You might also like
- How To Randomise BMJDocument3 pagesHow To Randomise BMJJu ChangNo ratings yet
- New Health Systems: Integrated Care and Health Inequalities ReductionFrom EverandNew Health Systems: Integrated Care and Health Inequalities ReductionNo ratings yet
- Mehu131 - U1 - T4 - Corticoesteroides en Meningitis TuberculosaDocument3 pagesMehu131 - U1 - T4 - Corticoesteroides en Meningitis TuberculosalizdanNo ratings yet
- Articulo HealthDocument9 pagesArticulo HealthAntonio MalacaraNo ratings yet
- Global Health for All: Knowledge, Politics, and PracticesFrom EverandGlobal Health for All: Knowledge, Politics, and PracticesNo ratings yet
- Bryant 2017Document20 pagesBryant 2017Jean M Huaman FiallegaNo ratings yet
- The Opioid Epidemic and the Therapeutic Community Model: An Essential GuideFrom EverandThe Opioid Epidemic and the Therapeutic Community Model: An Essential GuideJonathan D. AveryNo ratings yet
- WHPL Canon Kickbusch 2003 Contribution of The WHO To A New Public Health and Health Promotion Ajph.93.3.383Document6 pagesWHPL Canon Kickbusch 2003 Contribution of The WHO To A New Public Health and Health Promotion Ajph.93.3.383jaswanthlalam2010No ratings yet
- The Contribution of The World Health Organization To A New Public Health and Health PromotionDocument12 pagesThe Contribution of The World Health Organization To A New Public Health and Health PromotionLaura ZahariaNo ratings yet
- The Five Star DoctorDocument3 pagesThe Five Star DoctorTasya Laresa100% (1)
- The Measurement of Health and Health StatusDocument2 pagesThe Measurement of Health and Health StatusKes DimapilisNo ratings yet
- Neogi-2018-Patient Education and Engagement in Treat-To-targetDocument3 pagesNeogi-2018-Patient Education and Engagement in Treat-To-targetNash YoungNo ratings yet
- Health Systems Strengthening, Universal Health Coverage, Health Security and ResilienceDocument1 pageHealth Systems Strengthening, Universal Health Coverage, Health Security and ResilienceCharles ChalimbaNo ratings yet
- Sepulveda 2002 Paliative Care Who PerspectiveDocument6 pagesSepulveda 2002 Paliative Care Who PerspectiveDaniela MunteleNo ratings yet
- Who 2007-2017 PDFDocument152 pagesWho 2007-2017 PDFshindyayu widyaswaraNo ratings yet
- WHO HSE GCR 2015.5 Eng PDFDocument180 pagesWHO HSE GCR 2015.5 Eng PDFFull ColourNo ratings yet
- Reviewed Lecture International Health RMDC 1.18.52 PMDocument36 pagesReviewed Lecture International Health RMDC 1.18.52 PMSyed HussainNo ratings yet
- Comment: For Lancet On Universal Universal-Health-CoverageDocument2 pagesComment: For Lancet On Universal Universal-Health-Coverageapi-112905159No ratings yet
- Introduction: Positioning Universal Health Coverage in The Post-2015 Development AgendaDocument15 pagesIntroduction: Positioning Universal Health Coverage in The Post-2015 Development AgendaJihan SyafitriNo ratings yet
- WHO World ReportDocument204 pagesWHO World ReportAan NurwatiNo ratings yet
- Unit Ii. The Health Care Delivery SystemDocument8 pagesUnit Ii. The Health Care Delivery SystemShane PangilinanNo ratings yet
- Midtest For FKM Class A Read The Text WellDocument3 pagesMidtest For FKM Class A Read The Text WellDarsini Puji LNo ratings yet
- Years of The WHO Essential Medicines Lis20161105-14972-15gvha0-With-Cover-Page-V2Document8 pagesYears of The WHO Essential Medicines Lis20161105-14972-15gvha0-With-Cover-Page-V2Taufi HemyariNo ratings yet
- AFHS Global ConsultationDocument29 pagesAFHS Global Consultationapi-3749052No ratings yet
- Global Health and Nursing Group 2Document16 pagesGlobal Health and Nursing Group 2Kathleen Camile CenaNo ratings yet
- World Health Report 2004Document96 pagesWorld Health Report 2004agniesia_rakNo ratings yet
