You might also like
- Dungeon Master's SheetDocument1 pageDungeon Master's SheetJuan MonsalveNo ratings yet
- Customer Experience Journey MapDocument1 pageCustomer Experience Journey MapdiazortegaNo ratings yet
- Diagnostic Criteria Examination Form PDFDocument2 pagesDiagnostic Criteria Examination Form PDFNor Nadia Zakaria50% (2)
- Topic 6 Internship ReflectionDocument4 pagesTopic 6 Internship Reflectionapi-490976435No ratings yet
- CprtableDocument1 pageCprtableJohanna ChavezNo ratings yet
- Bridge 10 35m-Abutment A ScheduleDocument1 pageBridge 10 35m-Abutment A Schedulerichard almirolNo ratings yet
- RUBRIC - Speech DemonstrationDocument1 pageRUBRIC - Speech DemonstrationYuGenNo ratings yet
- Link ClickDocument2 pagesLink Clicke291083No ratings yet
- PTE PTE PTE PTE PTE: SangrurDocument1 pagePTE PTE PTE PTE PTE: SangrurSukhDeolNo ratings yet
- Customer Experience Journey Map: Stage 1 Stage 2 Stage 3 Stage 4 Stage 5 Stage 6Document1 pageCustomer Experience Journey Map: Stage 1 Stage 2 Stage 3 Stage 4 Stage 5 Stage 6Anthony RobertsNo ratings yet
- Haha Bitch PDFDocument1 pageHaha Bitch PDFNatakka AlbertsNo ratings yet
- Aida ModelDocument19 pagesAida Modelsiddharth devnaniNo ratings yet
- PTE PTE PTE PTE PTE: SangrurDocument1 pagePTE PTE PTE PTE PTE: SangrurSukhDeolNo ratings yet
- 1 ST Grade FULLDocument1 page1 ST Grade FULLwok69erNo ratings yet
- Anti LockBrakersCircuitDocument1 pageAnti LockBrakersCircuitNicolás García AlbaNo ratings yet
- Chapter 005Document31 pagesChapter 005Akshaya DNo ratings yet
- WoundauditDocument84 pagesWoundauditJaysie BeauNo ratings yet
- SCHOOL FORM 4.wordDocument22 pagesSCHOOL FORM 4.wordDecember CoolNo ratings yet
- Spell Save DC Cantrips Known Spells Prepared 1st 2nd 3rd 4th 5th 6th 7th 8th 9thDocument1 pageSpell Save DC Cantrips Known Spells Prepared 1st 2nd 3rd 4th 5th 6th 7th 8th 9thDenis SaavedraNo ratings yet
- Domain and Range Set and Interval NotationsDocument1 pageDomain and Range Set and Interval NotationsHafsa KhanNo ratings yet
- Medical and Pharmacy Abbreviations (Sig Codes) : Abbreviation Meaning(s) CategoryDocument3 pagesMedical and Pharmacy Abbreviations (Sig Codes) : Abbreviation Meaning(s) Categoryscope 3901No ratings yet
- Yawar Trade S.A.C.: Formato Resumen Del Dia - Clasificacion VehicularDocument1 pageYawar Trade S.A.C.: Formato Resumen Del Dia - Clasificacion VehicularDiego Condori CervantesNo ratings yet
- Formato de Data GPSDocument3 pagesFormato de Data GPSlut80No ratings yet
- Analisa Lalu Lintas (1 HARI)Document121 pagesAnalisa Lalu Lintas (1 HARI)Rizki RikiNo ratings yet
- Posyandu Semangka TPDocument13 pagesPosyandu Semangka TPNovi AriyantoNo ratings yet
- Posyandu Kemuning KDDocument13 pagesPosyandu Kemuning KDNovi AriyantoNo ratings yet
- Posyandu Mawar 6Document13 pagesPosyandu Mawar 6Novi AriyantoNo ratings yet
- Posyandu Melati 1 MandalasariDocument13 pagesPosyandu Melati 1 MandalasariNovi AriyantoNo ratings yet
- DegalemDocument6 pagesDegalemsilesh mulunehNo ratings yet
- Sciencedirect SciencedirectDocument7 pagesSciencedirect SciencedirectJohnny SimpNo ratings yet
- Product Selection Guide HansatonDocument6 pagesProduct Selection Guide HansatonAUDIOLOGIA AUDISER0% (1)
- Admission Form 2022 BADocument3 pagesAdmission Form 2022 BAJe Da MeiNo ratings yet
