You might also like
- Laws of ThermocoupleDocument3 pagesLaws of ThermocoupleMourougapragash SubramanianNo ratings yet
- Oral Medication PharmacologyDocument4 pagesOral Medication PharmacologyElaisa Mae Delos SantosNo ratings yet
- Case Study Resilience and SpiritualityDocument17 pagesCase Study Resilience and Spiritualityshowerfalls100% (1)
- Mediating Effects Coping Spirituality PsychologicalDistressDocument13 pagesMediating Effects Coping Spirituality PsychologicalDistressGina SmithNo ratings yet
- 2016 Agli Frecnh PDFDocument13 pages2016 Agli Frecnh PDFnermal93No ratings yet
- Psy Research Proposal - Religiosty and DepressionDocument15 pagesPsy Research Proposal - Religiosty and DepressionHadi RazaNo ratings yet
- 2015 Raffertyetal Rscomm journalRHDocument19 pages2015 Raffertyetal Rscomm journalRHCristiana CarvalhoNo ratings yet
- Spiritual Well-Being and Lifestyle Choices in Adolescents: A Quantitative Study Among Afrikaans-Speaking Learners in The North West Province of South AfricaDocument11 pagesSpiritual Well-Being and Lifestyle Choices in Adolescents: A Quantitative Study Among Afrikaans-Speaking Learners in The North West Province of South Africahendra pranataNo ratings yet
- Research Paper On DepressionDocument8 pagesResearch Paper On Depressionfveec9sx100% (1)
- Religion Spirituality and Gender-Diferentiated Trajectories - kent 2019Document18 pagesReligion Spirituality and Gender-Diferentiated Trajectories - kent 2019Mércia FiuzaNo ratings yet
- JurnalDocument21 pagesJurnalyesi martinaNo ratings yet
- Schreiber 2011Document13 pagesSchreiber 2011Angelia Adinda AnggonoNo ratings yet
- Spiritual and Religious Beliefs As Risk Factors For The Onset of Major DepressionDocument13 pagesSpiritual and Religious Beliefs As Risk Factors For The Onset of Major DepressionAlee VerdinNo ratings yet
- Ni Hms 101891 Bienestar y DepresiónDocument12 pagesNi Hms 101891 Bienestar y DepresiónKaren MendozaNo ratings yet
- Do Spirituality HelpDocument16 pagesDo Spirituality HelpChe'gu JamalNo ratings yet
- 2011 - Linden - Attitudes of Qualified Vs Student Mental Health Nurses Towards An IndividualDocument10 pages2011 - Linden - Attitudes of Qualified Vs Student Mental Health Nurses Towards An IndividualRonii SzékelyNo ratings yet
- Saleem and Saleem - 2017 - Role of Religiosity in Psychological Well-Being AmDocument12 pagesSaleem and Saleem - 2017 - Role of Religiosity in Psychological Well-Being AmAMIT KUMAR DWIVEDINo ratings yet
- An Exploration of Health and Religion in Elderly People Through The Lens of Scriptural ReminiscenceDocument14 pagesAn Exploration of Health and Religion in Elderly People Through The Lens of Scriptural Reminiscencegiseladelarosa2006No ratings yet
- A Study of Religiosity in Relation To Spirituality and AnxietyDocument17 pagesA Study of Religiosity in Relation To Spirituality and AnxietyRavi KumarNo ratings yet
- Fukui2012 Article SpiritualWell-BeingOfPeopleWitDocument10 pagesFukui2012 Article SpiritualWell-BeingOfPeopleWitVerinha CarvNo ratings yet
- The Relationship Between Religiosity and Anxiety PDFDocument11 pagesThe Relationship Between Religiosity and Anxiety PDFAini Nayara PutriNo ratings yet
- Role of Religiosity and Psychological Well BeingDocument11 pagesRole of Religiosity and Psychological Well BeingCynthia Torres-GonzálezNo ratings yet
- Powell, Religion, Spirituality, Health, AmPsy, 2003Document17 pagesPowell, Religion, Spirituality, Health, AmPsy, 2003Muresanu Teodora IlincaNo ratings yet
- (Series in Positive Psychology.) Pluess, Michael - Genetics of Psychological Well-Being - The Role of Heritability and Genetics in Positive Psychology-Oxford UniveDocument317 pages(Series in Positive Psychology.) Pluess, Michael - Genetics of Psychological Well-Being - The Role of Heritability and Genetics in Positive Psychology-Oxford UniveLaura Quintero100% (1)
- HHS Public Access: Incorporating Spirituality in Primary CareDocument14 pagesHHS Public Access: Incorporating Spirituality in Primary CareTibor GalacziNo ratings yet