- How Can The Sustainable Development Goals Improve Global Health? Call For PapersDocument2 pagesHow Can The Sustainable Development Goals Improve Global Health? Call For PapersZelalem TilahunNo ratings yet
- CMH Working Paper SeriesDocument41 pagesCMH Working Paper SeriesPeter M. HeimlichNo ratings yet
- Gs Infant Feeding Text EngDocument36 pagesGs Infant Feeding Text Engreza yunusNo ratings yet
- Healthcare Delivery System Changes in the PhilippinesDocument9 pagesHealthcare Delivery System Changes in the PhilippinesKrystel Anne MilanNo ratings yet
- WO RLD Health Organization HistoryDocument9 pagesWO RLD Health Organization HistoryEmerina SoNo ratings yet
- World Health Report 2008Document148 pagesWorld Health Report 2008dancutrer2100% (2)
- Introduction To Essential DrugsDocument46 pagesIntroduction To Essential DrugsMrym NbNo ratings yet
- Reviewer Ncm104Document18 pagesReviewer Ncm104SONZA JENNEFERNo ratings yet
- The Continuing Evolution of Health Promotion - 2021Document3 pagesThe Continuing Evolution of Health Promotion - 2021nuno ferreiraNo ratings yet
- Community-Based Noncommunicable Disease Interventions: Lessons From Developed Countries For Developing OnesDocument8 pagesCommunity-Based Noncommunicable Disease Interventions: Lessons From Developed Countries For Developing Onessukainah al hadadNo ratings yet
- WHO - The World Health 2000Document215 pagesWHO - The World Health 2000esmoiponja100% (1)
- The World Health Report 2000Document27 pagesThe World Health Report 2000Perpustakaan stikesbpiNo ratings yet
- International HealthDocument110 pagesInternational HealthHiren patelNo ratings yet
- Nations For Mental Health: Final ReportDocument68 pagesNations For Mental Health: Final ReportEnchantia R. NightshadeNo ratings yet
- Key Data and Findings Maternal Health MedicinesDocument37 pagesKey Data and Findings Maternal Health MedicinesKabir AhmedNo ratings yet
- WHO Health Promotion Glossary: New TermsDocument6 pagesWHO Health Promotion Glossary: New TermsBrendan MaloneyNo ratings yet
- COVID-19 MUN Conference MessageDocument21 pagesCOVID-19 MUN Conference MessageAastha AroraNo ratings yet
- Olemberio Lesson Plan4Document5 pagesOlemberio Lesson Plan4Jayvee OlemberioNo ratings yet
- Preventing HIV in Young People: A Systematic Review of The Evidence From Developing CountriesDocument357 pagesPreventing HIV in Young People: A Systematic Review of The Evidence From Developing CountriesCrowdOutAIDSNo ratings yet
- Materi UTS Global HealthDocument141 pagesMateri UTS Global HealthNurul AnggrainiNo ratings yet
- WHO's Role in Combating COVID-19Document28 pagesWHO's Role in Combating COVID-19Priyanshi MehtaNo ratings yet
- Health and The Millennium Development Goals: School of Population HealthDocument15 pagesHealth and The Millennium Development Goals: School of Population HealthAtta BoamahNo ratings yet
- Origins of Primary Health Care and Selective Primary Health CareDocument16 pagesOrigins of Primary Health Care and Selective Primary Health CareMaria MahusayNo ratings yet
- Operationalizing One Health: Developing an Implementation RoadmapDocument24 pagesOperationalizing One Health: Developing an Implementation RoadmapsackNo ratings yet
- Who Global StrategyDocument37 pagesWho Global StrategyAdethya SimatupangNo ratings yet
- MDG Indicators HFS032Document16 pagesMDG Indicators HFS032teguhNo ratings yet
- Mapeh 10Document12 pagesMapeh 10mercadolorence20No ratings yet
- Strengthening health systems for universal health coverage and sustainable developmentDocument3 pagesStrengthening health systems for universal health coverage and sustainable developmentghoudzNo ratings yet
- Koplan2009 - Defincion de Salud GlobalDocument3 pagesKoplan2009 - Defincion de Salud GlobalIsa SuMe01No ratings yet