- Anexo. Enlace Malvilla. 2018Document6 pagesAnexo. Enlace Malvilla. 2018ivan gerardo matos jaraNo ratings yet
- Course Registration Fee Course Registration Fee Course Registration Fee Course Registration FeeDocument1 pageCourse Registration Fee Course Registration Fee Course Registration Fee Course Registration FeeMian Jobs Sangla HillNo ratings yet
- Technology and Livelihood Education SY: 2020 - 2021Document2 pagesTechnology and Livelihood Education SY: 2020 - 2021Roniel BalverdeNo ratings yet
- Tools and EquipmentsDocument2 pagesTools and EquipmentsRoniel BalverdeNo ratings yet
- Anexo. Enlace Melipilla. 2018Document8 pagesAnexo. Enlace Melipilla. 2018ivan gerardo matos jaraNo ratings yet
- Branch Code: Branch Code: Branch Code:: Registration No. Registration No. Registration NoDocument1 pageBranch Code: Branch Code: Branch Code:: Registration No. Registration No. Registration NoSrimannarayana NandamNo ratings yet
- Umg 96sDocument96 pagesUmg 96sBima Dwi PSNo ratings yet
- Samboan FSDocument6 pagesSamboan FSalvic rodaNo ratings yet
- Anexo. Enlace Luis Reus. 2018Document5 pagesAnexo. Enlace Luis Reus. 2018ivan gerardo matos jaraNo ratings yet
- Maroochy Spell SheetDocument1 pageMaroochy Spell SheetwineCentric 'Matthew Lewis'No ratings yet
- 2007 Ford Ranger 2007 Ford Ranger: System Wiring Diagrams System Wiring DiagramsDocument1 page2007 Ford Ranger 2007 Ford Ranger: System Wiring Diagrams System Wiring DiagramsJonas LugoNo ratings yet
- Matriks Klinis Puskesmas TBDocument117 pagesMatriks Klinis Puskesmas TBigaNo ratings yet
- Cuatricomia - Calle Maldonado Luis David-1Document2 pagesCuatricomia - Calle Maldonado Luis David-1Francisco SacotoNo ratings yet
- Exp IV Spectrometer WavelengthDocument12 pagesExp IV Spectrometer Wavelengthharshitsharma.siwalNo ratings yet
- Course Registration Fee Course Registration Fee Course Registration Fee Course Registration FeeDocument1 pageCourse Registration Fee Course Registration Fee Course Registration Fee Course Registration FeeAhtasham AmeenNo ratings yet
- TQL 2012 Web PDFDocument78 pagesTQL 2012 Web PDFHaroldNo ratings yet
- Penilaian Standar Kinerja: InstrumenDocument117 pagesPenilaian Standar Kinerja: Instrumenintan pratiwiNo ratings yet
- Autoranging Combiscope pm3370bDocument478 pagesAutoranging Combiscope pm3370bjohn doeNo ratings yet
- Control - Statistical Process Control SPCDocument22 pagesControl - Statistical Process Control SPCHalimNo ratings yet
- Checklist LatestDocument1 pageChecklist LatestTNN EntNo ratings yet
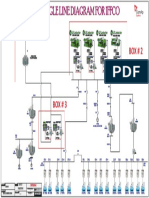
- Step Down Transformers: Single Line Diagram For IffcoDocument1 pageStep Down Transformers: Single Line Diagram For IffcoManahil KhalilNo ratings yet
- Wuolah Free STATISTICS 3Document14 pagesWuolah Free STATISTICS 3pabloenriquerh28No ratings yet
- 8WC 2020 - Wow 10 PDFDocument2 pages8WC 2020 - Wow 10 PDFBNo ratings yet
- Matriks Klinis Puskesmas KosongDocument117 pagesMatriks Klinis Puskesmas KosongJenda Muli SembiringNo ratings yet
- Tac451 Vocab List Bab 3Document1 pageTac451 Vocab List Bab 3rosameizaNo ratings yet
- Reference Cells, Formula Auiditng, ShortcutsDocument3 pagesReference Cells, Formula Auiditng, ShortcutsBhavya NawalakhaNo ratings yet
- Tasks Workbook PR 2018 11EDocument9 pagesTasks Workbook PR 2018 11EUsama SuriyaNo ratings yet
- Ultimate NLP Practitioner Training ProgramDocument2 pagesUltimate NLP Practitioner Training ProgramPreetiBhambhaniNo ratings yet
