You might also like
- Se LF Di SC Ip Li NeDocument9 pagesSe LF Di SC Ip Li NeHannah Andrea Laparan100% (2)
- Lean Body DietDocument68 pagesLean Body DietManiraj PalanikaniNo ratings yet
- Where The Money Is in 2021Document34 pagesWhere The Money Is in 2021FidelisNo ratings yet
- Stress ManagementDocument54 pagesStress ManagementDen Pamplona100% (4)
- NSTP-CWTS 2 Chapter 2Document13 pagesNSTP-CWTS 2 Chapter 2Jaymark Enoy75% (4)
- Improving Hospital Performance and Productivity With The Balanced Scorecard - 2Document22 pagesImproving Hospital Performance and Productivity With The Balanced Scorecard - 2Yunita Soraya HusinNo ratings yet
- Community Outreach Programs and Extension Servicesof The Pangasinan State UniversityDocument13 pagesCommunity Outreach Programs and Extension Servicesof The Pangasinan State UniversityJeff PereyrasNo ratings yet
- Reach out Africa: Studies in Community Empowerment, Sustainable Development, and Cross-Cultural EngagementFrom EverandReach out Africa: Studies in Community Empowerment, Sustainable Development, and Cross-Cultural EngagementNo ratings yet
- The AAS Personal StatementDocument3 pagesThe AAS Personal StatementRetno Suminar100% (3)
- 6546 27022 1 PBDocument22 pages6546 27022 1 PBascarolineeNo ratings yet
- A Pilot Implementation of Interprofessional Education in A Community-Academe Partnership in The PhilipinessDocument8 pagesA Pilot Implementation of Interprofessional Education in A Community-Academe Partnership in The PhilipinessMada Pasalli SaludungNo ratings yet
- Cbme 1Document3 pagesCbme 1Waqar JeelaniNo ratings yet
- A Qualitative Evaluation of The Impact of A Palliative Care Course On Preregistration Nursing Students' Practice in CameroonDocument14 pagesA Qualitative Evaluation of The Impact of A Palliative Care Course On Preregistration Nursing Students' Practice in Cameroonkuro hanabusaNo ratings yet
- Kelly 2014Document5 pagesKelly 2014Anggoro OctaNo ratings yet
- The Essential Conditions Needed (EN)Document16 pagesThe Essential Conditions Needed (EN)WILLIAM GRANJA ANGULONo ratings yet
- "Being The Light": A Case Study On The Guidance Counselors' Struggles During The COVID-19 PandemicDocument10 pages"Being The Light": A Case Study On The Guidance Counselors' Struggles During The COVID-19 PandemicJase AngNo ratings yet
- Tutoría Entre Iguales en Una Escuela de Medicina Percepciones de Tutores y TutoradosDocument7 pagesTutoría Entre Iguales en Una Escuela de Medicina Percepciones de Tutores y TutoradosFalconSerfinNo ratings yet
- MNC Annual Report Bolinto TabinDocument5 pagesMNC Annual Report Bolinto TabinRainier Moreno-LacalleNo ratings yet
- s12909 019 1740 6Document13 pagess12909 019 1740 6Hàn Nguyệt CátNo ratings yet
- Community-Based Research WEB 1 PDFDocument4 pagesCommunity-Based Research WEB 1 PDFAnonymous QqyLDoW1No ratings yet
- PAILAGA ReflectionDocument2 pagesPAILAGA ReflectionTiara Ysabella PailagaNo ratings yet
- Recruitment of Caregivers Into Health Services ResDocument10 pagesRecruitment of Caregivers Into Health Services ResMónica Encantado GaboleiroNo ratings yet
- PASCOM Letter Practices in Teaching Community Medicine Amidst The Pandemic.v05062020Document3 pagesPASCOM Letter Practices in Teaching Community Medicine Amidst The Pandemic.v05062020MDreamerNo ratings yet
- The Nursing Centre As A Collaborative Approach To Integrate Community Health Service and Nursing Education in IndonesiaDocument3 pagesThe Nursing Centre As A Collaborative Approach To Integrate Community Health Service and Nursing Education in IndonesiaTentry Fuji PurwantiNo ratings yet
- Family Adoption Programme For Medical UndergraduatDocument5 pagesFamily Adoption Programme For Medical UndergraduatD SunnyNo ratings yet
- Advanced Practice Nursing Education: Opening Doors To Community CollaborationDocument4 pagesAdvanced Practice Nursing Education: Opening Doors To Community Collaborationscifer_06No ratings yet
- Harrington Costa Rica Recommendation Report 2014Document17 pagesHarrington Costa Rica Recommendation Report 2014Ayuba Adamu PampammiNo ratings yet
