You might also like
- Acute Kidney Injury in HFDocument14 pagesAcute Kidney Injury in HFAnonymous NeRC5JYiSNo ratings yet
- Right Heart Failure and Cardiorenal Syndrome 2020Document18 pagesRight Heart Failure and Cardiorenal Syndrome 2020Raul FernandoNo ratings yet
- Cardiorenal Syndrome Review 2015Document7 pagesCardiorenal Syndrome Review 2015Chika SabaNo ratings yet
- Right Heart Failure and Cardiorenal SyndromeDocument18 pagesRight Heart Failure and Cardiorenal SyndromePedro AugustoNo ratings yet
- Oxford 2015Document17 pagesOxford 2015rosyidmawardi7No ratings yet
- Koniari 2011Document11 pagesKoniari 2011rosyidmawardi7No ratings yet
- Mon Anemia and CardiovascularDocument11 pagesMon Anemia and CardiovasculartyasNo ratings yet
- Price-Goldstein2009 Article CardiorenalSyndromeInChildrenWDocument8 pagesPrice-Goldstein2009 Article CardiorenalSyndromeInChildrenWEliana LopezNo ratings yet
- Therapeutic Options For The Management of The Cardiorenal SyndromeDocument11 pagesTherapeutic Options For The Management of The Cardiorenal SyndromeAntoine SchallerNo ratings yet
- Cardiorenal Syndrome Diagnosis and Management GuideDocument20 pagesCardiorenal Syndrome Diagnosis and Management GuideLucrecia BilancieriNo ratings yet
- Cardiorenal Syndrome - Cardiologist vs. Nephrologist - ACVIM 2014 - VINDocument5 pagesCardiorenal Syndrome - Cardiologist vs. Nephrologist - ACVIM 2014 - VINTactvisNo ratings yet
- Influence of Progressive Renal Dysfunction in Chronic Heart FailureDocument6 pagesInfluence of Progressive Renal Dysfunction in Chronic Heart Failurenandhini raguNo ratings yet
- Cardiorenal SyndromeDocument13 pagesCardiorenal Syndromenisa_kartikaNo ratings yet
- Hepato and Cardiorenal SyndromeDocument31 pagesHepato and Cardiorenal SyndromeanandababuNo ratings yet
- Bellomo Claudio Ronco, Mikko Haapio, Andrew A. House, Nagesh Anavekar, and RinaldoDocument15 pagesBellomo Claudio Ronco, Mikko Haapio, Andrew A. House, Nagesh Anavekar, and RinaldoEdgar Herrera Espino GalvánNo ratings yet
- Acute Cardiorenal Syndrome An UpdateDocument10 pagesAcute Cardiorenal Syndrome An UpdateErika Jiménez De LaraNo ratings yet
- High output heart failure: a reviewDocument7 pagesHigh output heart failure: a reviewChanvira Aria CandrayanaNo ratings yet
- Cardiorenal SyndromeDocument15 pagesCardiorenal SyndromeDrSunil Kumar KarnaNo ratings yet
- Patofisiologu Cardiorenal SyndromeDocument7 pagesPatofisiologu Cardiorenal SyndromeHarika PutraNo ratings yet
- Cardio-Renal Anemia SyndromeDocument11 pagesCardio-Renal Anemia SyndromeCecilia Casandra UneputtyNo ratings yet
- 07 Cardiorenal Syndrome PDFDocument22 pages07 Cardiorenal Syndrome PDFLucrecia BilancieriNo ratings yet
- Nursing Management of Patient With CCFDocument34 pagesNursing Management of Patient With CCFJayarani Ashok100% (1)
- Cardiorenal Syndrome Schrier R (Curr Cardiol Rep 2013)Document9 pagesCardiorenal Syndrome Schrier R (Curr Cardiol Rep 2013)Luis Gerardo Alcalá GonzálezNo ratings yet
- Cardiorenal Syndrome: Definition, Prevalence, Diagnosis, and PathophysiologyDocument14 pagesCardiorenal Syndrome: Definition, Prevalence, Diagnosis, and PathophysiologyOlga BabiiNo ratings yet
