You might also like
- Base Excess, Strong Ion Difference, and Expected Compensations: As Simple As It IsDocument6 pagesBase Excess, Strong Ion Difference, and Expected Compensations: As Simple As It IsDel Rio LauraNo ratings yet
- 02-Siggaard-Andersen Vs Stuart (I Joubert)Document6 pages02-Siggaard-Andersen Vs Stuart (I Joubert)Gin RummyNo ratings yet
- 02-Siggaard-Andersen Vs Stuart (I Joubert)Document6 pages02-Siggaard-Andersen Vs Stuart (I Joubert)gasman2003No ratings yet
- Using Venous Blood Gas Analysis in The Assessment of COPD Exacerbations A Prospective Cohort StudyDocument7 pagesUsing Venous Blood Gas Analysis in The Assessment of COPD Exacerbations A Prospective Cohort Studynur amaliah idrusNo ratings yet
- Arterial Blood Gas Analysis - making it easyFrom EverandArterial Blood Gas Analysis - making it easyRating: 4.5 out of 5 stars4.5/5 (4)
- Acido BaseDocument10 pagesAcido Basebenitez1228No ratings yet
- Captura de Ecrã 2024-02-07 À(s) 19.30.27Document19 pagesCaptura de Ecrã 2024-02-07 À(s) 19.30.27yurgan7No ratings yet
- Respiratory Acid-Base DisordersDocument13 pagesRespiratory Acid-Base DisordersAlfredo PreciadoNo ratings yet
- Ijccm 23 258Document5 pagesIjccm 23 258Aksheth GinnaNo ratings yet
- Correlation of Arterial and Venous Blood Gas ValuesDocument6 pagesCorrelation of Arterial and Venous Blood Gas ValuesandreaNo ratings yet
- Hemodynamic Indices in Pulmonary Hypertension: A Narrative ReviewDocument15 pagesHemodynamic Indices in Pulmonary Hypertension: A Narrative ReviewfabiolaNo ratings yet
- Mergency Medicine, Second Edition: 60 Acid-Base DisordersDocument21 pagesMergency Medicine, Second Edition: 60 Acid-Base DisordersLukman NurfauziNo ratings yet
- Correct Sampling for Blood Gas AnalysisDocument2 pagesCorrect Sampling for Blood Gas AnalysisJavier DeinecaNo ratings yet
- Analysis of Acid-Base Disorders in An ICU Cohort UDocument13 pagesAnalysis of Acid-Base Disorders in An ICU Cohort UJack FruitNo ratings yet
- Blood Gas Analysis For Bedside DiagnosisDocument6 pagesBlood Gas Analysis For Bedside DiagnosisMuhamad Wirawan AdityoNo ratings yet
- Chapter 20Document5 pagesChapter 20Bettina DavenportNo ratings yet
- Exercise HTP ArtDocument10 pagesExercise HTP ArtDiana CarstairsNo ratings yet
- A Study On Serum Sodium and Potassium in Newly Diagnosed Primary HypertensionDocument6 pagesA Study On Serum Sodium and Potassium in Newly Diagnosed Primary HypertensionIJAR JOURNALNo ratings yet
- Acid-Base and Electrolyte Teaching Case Assessing Acid-Base Status: Physiologic Versus Physicochemical ApproachDocument10 pagesAcid-Base and Electrolyte Teaching Case Assessing Acid-Base Status: Physiologic Versus Physicochemical Approachgasman2003No ratings yet
- Superoxide Dismutase As A Protective Factor ForDocument23 pagesSuperoxide Dismutase As A Protective Factor ForUntoro Heri saputroNo ratings yet
- Medicina: Pulmonary Hypertension in COPD: A Case Study and Review of The LiteratureDocument8 pagesMedicina: Pulmonary Hypertension in COPD: A Case Study and Review of The Literatureguhan taraNo ratings yet
- Erp 17 0071Document14 pagesErp 17 0071Jamir PastranaNo ratings yet
- Arterial Blood Gas - Treatment & Management - Point of CareDocument10 pagesArterial Blood Gas - Treatment & Management - Point of CareRo RyNo ratings yet
- Abg Analysis and InterpretationDocument27 pagesAbg Analysis and InterpretationvaishnaviNo ratings yet
- Cerebral Blood Flow and Oxygen DeliDocument12 pagesCerebral Blood Flow and Oxygen DeliMARIA MARCELINA PACHECHO VARGASNo ratings yet
- Study of Serum Electrolytes in Acute Exacerbation of Chronic Obstructive Pulmonary Disease PatientsDocument4 pagesStudy of Serum Electrolytes in Acute Exacerbation of Chronic Obstructive Pulmonary Disease PatientsTri UtomoNo ratings yet
- AGA Venoso Vs ArterialDocument6 pagesAGA Venoso Vs ArterialFulanito CosmeNo ratings yet