- Academic Experiences, Physical and Mental Health Impact of COVID-19 Pandemic On Students and Lecturers in Health Care EducationDocument13 pagesAcademic Experiences, Physical and Mental Health Impact of COVID-19 Pandemic On Students and Lecturers in Health Care Educationluis renzoNo ratings yet
- 2022 Civic ResponsibilityDocument6 pages2022 Civic ResponsibilityDr. Sajida NaseemNo ratings yet
- Residency Training Program: Perceptions of Residents: June 2010Document5 pagesResidency Training Program: Perceptions of Residents: June 2010habtishNo ratings yet
- Preceptor 1Document7 pagesPreceptor 1Stevanus JonathanNo ratings yet
- Online Problem-Based Learning (PBL) During Coronavirus Pandemic: Trial at The Libyan International Medical UniversityDocument7 pagesOnline Problem-Based Learning (PBL) During Coronavirus Pandemic: Trial at The Libyan International Medical UniversityIJAR JOURNALNo ratings yet
- Targeting The Poor of The Sitios ThroughDocument18 pagesTargeting The Poor of The Sitios Throughsherwintarong0No ratings yet
- Journal Extension PDFDocument5 pagesJournal Extension PDFLAILANIE DELA PENANo ratings yet
- Prof Final WorkDocument39 pagesProf Final WorkabdulmuuteehNo ratings yet
- Hybrid SyllabusDocument22 pagesHybrid SyllabusJenni CavanaughNo ratings yet
- Helpful BookDocument68 pagesHelpful BookMubashar HussainNo ratings yet
- NSTP 1 CWTS Module 1Document15 pagesNSTP 1 CWTS Module 1Kyle SoveranoNo ratings yet
- Community Based Education PDFDocument2 pagesCommunity Based Education PDFAngel100% (1)
- Medu 14194Document2 pagesMedu 14194ZoeNo ratings yet
- Best Practise in Community EngagementDocument60 pagesBest Practise in Community EngagementBimalHPatelNo ratings yet
- Nursing and Midwifery StudentsDocument15 pagesNursing and Midwifery StudentsJumariah Tana PaserNo ratings yet
- 8 1formalreportrevisedDocument12 pages8 1formalreportrevisedapi-285547750No ratings yet
- Keywords: School of Accountancy, Business and Hospitality, Community EngagementDocument26 pagesKeywords: School of Accountancy, Business and Hospitality, Community EngagementPrecious Joy Sumer AgdeppaNo ratings yet
- Teaching Clinical Reasoning: A New Playbook: Covid-19 InsightsDocument4 pagesTeaching Clinical Reasoning: A New Playbook: Covid-19 InsightsMahmoud AbouelsoudNo ratings yet
- Blended Learning For PostgraduateDocument7 pagesBlended Learning For PostgraduateAnonymous GOUaH7FNo ratings yet
- The Outcomes of A Mobile Learning Intervention For Teaching BioethicsDocument13 pagesThe Outcomes of A Mobile Learning Intervention For Teaching Bioethicssara.qmcNo ratings yet
- Facilitating LeDocument6 pagesFacilitating LeKarl SiganayNo ratings yet
- Rural Healthcare Providers Coping With Clinical CaDocument9 pagesRural Healthcare Providers Coping With Clinical CaSamuelAshleyNo ratings yet
- Global Faculty Development: Lessons Learned From The Foundation For Advancement of International Medical Education and Research (FAIMER) InitiativesDocument3 pagesGlobal Faculty Development: Lessons Learned From The Foundation For Advancement of International Medical Education and Research (FAIMER) InitiativesawaNo ratings yet
- Sharma - Medical School Lectures  As Dead As The DodoDocument2 pagesSharma - Medical School Lectures  As Dead As The Dododelap05No ratings yet
- Navigation Programs To Support Community-Dwelling Individuals With Life-Limiting Illness: Determinants of ImplementationDocument11 pagesNavigation Programs To Support Community-Dwelling Individuals With Life-Limiting Illness: Determinants of ImplementationarysiaNo ratings yet
- CHN 1 Prelim Module Week 2Document9 pagesCHN 1 Prelim Module Week 2Joshua AysonNo ratings yet
- Community Dialogues For Healthy Children: Encouraging Communities To TalkDocument32 pagesCommunity Dialogues For Healthy Children: Encouraging Communities To Talkmalaria_consortiumNo ratings yet
- Community-Based Health-Professions Interprofessional Education: A Collaborative and Sustainable ModelDocument8 pagesCommunity-Based Health-Professions Interprofessional Education: A Collaborative and Sustainable ModelRizki irsyad MaulanaNo ratings yet