- Congestive Nephropathy: A Neglected Entity? Proposal For Diagnostic Criteria and Future PerspectivesDocument21 pagesCongestive Nephropathy: A Neglected Entity? Proposal For Diagnostic Criteria and Future PerspectivesMuhammad SyammNo ratings yet
- Aclinicalapproachtothe Acutecardiorenal Syndrome: Jacob C. Jentzer,, Lakhmir S. ChawlaDocument19 pagesAclinicalapproachtothe Acutecardiorenal Syndrome: Jacob C. Jentzer,, Lakhmir S. Chawlaiqe chanNo ratings yet
- Sindrom Jantung GinjalDocument10 pagesSindrom Jantung GinjalEmallia Phypiet FitrianiNo ratings yet
- Congestive Hepatopathy: Molecular SciencesDocument23 pagesCongestive Hepatopathy: Molecular SciencesRizky ValriansyahNo ratings yet
- Cardiorenal Syndrome Definition, Prevalence, Diagnosis and PathophysiologyDocument18 pagesCardiorenal Syndrome Definition, Prevalence, Diagnosis and PathophysiologyfelipetheNo ratings yet
- Sindrome HepatorenalDocument14 pagesSindrome HepatorenalAdrian DiazNo ratings yet
- Cardiorenal SyndromeDocument20 pagesCardiorenal SyndromeinarenhdcenNo ratings yet
- Heart Failure DDx and WorkupDocument3 pagesHeart Failure DDx and WorkupAizel ManiagoNo ratings yet
- 4.heart Failure HandoutDocument108 pages4.heart Failure HandoutGetachewNo ratings yet
- 2. Heart failureDocument61 pages2. Heart failurehadushnl770No ratings yet
- Cardiorenal Syndrome: Asist. Univ. DR Tanasa AnaDocument30 pagesCardiorenal Syndrome: Asist. Univ. DR Tanasa AnaSofia RhellabNo ratings yet
- Chronic Heart FailureDocument90 pagesChronic Heart FailureTemesgenNo ratings yet
- Anemia Dan JantungDocument5 pagesAnemia Dan JantungprimayosiNo ratings yet
- Heart FailureDocument10 pagesHeart FailureJajangNo ratings yet
- The Clinical Epidemiology of Cardiac Disease in Chronic Renal FailureDocument10 pagesThe Clinical Epidemiology of Cardiac Disease in Chronic Renal FailureRaden Mas IkhsanNo ratings yet
- Management of Heart Failure in Patients With ChronDocument9 pagesManagement of Heart Failure in Patients With ChronSiddhartha PalaciosNo ratings yet
- Nefropatia Congestiva 21Document21 pagesNefropatia Congestiva 21John Wesley BragaNo ratings yet
- Hypertensive Vascular DiseaseDocument5 pagesHypertensive Vascular DiseaseGenoMacaraanNo ratings yet
- Cardiorenal Syndrome Definition, Prevalence, Diagnosis, and PathophysiologyDocument17 pagesCardiorenal Syndrome Definition, Prevalence, Diagnosis, and PathophysiologyRafael Vieira lealNo ratings yet
- Peripheral Edema: ReviewDocument7 pagesPeripheral Edema: ReviewVmsdNo ratings yet
- Cardiorenal Syndrome in Chronic Kidney Disease: ReviewDocument9 pagesCardiorenal Syndrome in Chronic Kidney Disease: Reviewnisa_kartikaNo ratings yet
- Cardiorenal Syndrome: Definition, Prevalence, Diagnosis, and Pa Tho PhysiologyDocument10 pagesCardiorenal Syndrome: Definition, Prevalence, Diagnosis, and Pa Tho PhysiologySimone AquinoNo ratings yet
- ICCFEP, Falla Renal, 2021Document11 pagesICCFEP, Falla Renal, 2021GeovannaHGNo ratings yet
- Clinical PresentationsDocument37 pagesClinical PresentationsJim Christian EllaserNo ratings yet