- Awatani 1975Document6 pagesAwatani 1975Ilmal YaqinNo ratings yet
- Inter Traffic Preview DigitalDocument60 pagesInter Traffic Preview DigitalAkash SinhaNo ratings yet
- Annotated BibliographyDocument6 pagesAnnotated Bibliographyapi-302100895No ratings yet
- Contribution of Tax Morale and Compliance Costs To Tax Compliance of Micro and Small Scale Enterprises in GhanaDocument20 pagesContribution of Tax Morale and Compliance Costs To Tax Compliance of Micro and Small Scale Enterprises in GhanaLealyn CuestaNo ratings yet
- Lesson Four: Vocabulary: Vocabulary WordsDocument2 pagesLesson Four: Vocabulary: Vocabulary WordsKristine BocciaNo ratings yet
- NSEP Above MasDocument63 pagesNSEP Above MasMDPCOS SCHOOLNo ratings yet
- CSC128 - Test - 8 July 2021 (Question) UiTM PENANGDocument8 pagesCSC128 - Test - 8 July 2021 (Question) UiTM PENANGMuhd Alif MikhailNo ratings yet
- SSRBM Jeevan Bhima Nagar Handbook 2023-24 - 0 - 1Document9 pagesSSRBM Jeevan Bhima Nagar Handbook 2023-24 - 0 - 1Kiran Kidiyappa ShivakumarNo ratings yet
- Appendix A Letter of RequestDocument6 pagesAppendix A Letter of RequestMarjorie ResuelloNo ratings yet
- Gao2007 PDFDocument5 pagesGao2007 PDFAnonymous cYpEVvoNo ratings yet
- Lenovo Z370Z470Z570 Hardware Maintenance Manual V1.0Document120 pagesLenovo Z370Z470Z570 Hardware Maintenance Manual V1.0Anna Lissa PilapilNo ratings yet
- Benz 968590164562 20171230224054Document5 pagesBenz 968590164562 20171230224054عمار ميسينيNo ratings yet
- Quiz On Chapter Eleven PDFDocument7 pagesQuiz On Chapter Eleven PDFNora LinNo ratings yet
- Validity and ReliabilityDocument6 pagesValidity and Reliabilitywedad jumaNo ratings yet
- Paper P-1.p65-1Document33 pagesPaper P-1.p65-1SantoshNo ratings yet
- MicronDocument6 pagesMicroncitaanindikaNo ratings yet
- Beginner Typing Lesson 1 - LEARN TYPINGDocument5 pagesBeginner Typing Lesson 1 - LEARN TYPINGThiyagu0% (1)
- PIA B2 - Module 2 (PHYSICS) SubModule 2.2 (Mechanics) FinalDocument82 pagesPIA B2 - Module 2 (PHYSICS) SubModule 2.2 (Mechanics) Finalsamarrana1234679No ratings yet
- FINALby REDAZADocument3 pagesFINALby REDAZANoreen RedazaNo ratings yet
- Self Inflating TyresDocument12 pagesSelf Inflating TyresRishabh DeedwaniyaNo ratings yet
- 2018-06-22 - Quantum Algorithms For Pattern Matching in Genomic Sequences - MSC ThesisDocument36 pages2018-06-22 - Quantum Algorithms For Pattern Matching in Genomic Sequences - MSC ThesisAritra SarkarNo ratings yet
- Behaviour Change For Sustainable Development: October 2018Document11 pagesBehaviour Change For Sustainable Development: October 2018Febrian Bagus SetiawanNo ratings yet
- Ubd Template 1Document5 pagesUbd Template 1api-405027829No ratings yet
- Chapter3-Requirement AnalysisDocument55 pagesChapter3-Requirement AnalysisShariar Parvez TonmoyNo ratings yet
- Bn68-09016a-01 QNQ8CB Asia Eng 180406.0Document24 pagesBn68-09016a-01 QNQ8CB Asia Eng 180406.0Parveen ArifNo ratings yet
- The Last Lesson NotesDocument11 pagesThe Last Lesson NotesAnvi Sameer TiwariNo ratings yet
- Exercise Physiology-LecturDocument102 pagesExercise Physiology-Lecturworku kassieNo ratings yet
- Deakin University: Lesson Planning Template: School of EducationDocument4 pagesDeakin University: Lesson Planning Template: School of EducationJessicaNo ratings yet