- Arterial Blood Gases and KDADocument2 pagesArterial Blood Gases and KDAMarvin Evelio Claros HernandezNo ratings yet
- Art Enfermedad Renal CronicaDocument8 pagesArt Enfermedad Renal CronicaLisset FernandezNo ratings yet
- Gases Arteriales - BE NEJMDocument10 pagesGases Arteriales - BE NEJMalexsr36No ratings yet
- Study of Hemotologicalprofile and Serum Iron Indices in Chronic Kidney Disease in Tertiary Care CentreDocument5 pagesStudy of Hemotologicalprofile and Serum Iron Indices in Chronic Kidney Disease in Tertiary Care CentreIJAR JOURNALNo ratings yet
- Diagnostic Use of Base Excess in Acid-BaseDocument10 pagesDiagnostic Use of Base Excess in Acid-Basejcarl_20063003No ratings yet
- 1302 FullDocument9 pages1302 FullSupicha VichaiditNo ratings yet
- COPD MuscleDocument4 pagesCOPD MuscleJames Cojab SacalNo ratings yet
- HTN CV ComorbiditiesDocument19 pagesHTN CV Comorbiditieslakshminivas PingaliNo ratings yet
- Aquickreferenceon Respiratoryacidosis: Rebecca A. JohnsonDocument5 pagesAquickreferenceon Respiratoryacidosis: Rebecca A. JohnsonJaya Semara PutraNo ratings yet
- Arterial Blood GasesDocument10 pagesArterial Blood GasesSoumya BhattacharyaNo ratings yet
- Abg AnalysisDocument26 pagesAbg Analysissridhar100% (11)
- Ijcm 2014012415343834 PDFDocument5 pagesIjcm 2014012415343834 PDFangela_karenina_1No ratings yet
- Acido Base Critical CareDocument18 pagesAcido Base Critical CareJulia Uchoa UchoaNo ratings yet
- Management of Hypertension in Diabetic Kidney DiseaseDocument12 pagesManagement of Hypertension in Diabetic Kidney DiseasesamuelNo ratings yet
- Cardiopulmo Act 4Document4 pagesCardiopulmo Act 4Zgama AbdulrahmanNo ratings yet
- Acido Base NEJMDocument12 pagesAcido Base NEJMUlises de ÍtacaNo ratings yet
- Postdialysis Hypertension: Associated Factors, Patient Profiles, and Cardiovascular MortalityDocument6 pagesPostdialysis Hypertension: Associated Factors, Patient Profiles, and Cardiovascular MortalityLaura PutriNo ratings yet
- Pathophysiology of COPDDocument4 pagesPathophysiology of COPDrinieeeNo ratings yet
- GLAUKOMA2Document12 pagesGLAUKOMA2NorytaWahyuniawatiAsfianaNo ratings yet
- Abg Analysis NotesDocument32 pagesAbg Analysis Notesakheel ahammedNo ratings yet
- Trastorno Acido BaseDocument15 pagesTrastorno Acido BaseCami Vergara Caro0% (1)
- Revisiting The Role of Oxygen Therapy in Cardiac Patients: Raman Moradkhan, MD, Lawrence I. Sinoway, MDDocument4 pagesRevisiting The Role of Oxygen Therapy in Cardiac Patients: Raman Moradkhan, MD, Lawrence I. Sinoway, MDIda LemonNo ratings yet
- KDIGO Blood Pressure Conference Scope of Work Public ReviewDocument7 pagesKDIGO Blood Pressure Conference Scope of Work Public ReviewYulia SyarifaNo ratings yet
- Nej MR A 1003327Document12 pagesNej MR A 1003327Ivan VazquezNo ratings yet
- 2014 - KenrickDocument12 pages2014 - KenrickCarlNo ratings yet
- 1 s2.0 S1053077023009060 MainDocument31 pages1 s2.0 S1053077023009060 MainedwardmenesesNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 4: VascularFrom EverandComplementary and Alternative Medical Lab Testing Part 4: VascularNo ratings yet
- Plasma Lipids: Optimal Levels for HealthFrom EverandPlasma Lipids: Optimal Levels for HealthAmerican Health FoundationNo ratings yet
- Continuous Renal Replacement Therapy - Who, When, Why and HowDocument37 pagesContinuous Renal Replacement Therapy - Who, When, Why and HowAndrew MihaiNo ratings yet
- Venous OximetryDocument3 pagesVenous OximetryAndrew MihaiNo ratings yet
- Coagulation Support During Perioperative Bleeding ManagementDocument4 pagesCoagulation Support During Perioperative Bleeding ManagementAndrew MihaiNo ratings yet
- Guidelines For The Management of Patients With Severe Acute PancreatitisDocument17 pagesGuidelines For The Management of Patients With Severe Acute PancreatitisJorge Armando Arrieta GalvanNo ratings yet