- UN Report Examines Link Between Nutrition, Diets and NCDsDocument12 pagesUN Report Examines Link Between Nutrition, Diets and NCDsVineet MariyappanNo ratings yet
- Global Health Issues and ConcernsDocument24 pagesGlobal Health Issues and ConcernsMa Eloiza Urbana100% (1)
- Urban Health in Developing CountriesDocument14 pagesUrban Health in Developing Countriesvictoriatatenda06No ratings yet
- 3B User-Manual CPAP-Auto-CPAP RESmart BMC V1.7 ENG-1Document35 pages3B User-Manual CPAP-Auto-CPAP RESmart BMC V1.7 ENG-1Ricardo Costa CaribéNo ratings yet
- Nursing Reflective Practice - An Empirical Literature ReviewDocument10 pagesNursing Reflective Practice - An Empirical Literature ReviewChris LeeNo ratings yet
- Reflections in LearningDocument17 pagesReflections in LearningChris LeeNo ratings yet
- The "Completely Randomised" and The "Randomised Block" Are The Only Experimental Designs Suitable For Widespread Use in Pre Clinical ResearchDocument5 pagesThe "Completely Randomised" and The "Randomised Block" Are The Only Experimental Designs Suitable For Widespread Use in Pre Clinical ResearchChris LeeNo ratings yet
- Reflection in and On Nursing Practices - How NursesDocument7 pagesReflection in and On Nursing Practices - How NursesChris LeeNo ratings yet
- 狗乾糧推薦名單2021Document5 pages狗乾糧推薦名單2021Chris LeeNo ratings yet
- Chemotherapy of Tuberculosis in Hong KongDocument17 pagesChemotherapy of Tuberculosis in Hong KongChris LeeNo ratings yet
- Reflective Learning in Higher Education - A Comparative AnalysisDocument8 pagesReflective Learning in Higher Education - A Comparative AnalysisChris LeeNo ratings yet
- Arterial Blood Gas (ABG) Analysis: Normal ValuesDocument3 pagesArterial Blood Gas (ABG) Analysis: Normal ValuesNayem Hossain HemuNo ratings yet
- Pneumonia, Atelectasis & EffusionsDocument38 pagesPneumonia, Atelectasis & EffusionsChris LeeNo ratings yet
- RESmart - CPAP, Auto - User ManualDocument40 pagesRESmart - CPAP, Auto - User ManualChris LeeNo ratings yet
- Terms of The Creative Commons Attribution Share Alike-3.0 LicenseDocument109 pagesTerms of The Creative Commons Attribution Share Alike-3.0 LicenseChris LeeNo ratings yet
- Adult Cardiac Arrest Circular Algorithm: Monitor CPR QualityDocument1 pageAdult Cardiac Arrest Circular Algorithm: Monitor CPR QualityChris LeeNo ratings yet
- CT Scans of The Head: A Neurologist's PerspectiveDocument111 pagesCT Scans of The Head: A Neurologist's PerspectiveChris LeeNo ratings yet
- 12-Lead Ecgs and Electrical Axis: Fast & Easy Ecgs, 2Nd E - A Self-Paced Learning ProgramDocument66 pages12-Lead Ecgs and Electrical Axis: Fast & Easy Ecgs, 2Nd E - A Self-Paced Learning ProgramlalaNo ratings yet
- Pneumonia, Atelectasis & EffusionsDocument38 pagesPneumonia, Atelectasis & EffusionsChris LeeNo ratings yet
- 12-Lead Ecgs and Electrical Axis: Fast & Easy Ecgs, 2Nd E - A Self-Paced Learning ProgramDocument66 pages12-Lead Ecgs and Electrical Axis: Fast & Easy Ecgs, 2Nd E - A Self-Paced Learning ProgramlalaNo ratings yet
- Cir 0000000000000613 PDFDocument10 pagesCir 0000000000000613 PDFDeivy De Jesus Cordoba SerratoNo ratings yet
- How To Read A Head CTDocument90 pagesHow To Read A Head CTChris LeeNo ratings yet
- Thoracic Radiographic Anatomy: Einav Shochat MS4 Visiting Medical StudentDocument81 pagesThoracic Radiographic Anatomy: Einav Shochat MS4 Visiting Medical StudentChris LeeNo ratings yet
- CT Head and Ischemic Cva: What To Look For On The Early Scan??Document19 pagesCT Head and Ischemic Cva: What To Look For On The Early Scan??Chris LeeNo ratings yet
- Acute Stroke Management Resource:: Types of Stroke & Anatomy and Physiology of Acute StrokeDocument52 pagesAcute Stroke Management Resource:: Types of Stroke & Anatomy and Physiology of Acute StrokeChris LeeNo ratings yet