- Anemia as a Risk Factor for Cardiovascular DiseaseDocument8 pagesAnemia as a Risk Factor for Cardiovascular DiseaseyusufNo ratings yet
- Manejo de La Insufiencia Cardica HtaDocument10 pagesManejo de La Insufiencia Cardica HtaNeiny FonsecaNo ratings yet
- Heart Failure and Liver DiseaseDocument11 pagesHeart Failure and Liver DiseaseFreddy PanjaitanNo ratings yet
- Cardiorenal Syndrome ExplainedDocument9 pagesCardiorenal Syndrome ExplainedThais Paiva TorresNo ratings yet
- 10.1038@s41581 018 0101 8Document17 pages10.1038@s41581 018 0101 8Ess liNo ratings yet
- Liver International - 2017 - M Ller - The Pathophysiology of Arterial Vasodilatation and Hyperdynamic Circulation inDocument11 pagesLiver International - 2017 - M Ller - The Pathophysiology of Arterial Vasodilatation and Hyperdynamic Circulation inVero GiraldoNo ratings yet
- Heart Failure & Cor PulmunaleDocument12 pagesHeart Failure & Cor PulmunaleShrestha AnjivNo ratings yet
- Mechanisms For Hemodynamic Instability Related To Renal Replacement Therapy: A Narrative ReviewDocument14 pagesMechanisms For Hemodynamic Instability Related To Renal Replacement Therapy: A Narrative Reviewvictor figueroaNo ratings yet
- Cardiorenal Syndrome: SciencedirectDocument10 pagesCardiorenal Syndrome: SciencedirectDwiFitriaAnggrainiNo ratings yet
- Cardiorenal Syndrome Referat Imam (BYS & EM)Document27 pagesCardiorenal Syndrome Referat Imam (BYS & EM)Afrilia IntanNo ratings yet
- Jurnal PMI 5Document8 pagesJurnal PMI 5Staying At JogyaNo ratings yet
- Safari(7)Document137 pagesSafari(7)Rajan JattNo ratings yet
- ISBPlacements Report 2023Document24 pagesISBPlacements Report 2023Gaurav RawatNo ratings yet
- SafariDocument7 pagesSafariRajan JattNo ratings yet
- Https:%2Fmdpi Res.com%2Fd Attachment%2Fijms%2Fijms 20 04976%2Farticle Deploy%2FiDocument15 pagesHttps:%2Fmdpi Res.com%2Fd Attachment%2Fijms%2Fijms 20 04976%2Farticle Deploy%2FiRajan JattNo ratings yet
- Introduction Biochemical Engineering PT 530Document82 pagesIntroduction Biochemical Engineering PT 530Rajan JattNo ratings yet
- Dipak Patil Opthalmic ReportsDocument5 pagesDipak Patil Opthalmic ReportsRajan JattNo ratings yet
- Company Profile PXCDocument6 pagesCompany Profile PXCRajan JattNo ratings yet
- Autism and Vaccination (Final)Document8 pagesAutism and Vaccination (Final)Rajan JattNo ratings yet
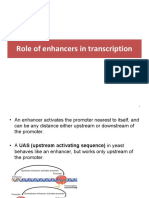
- 8 ROle of Enhancers in Trancription PDFDocument14 pages8 ROle of Enhancers in Trancription PDFRajan JattNo ratings yet
- Aerosol Gpat NotesDocument9 pagesAerosol Gpat NotesRajan JattNo ratings yet
- Drug InteractionsDocument13 pagesDrug InteractionsRajan JattNo ratings yet
- Important QuestionsDocument11 pagesImportant QuestionsRajan JattNo ratings yet
- PhotoDocument1 pagePhotoRajan JattNo ratings yet
- Https:/twin Sci-Hub Se/5948//howlett2008Document15 pagesHttps:/twin Sci-Hub Se/5948//howlett2008Rajan JattNo ratings yet
- Continuous CultureDocument33 pagesContinuous CultureRajan JattNo ratings yet
- DTU Casebook 2021-22Document136 pagesDTU Casebook 2021-22Prashant MishraNo ratings yet
- Pharma Earnings 2023 Q1Document20 pagesPharma Earnings 2023 Q1nimsi encisoNo ratings yet