- How spirituality and resilience impact mental healthDocument16 pagesHow spirituality and resilience impact mental healthDimas NugrohoNo ratings yet
- Self-Stigma Experiences Among Older Adults With MeDocument10 pagesSelf-Stigma Experiences Among Older Adults With MeKlinik KitamuraNo ratings yet
- Psychosocial Health'Document8 pagesPsychosocial Health'hadiNo ratings yet
- Measuring Differentiation SelfDocument9 pagesMeasuring Differentiation SelfDeborah NgaNo ratings yet
- Print APT 2002 Culliford 249 58Document14 pagesPrint APT 2002 Culliford 249 58elvineNo ratings yet
- The Revised Intrinsic/Extrinsic Religious Orientation Scale in A Sample of Attica's InhabitantsDocument12 pagesThe Revised Intrinsic/Extrinsic Religious Orientation Scale in A Sample of Attica's InhabitantslathNo ratings yet
- Family Therapy Literature ReviewDocument4 pagesFamily Therapy Literature Reviewafdtalblw100% (2)
- Harker Washington 0250E 19146Document109 pagesHarker Washington 0250E 19146CHEE KOK SENGNo ratings yet
- Measures of Psychological Stress and Physical Health in Family Caregivers of Stroke Survivors A Literature ReviewDocument11 pagesMeasures of Psychological Stress and Physical Health in Family Caregivers of Stroke Survivors A Literature ReviewaNo ratings yet
- Article in Press: Alexander Moreira-Almeida, Harold G. KoenigDocument5 pagesArticle in Press: Alexander Moreira-Almeida, Harold G. KoenigCristina ArionNo ratings yet
- Autopercepción MortalidadDocument10 pagesAutopercepción MortalidadEduardo JohannesNo ratings yet
- Gore Et Al 2018 Forecasting Changes in ReligiosityDocument26 pagesGore Et Al 2018 Forecasting Changes in ReligiosityLeRonNo ratings yet
- Underwood Teres IDocument12 pagesUnderwood Teres ILizucaPatrocleNo ratings yet
- An Exploratory Study of Religious Involvement As A Moderator Between Anxiety, Depressive Symptoms and Quality of Life Outcomes of Older AdultsDocument12 pagesAn Exploratory Study of Religious Involvement As A Moderator Between Anxiety, Depressive Symptoms and Quality of Life Outcomes of Older AdultsaryaNo ratings yet
- Test UploadDocument12 pagesTest UploadIzzuddin KhalisNo ratings yet
- Social RelationshipDocument7 pagesSocial RelationshipAurelia AnankeNo ratings yet
- A Literature Review of Western Bereavement TheoryDocument6 pagesA Literature Review of Western Bereavement TheoryafmzndvyddcoioNo ratings yet
- Shalini Lal StudyDocument11 pagesShalini Lal StudyPeterNo ratings yet
- Death Anxiety 1Document7 pagesDeath Anxiety 1BeeHoofNo ratings yet
- Resilience in Family Members of Persons With Autism Spectrum Disorder A Review of The LiteratureDocument13 pagesResilience in Family Members of Persons With Autism Spectrum Disorder A Review of The LiteratureFatma Azmi AndriniNo ratings yet
- Aging and ReligiusDocument15 pagesAging and ReligiusFelipe Vázquez PalaciosNo ratings yet
- Caregiver Burden, Spirituality, and Psychological Well-Being Parents of Having Children With ThalassemiaDocument15 pagesCaregiver Burden, Spirituality, and Psychological Well-Being Parents of Having Children With ThalassemiamurvinandNo ratings yet
- Gilang Pandu Akbar - The Effect of An Islamic-Based Intervention On Depression and Anxiety in MalaysiaDocument14 pagesGilang Pandu Akbar - The Effect of An Islamic-Based Intervention On Depression and Anxiety in MalaysiaGilang pandu akbarNo ratings yet
- Ansiedade SocialDocument12 pagesAnsiedade Socialvemec31798No ratings yet
- Importance of HealthDocument11 pagesImportance of Healthtatiana.gordiencoNo ratings yet
- Capacidad de Resiliencia Segun Creencia en Dios y Sexo en Estudiantes UniversitariosDocument11 pagesCapacidad de Resiliencia Segun Creencia en Dios y Sexo en Estudiantes UniversitariosIJAR JOURNALNo ratings yet
- Mental Health Literature Review ExampleDocument8 pagesMental Health Literature Review Examplec5g10bt2100% (1)
- 1 s2.0 S0277953607001499 MainDocument17 pages1 s2.0 S0277953607001499 MainOana OrosNo ratings yet
- 2008 Article 24134Document15 pages2008 Article 24134MerryMerdekawatiNo ratings yet
- Religious Training and Religiosity in Psychiatry Residency ProgramsDocument7 pagesReligious Training and Religiosity in Psychiatry Residency Programsbdalcin5512No ratings yet