- CAPD - StaySafe Training Manual PDFDocument16 pagesCAPD - StaySafe Training Manual PDFChris LeeNo ratings yet
- 2 4 Plasma ProductsDocument3 pages2 4 Plasma Productsشريف عبد المنعمNo ratings yet
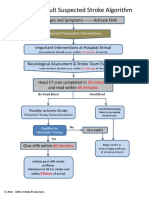
- ACLS Stroke Algorithm PDFDocument1 pageACLS Stroke Algorithm PDFChris LeeNo ratings yet
- Catheter Care Guidelines PDFDocument45 pagesCatheter Care Guidelines PDFJayakumar JNo ratings yet
- Nursing Tools Psychotherapy PDFDocument1 pageNursing Tools Psychotherapy PDFChris LeeNo ratings yet
- Bladder Irrigation CystoclysisDocument4 pagesBladder Irrigation Cystoclysisme meNo ratings yet
- Anorexia PaperDocument6 pagesAnorexia Paperapi-254016016No ratings yet
- Impact of Diabetic Ketoacidosis Management in The Medical Intensive Care Unit After Order Set ImplementationDocument6 pagesImpact of Diabetic Ketoacidosis Management in The Medical Intensive Care Unit After Order Set ImplementationFrancisco Sampedro0% (1)
- Elastic Bandage Applying PDFDocument4 pagesElastic Bandage Applying PDFDaniIrawanNo ratings yet
- Reproduction Pathology ReviewDocument9 pagesReproduction Pathology ReviewkishorechandraNo ratings yet
- BE FAST ED FormDocument1 pageBE FAST ED FormTHARHATA I JUHASANNo ratings yet
- Cebu Activity DesignDocument22 pagesCebu Activity DesignMariefer EsplagoNo ratings yet
- Frequency of Over Eruption in Unopposed Posterior TeethDocument7 pagesFrequency of Over Eruption in Unopposed Posterior TeethDaniel Lévano AlzamoraNo ratings yet
- Feeding Infants and ToddlersDocument6 pagesFeeding Infants and ToddlersNedum WilfredNo ratings yet
- First Aid KitDocument25 pagesFirst Aid Kitgo back to natureNo ratings yet
- Sleep Disorders in The ElderlyDocument50 pagesSleep Disorders in The ElderlykikimarioNo ratings yet
- Vertical Root Fractures in Endodontically Treated Teeth A Clinical SurveyDocument4 pagesVertical Root Fractures in Endodontically Treated Teeth A Clinical SurveyVimi GeorgeNo ratings yet
- ChemDocument15 pagesChemYaghvi VaishnavNo ratings yet
- WWTPD Lab Assign 3Document3 pagesWWTPD Lab Assign 3Zohaib BaigNo ratings yet
- Keep Your Eyes HealthyDocument20 pagesKeep Your Eyes HealthydrjperumalNo ratings yet
- Congestive Heart FailureDocument15 pagesCongestive Heart FailureChiraz Mwangi100% (1)
- FilgrastimDocument3 pagesFilgrastimapi-3797941No ratings yet
- Geriatric Assessment TomtomDocument4 pagesGeriatric Assessment TomtomMark Angelo Soliman AcupidoNo ratings yet
- Medication ErrorsDocument13 pagesMedication Errorsrozsheng100% (1)
- 2.D Ndera CaseDocument9 pages2.D Ndera CaseNsengimana Eric MaxigyNo ratings yet
- Knowledge DeficitDocument2 pagesKnowledge DeficitSahara Sahjz Macabangun67% (3)
- Bio 473 Reproductive Endocrinology Lab Compiled LabDocument10 pagesBio 473 Reproductive Endocrinology Lab Compiled Labapi-253602935No ratings yet
- Color Atlas of Emergency TraumaDocument314 pagesColor Atlas of Emergency TraumaIacob Razvan75% (8)
- Drug Therapy ProblemDocument19 pagesDrug Therapy ProblemAulia NorfiantikaNo ratings yet
- After 2 Hours of Nursing Intervention, The Mother Will Verbalized The Understanding of The Condition, Process, and TreatmentDocument3 pagesAfter 2 Hours of Nursing Intervention, The Mother Will Verbalized The Understanding of The Condition, Process, and TreatmentJelly Yanquiling DumlaoNo ratings yet
- Power Point ClabsiDocument11 pagesPower Point Clabsiapi-290870524No ratings yet
- Varcarolis: Essentials of Psychiatric Mental Health Nursing: Test Bank Chapter 10: Personality Disorders Multiple ChoiceDocument17 pagesVarcarolis: Essentials of Psychiatric Mental Health Nursing: Test Bank Chapter 10: Personality Disorders Multiple Choiceyaneidys perezNo ratings yet
