- Comparative Analysis of Therapeutic Benefits of Ocimum: Gratissimum and Vernonia AmygdalinaDocument4 pagesComparative Analysis of Therapeutic Benefits of Ocimum: Gratissimum and Vernonia Amygdalinasandeep singh cheemaNo ratings yet
- SukhmanisahibDocument85 pagesSukhmanisahibvarpalNo ratings yet
- TavprasadsvyeDocument3 pagesTavprasadsvyeAman DsNo ratings yet
- Autobiography of Bhai Sahib Randhir Singh JiDocument255 pagesAutobiography of Bhai Sahib Randhir Singh JiSikh Texts100% (3)
- August-2021-Pdf-Free-Download/: (Updated)Document12 pagesAugust-2021-Pdf-Free-Download/: (Updated)sandeep singh cheemaNo ratings yet
- Old Age Chapter-1,2,3 FullDocument23 pagesOld Age Chapter-1,2,3 Fullsandeep singh cheemaNo ratings yet
- Kirtan Sohila - GurmukhiDocument2 pagesKirtan Sohila - GurmukhiAngela GriffithNo ratings yet
- Anand Sahib 3.2x3.8Document42 pagesAnand Sahib 3.2x3.8Harkirat SinghNo ratings yet
- Jan Lokpal Big OffsetDocument16 pagesJan Lokpal Big OffseteklakshNo ratings yet
- LMCHE102Document45 pagesLMCHE102sandeep singh cheemaNo ratings yet
- Sri Guru Granth Sahib Ji GurmukhiDocument1,490 pagesSri Guru Granth Sahib Ji Gurmukhinss1234567890No ratings yet
- JappsahibDocument18 pagesJappsahibAman DeepNo ratings yet
- Dasam MahantaDocument11 pagesDasam Mahantaਪਰਮਵੀਰ ਸਿੰਘNo ratings yet
- Mastery Test 1Document2 pagesMastery Test 1Garry D. DivinagraciaNo ratings yet
- Chapter 28 - Management of Patients With Coronary Vascular DisordersDocument10 pagesChapter 28 - Management of Patients With Coronary Vascular DisordersMichael BoadoNo ratings yet
- Bapedi Traditional Healers To Treat Erectile DysfunctionDocument9 pagesBapedi Traditional Healers To Treat Erectile DysfunctiontinyikoNo ratings yet
- Uveitis 140205125134 Phpapp02Document139 pagesUveitis 140205125134 Phpapp02ﻣﻠﻚ عيسىNo ratings yet
- COVID19 Vaccination Guidefor Eligible BeneficiariesDocument16 pagesCOVID19 Vaccination Guidefor Eligible BeneficiariesKartik R. MorjariaNo ratings yet
- IELTS Writing Manual Strategies and TechniquesDocument22 pagesIELTS Writing Manual Strategies and TechniquesHeuniceLoisSumabong100% (1)
- Boenninghausen Lesser WDocument323 pagesBoenninghausen Lesser WaldodiasNo ratings yet
- Adventist Youth Honors Answer Book/Health and Science/First Aid, BasicDocument17 pagesAdventist Youth Honors Answer Book/Health and Science/First Aid, BasicrinryNo ratings yet
- Grass Jelly On Glycemic ControlDocument11 pagesGrass Jelly On Glycemic ControlAnanta ArioNo ratings yet
- Community Health Nursing-II DiarrheaDocument4 pagesCommunity Health Nursing-II DiarrheaPriya bhattiNo ratings yet
- Drinking Water Contaminants in PakistanDocument4 pagesDrinking Water Contaminants in PakistanSardar Taimur Hyat-KhanNo ratings yet
- Comprehensive Exam in Nursing Part 1Document36 pagesComprehensive Exam in Nursing Part 1Ariane-Gay Cristobal DuranNo ratings yet
- Children's Cold & Allergy Medicine Uses, Directions and Age GuidelinesDocument4 pagesChildren's Cold & Allergy Medicine Uses, Directions and Age Guidelinesesti saptaNo ratings yet
- Covid 19 Pandemic With KeyDocument2 pagesCovid 19 Pandemic With KeyNan LibraNo ratings yet
- Investigatory Project On MeningitisDocument18 pagesInvestigatory Project On Meningitisno one67% (3)
- Mindmap BedahDocument120 pagesMindmap BedahKavin Maalan SadasseevanNo ratings yet
- Long-Term Effects of Bullying: Dieter Wolke, Suzet Tanya LereyaDocument7 pagesLong-Term Effects of Bullying: Dieter Wolke, Suzet Tanya LereyaEMN PlaylistNo ratings yet
- BNP in CKDDocument6 pagesBNP in CKDDedy ShauqiNo ratings yet
- OsteomyelitisDocument21 pagesOsteomyelitisSurgeonZak0% (1)
- Liver FailureDocument10 pagesLiver FailureLyra LoonNo ratings yet
- Gallbladder Surgery: Common FAQ & Myths - Kaizen Gastro CareDocument2 pagesGallbladder Surgery: Common FAQ & Myths - Kaizen Gastro CareKaizen Gastro CareNo ratings yet
- Nursing Care Plan Otitis MediaDocument3 pagesNursing Care Plan Otitis Mediaevi nur laili100% (2)
- Medicine OSCEDocument21 pagesMedicine OSCEAakash KsNo ratings yet
- Summarizing Key Information from TestsDocument3 pagesSummarizing Key Information from TestsMary Jane SolisNo ratings yet
- Koding BedahDocument2 pagesKoding Bedahabdul halikNo ratings yet
- Free Pharmacology Practice TestDocument3 pagesFree Pharmacology Practice TestDalbir SinghNo ratings yet
- Treating Nose and Throat DisordersDocument7 pagesTreating Nose and Throat DisordersBeda MalecdanNo ratings yet
- Diabetic Foot Care GuideDocument28 pagesDiabetic Foot Care GuidePraneetha NouduriNo ratings yet
- Psychiatric Nursing p.213-231Document20 pagesPsychiatric Nursing p.213-231hurrikhen100% (1)
- Lambert Eaton SyndromeDocument13 pagesLambert Eaton SyndromeOves PatniNo ratings yet