- Guideline Terbaru ACLFDocument28 pagesGuideline Terbaru ACLFNovita ApramadhaNo ratings yet
- Chem 1018Document4 pagesChem 1018krizelNo ratings yet
- What Is GDH Positive Toxin Negative Clostridium Difficile?: LeafletDocument2 pagesWhat Is GDH Positive Toxin Negative Clostridium Difficile?: LeafletAndrew MihaiNo ratings yet
- STC Bec Wir Plu D 0209 01 PDFDocument10 pagesSTC Bec Wir Plu D 0209 01 PDFAdel MorsyNo ratings yet
- F.E. Campbell - Sweet Slavery - HIT 139Document115 pagesF.E. Campbell - Sweet Slavery - HIT 139HokusLocus67% (3)
- NCM 106 Acute Biologic CrisisDocument142 pagesNCM 106 Acute Biologic CrisisEllamae Chua88% (8)
- Discontinued Tymphany LAT Products LAT500 001 PDFDocument2 pagesDiscontinued Tymphany LAT Products LAT500 001 PDFOgie FermoNo ratings yet
- Tap ChangerDocument5 pagesTap ChangerRavindra AngalNo ratings yet
- E06 Power Cable Joints and Terminations v1Document20 pagesE06 Power Cable Joints and Terminations v1Anorld WalkerNo ratings yet
- Zollinger-Ellison Syndrome (Gastrinoma)Document15 pagesZollinger-Ellison Syndrome (Gastrinoma)Huy QuangNo ratings yet
- Envl 4300 Lab3Document9 pagesEnvl 4300 Lab3api-662867343No ratings yet
- Literature Review On Procrastination Impact On Academic PerformanceDocument2 pagesLiterature Review On Procrastination Impact On Academic Performancemomi100% (1)
- Information Security Management System: Gheorghe MirelaDocument6 pagesInformation Security Management System: Gheorghe MirelaChristen CastilloNo ratings yet
- UM16000 Flame Detector Installation Guide EnglishDocument12 pagesUM16000 Flame Detector Installation Guide Englishmohamed.rescoNo ratings yet
- A 1116Document15 pagesA 1116Rama S. SinghNo ratings yet
- Polythionic Acid Stress Corrosion CrackingDocument2 pagesPolythionic Acid Stress Corrosion CrackingVajid MadathilNo ratings yet
- Ramial Chipped Wood - A Basic Tool For Regenerating SoilsDocument15 pagesRamial Chipped Wood - A Basic Tool For Regenerating SoilsmrmiscNo ratings yet
- 1978 - 90 Day Study or Rhesus Monkey ToxicityDocument4 pages1978 - 90 Day Study or Rhesus Monkey Toxicitygrace poudrierNo ratings yet
- Implementation of Swachh Bharat in MysoreDocument13 pagesImplementation of Swachh Bharat in MysoreDipyaman ChoudhuryNo ratings yet
- Analysis of Drinking Water Quality Parameters (A Case Study of Hanumangarh Town)Document8 pagesAnalysis of Drinking Water Quality Parameters (A Case Study of Hanumangarh Town)Editor IJTSRDNo ratings yet
- Quiz Integumentary SystemDocument23 pagesQuiz Integumentary SystemLemuel CunananNo ratings yet
- PMBOK - Chapter 9: Project Human Resource ManagementDocument16 pagesPMBOK - Chapter 9: Project Human Resource Management7565006No ratings yet
- W H G Kingston "Dick Cheveley": PrefaceDocument159 pagesW H G Kingston "Dick Cheveley": PrefaceGutenberg.orgNo ratings yet
- Pensions Reforms at NSSFDocument4 pagesPensions Reforms at NSSFcliffmogere2348No ratings yet
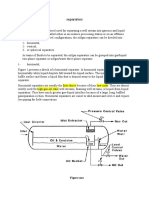
- Separators: Figure OneDocument8 pagesSeparators: Figure OneMohamed Moder100% (1)
- Papers Traducir CompletoDocument12 pagesPapers Traducir CompletoJuan Jesus Barreda TalaveraNo ratings yet
- Celecoxib Identification MethodsDocument5 pagesCelecoxib Identification Methodsabc1679No ratings yet
- Folder Hexa EngDocument8 pagesFolder Hexa EngMuresan MVNo ratings yet
- Pharmaceutical Microbiology - B.pharmDocument383 pagesPharmaceutical Microbiology - B.pharmkeyurNo ratings yet
- How To Judge A Dasha in JyotishDocument2 pagesHow To Judge A Dasha in JyotishRavan SharmaNo ratings yet
- Ats, TT, Tig: Anti Tetanus Serum, Tetanus Toxoid, Tetanus Immuno-GlobulinDocument15 pagesAts, TT, Tig: Anti Tetanus Serum, Tetanus Toxoid, Tetanus Immuno-Globulinjisoo100% (2)
- Perineal Care Procedure GuideDocument2 pagesPerineal Care Procedure GuideAlhadzra AlihNo ratings yet
- Music and Therapy Bun2Document17 pagesMusic and Therapy Bun2PanteaAlisaNo ratings yet