- Addiction Treatment Homework Planner Practiceplanners 5th Edition Ebook PDF VersionDocument62 pagesAddiction Treatment Homework Planner Practiceplanners 5th Edition Ebook PDF Versionjames.keeter43297% (39)
- NRS476.pdf Answer PDFDocument13 pagesNRS476.pdf Answer PDFsyabiellaNo ratings yet
- Social Case Study Report: I. Identifying InformationDocument4 pagesSocial Case Study Report: I. Identifying InformationLeoterio LacapNo ratings yet
- Torts: QuickStudy Laminated Reference GuideFrom EverandTorts: QuickStudy Laminated Reference GuideRating: 5 out of 5 stars5/5 (1)
- The Power of Our Supreme Court: How Supreme Court Cases Shape DemocracyFrom EverandThe Power of Our Supreme Court: How Supreme Court Cases Shape DemocracyRating: 5 out of 5 stars5/5 (2)
- Dictionary of Legal Terms: Definitions and Explanations for Non-LawyersFrom EverandDictionary of Legal Terms: Definitions and Explanations for Non-LawyersRating: 5 out of 5 stars5/5 (2)
- Legal Writing in Plain English, Third Edition: A Text with ExercisesFrom EverandLegal Writing in Plain English, Third Edition: A Text with ExercisesNo ratings yet
- Nolo's Encyclopedia of Everyday Law: Answers to Your Most Frequently Asked Legal QuestionsFrom EverandNolo's Encyclopedia of Everyday Law: Answers to Your Most Frequently Asked Legal QuestionsRating: 4 out of 5 stars4/5 (18)
- Legal Writing in Plain English: A Text with ExercisesFrom EverandLegal Writing in Plain English: A Text with ExercisesRating: 3 out of 5 stars3/5 (2)
- Employment Law: a Quickstudy Digital Law ReferenceFrom EverandEmployment Law: a Quickstudy Digital Law ReferenceRating: 1 out of 5 stars1/5 (1)
- Legal Forms for Starting & Running a Small Business: 65 Essential Agreements, Contracts, Leases & LettersFrom EverandLegal Forms for Starting & Running a Small Business: 65 Essential Agreements, Contracts, Leases & LettersNo ratings yet
- LLC or Corporation?: Choose the Right Form for Your BusinessFrom EverandLLC or Corporation?: Choose the Right Form for Your BusinessRating: 3.5 out of 5 stars3.5/5 (4)
- Nolo's Essential Guide to Buying Your First HomeFrom EverandNolo's Essential Guide to Buying Your First HomeRating: 4 out of 5 stars4/5 (43)
- Everybody's Guide to the Law: All The Legal Information You Need in One Comprehensive VolumeFrom EverandEverybody's Guide to the Law: All The Legal Information You Need in One Comprehensive VolumeNo ratings yet
- Nolo's Deposition Handbook: The Essential Guide for Anyone Facing or Conducting a DepositionFrom EverandNolo's Deposition Handbook: The Essential Guide for Anyone Facing or Conducting a DepositionRating: 5 out of 5 stars5/5 (1)
- A Student's Guide to Law School: What Counts, What Helps, and What MattersFrom EverandA Student's Guide to Law School: What Counts, What Helps, and What MattersRating: 5 out of 5 stars5/5 (4)
- Legal Guide for Starting & Running a Small BusinessFrom EverandLegal Guide for Starting & Running a Small BusinessRating: 4.5 out of 5 stars4.5/5 (9)
- Form Your Own Limited Liability Company: Create An LLC in Any StateFrom EverandForm Your Own Limited Liability Company: Create An LLC in Any StateNo ratings yet
- Essential Guide to Workplace Investigations, The: A Step-By-Step Guide to Handling Employee Complaints & ProblemsFrom EverandEssential Guide to Workplace Investigations, The: A Step-By-Step Guide to Handling Employee Complaints & ProblemsRating: 3 out of 5 stars3/5 (2)
- So You Want to be a Lawyer: The Ultimate Guide to Getting into and Succeeding in Law SchoolFrom EverandSo You Want to be a Lawyer: The Ultimate Guide to Getting into and Succeeding in Law SchoolNo ratings yet
- Nolo's Essential Guide to Child Custody and SupportFrom EverandNolo's Essential Guide to Child Custody and SupportRating: 4 out of 5 stars4/5 (1)