- Is Church Important for Mental HealthDocument17 pagesIs Church Important for Mental HealthSamNo ratings yet
- Nihms 1520387 ResilienceDocument18 pagesNihms 1520387 Resilienceari kurniawatiNo ratings yet
- Literature Review On Mental Health NursingDocument7 pagesLiterature Review On Mental Health Nursingafmzzgeqdsedez100% (1)
- Resubmission of Research Topic Proposal BS Psychology 3-3 Group 3Document7 pagesResubmission of Research Topic Proposal BS Psychology 3-3 Group 3Nathalie Aira GarvidaNo ratings yet
- Mental Health and Palliative Care Literature ReviewDocument4 pagesMental Health and Palliative Care Literature ReviewafdtbwkhbNo ratings yet
- Integrative Pathways: Navigating Chronic Illness with a Mind-Body-Spirit ApproachFrom EverandIntegrative Pathways: Navigating Chronic Illness with a Mind-Body-Spirit ApproachNo ratings yet
- DNA Affirmative - MSDI 2015Document146 pagesDNA Affirmative - MSDI 2015Michael TangNo ratings yet
- Chirag STDocument18 pagesChirag STchiragNo ratings yet
- Vincent Ira B. Perez: Barangay Gulod, Calatagan, BatangasDocument3 pagesVincent Ira B. Perez: Barangay Gulod, Calatagan, BatangasJohn Ramsel Boter IINo ratings yet
- Catalogo Head FixDocument8 pagesCatalogo Head FixANDREA RAMOSNo ratings yet
- Abbreviation Meaning Notes: Cibo ("With Food")Document4 pagesAbbreviation Meaning Notes: Cibo ("With Food")TantriNo ratings yet
- 8.4 Example: Swiss Market Index (SMI) : 188 8 Models of VolatilityDocument3 pages8.4 Example: Swiss Market Index (SMI) : 188 8 Models of VolatilityNickesh ShahNo ratings yet
- Presentation 1Document20 pagesPresentation 1nikitakhanduja1304No ratings yet
- SS1c MIDTERMS LearningModuleDocument82 pagesSS1c MIDTERMS LearningModuleBryce VentenillaNo ratings yet
- Best Home Oxygen Concentrators-Lowest Prices & Fast Shipping (Oxygen Machines) - 2021 - YuwellDocument1 pageBest Home Oxygen Concentrators-Lowest Prices & Fast Shipping (Oxygen Machines) - 2021 - YuwellPelayanan ResusitasiNo ratings yet
- BCRW Course - Answer-Booklet PDFDocument18 pagesBCRW Course - Answer-Booklet PDFSarah ChaudharyNo ratings yet
- Time Table Semester II 2019-2020Document18 pagesTime Table Semester II 2019-2020Shiv Kumar MeenaNo ratings yet
- SolarBright MaxBreeze Solar Roof Fan Brochure Web 1022Document4 pagesSolarBright MaxBreeze Solar Roof Fan Brochure Web 1022kewiso7811No ratings yet
- Multivariate Analysis Homework QuestionsDocument2 pagesMultivariate Analysis Homework Questions歐怡君No ratings yet
- Omobonike 1Document13 pagesOmobonike 1ODHIAMBO DENNISNo ratings yet
- AIOUDocument2 pagesAIOUHoorabwaseemNo ratings yet
- Polygenic InheritanceDocument13 pagesPolygenic InheritanceSandeep Kumar RaghuvanshiNo ratings yet
- List of household items for relocationDocument4 pagesList of household items for relocationMADDYNo ratings yet
- Siga-Cc1 12-22-2010Document6 pagesSiga-Cc1 12-22-2010Felipe LozanoNo ratings yet
- Business Analysis FoundationsDocument39 pagesBusiness Analysis FoundationsPriyankaNo ratings yet
- C11 Strategy DevelopmentDocument30 pagesC11 Strategy DevelopmentPARTI KEADILAN RAKYAT NIBONG TEBALNo ratings yet
- Olympic Ayres Magic LyricsDocument1 pageOlympic Ayres Magic Lyricsjackliddy96No ratings yet
- Inventory Storage and Retrieval System PatentDocument15 pagesInventory Storage and Retrieval System PatentdevanasokaNo ratings yet
- QP P1 APR 2023Document16 pagesQP P1 APR 2023Gil legaspiNo ratings yet
- MECHANICAL PROPERTIES OF SOLIDSDocument39 pagesMECHANICAL PROPERTIES OF SOLIDSAbdul Musavir100% (1)
- DLL Grade7 First 1solutions ConcentrationDocument5 pagesDLL Grade7 First 1solutions ConcentrationJaneth de JuanNo ratings yet
- OMR Sheet Has Been Attached at The End: EST Erial ODocument8 pagesOMR Sheet Has Been Attached at The End: EST Erial OSangeeta BansalNo ratings yet
- Organizational Behaviour Group Assignment-2Document4 pagesOrganizational Behaviour Group Assignment-2Prateek KurupNo ratings yet
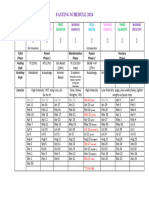
- Moon Fast Schedule 2024Document1 pageMoon Fast Schedule 2024mimiemendoza18No ratings yet