- Level of Awareness, Implemenattiona ND Engagement On The Community Outreach ProgramDocument9 pagesLevel of Awareness, Implemenattiona ND Engagement On The Community Outreach ProgramLeonilo B CapulsoNo ratings yet
- Community Extension Services BodyDocument17 pagesCommunity Extension Services BodyDhanessa CondesNo ratings yet
- Syllabus Hiv AidsDocument3 pagesSyllabus Hiv Aidsniketut alit arminiNo ratings yet
- Ojt LogbookDocument12 pagesOjt LogbookSandy UyNo ratings yet
- Creative Fieldwork Solutions Shifting The Paradigm AotaDocument8 pagesCreative Fieldwork Solutions Shifting The Paradigm Aotaapi-699389850No ratings yet
- Primary Health Care in Jamkhed, IndiaDocument5 pagesPrimary Health Care in Jamkhed, IndiaJay WalleNo ratings yet
- Article 2 (Teamwork) MGT648 PDFDocument9 pagesArticle 2 (Teamwork) MGT648 PDFNatasya ShaNo ratings yet
- AbstractDocument13 pagesAbstractDOH EAMC Healthcare Navigation and ReferralNo ratings yet
- ETEC 520 Assignment #1Document14 pagesETEC 520 Assignment #1Diana NgNo ratings yet
- The Impact and The Challenges ofDocument9 pagesThe Impact and The Challenges ofMarco A J OrtizNo ratings yet
- 3019-Article Text-7114-1-10-20190710Document14 pages3019-Article Text-7114-1-10-20190710CMP_0803No ratings yet
- Planning of Action (Poa) Hse Program Proposed For Pt. Abc: PIC Schedule Remark Description ADocument2 pagesPlanning of Action (Poa) Hse Program Proposed For Pt. Abc: PIC Schedule Remark Description Aru dieNo ratings yet
- Katherine E. Stickels: ObjectivesDocument4 pagesKatherine E. Stickels: Objectivesapi-358969355No ratings yet
- Unit 5 Midterm MN566Document6 pagesUnit 5 Midterm MN566Jhouleen Angelika TamNo ratings yet
- Safety Data Sheet: Section 1. IdentificationDocument15 pagesSafety Data Sheet: Section 1. IdentificationRaffey Navarroza100% (1)
- Science Dept Ci TeamfinalDocument29 pagesScience Dept Ci TeamfinalEmely EstacioNo ratings yet
- Middle School Physical Education HomeworkDocument8 pagesMiddle School Physical Education Homeworkh41zdb84100% (1)
- CAP ADHD Form PDFDocument1 pageCAP ADHD Form PDFrohailNo ratings yet
- Memory Loss & 10 Early Signs of Alzheimer's - Alzheimer's AssociationDocument9 pagesMemory Loss & 10 Early Signs of Alzheimer's - Alzheimer's AssociationRatnaPrasadNalamNo ratings yet
- Altamash Shabbir Maniyar Resume 22-05-2023-04-03-54 230601 200613Document3 pagesAltamash Shabbir Maniyar Resume 22-05-2023-04-03-54 230601 200613Kanhaiya VermaNo ratings yet
- Bladder Training Stroke PDFDocument10 pagesBladder Training Stroke PDFLeony KhairunisaNo ratings yet
- 2011 Wingspread Forum ReportDocument74 pages2011 Wingspread Forum ReportCenterForCitizenDiplomacyNo ratings yet
- Practical Research 1Document2 pagesPractical Research 1jillianeNo ratings yet
- BritanniaDocument269 pagesBritanniaAnushkaa GuptaNo ratings yet
- The Need For Time Management Training Is Universal: Evidence From TurkeyDocument8 pagesThe Need For Time Management Training Is Universal: Evidence From TurkeyAnil AkhterNo ratings yet
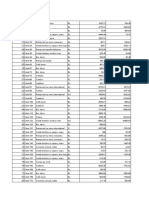
- Baza Date Test Excel - Varianta 2019 FADocument654 pagesBaza Date Test Excel - Varianta 2019 FAMierlea Alexandru-Nicolae100% (1)
- Plan of Care PaperDocument5 pagesPlan of Care Paperapi-548969267No ratings yet
- Darling Hammond2019 PDFDocument45 pagesDarling Hammond2019 PDFsantimosNo ratings yet
- LLL - Week 1Document9 pagesLLL - Week 1Reggie AbañoNo ratings yet
- Virtual Trials and Real-World Evidence Data CollectionDocument4 pagesVirtual Trials and Real-World Evidence Data CollectionRoopali AggarwalNo ratings yet
- Medi 99 E11005Document6 pagesMedi 99 E11005maninagaNo ratings yet
- Alcohol ResearcDocument85 pagesAlcohol ResearcEmmanuel de LeonNo ratings yet
- Lessons From The Borderline Anthropology, Psychiatry and The Risks of Being HumanDocument10 pagesLessons From The Borderline Anthropology, Psychiatry and The Risks of Being HumanDaniel Blanco VaroNo ratings yet
- Proposal Form New India Mediclaim Policy 01102021Document6 pagesProposal Form New India Mediclaim Policy 01102021abcdefabcNo ratings yet
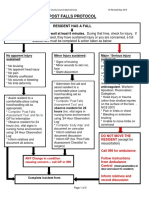
- 4-Hampshire Falls ProtocolDocument5 pages4-Hampshire Falls ProtocolsheenaNo ratings yet