You might also like
- Diabetes and Exercise: From Pathophysiology to Clinical ImplementationFrom EverandDiabetes and Exercise: From Pathophysiology to Clinical ImplementationJane E. B. Reusch, MDNo ratings yet
- Switch Olanzapin Ke RisperidonDocument10 pagesSwitch Olanzapin Ke RisperidonAnonymous Ca0YyWNnVNo ratings yet
- Hruby 2016Document7 pagesHruby 2016Sam Steven Hernandez JañaNo ratings yet
- 3 - (Ler) Estilos de Vida, Consequencias ObesidadeDocument7 pages3 - (Ler) Estilos de Vida, Consequencias ObesidadeMateus CarvalhoNo ratings yet
- Tsai2019 Obesity in The Clinic ACPDocument17 pagesTsai2019 Obesity in The Clinic ACPLuis RodriguezNo ratings yet
- Misclassification of Cardiometabolic Health When Using Body Mass Index Categories in NHANES 2005-2012Document5 pagesMisclassification of Cardiometabolic Health When Using Body Mass Index Categories in NHANES 2005-2012Maria Ignacia MacariNo ratings yet
- Popular Diets: A Scientific Review: Executive SummaryDocument5 pagesPopular Diets: A Scientific Review: Executive SummaryKarina ValenzuelaNo ratings yet
- Ioi70171 2461 2468Document8 pagesIoi70171 2461 2468jimmyneutron1337No ratings yet
- Ahei & HeiDocument12 pagesAhei & HeiBushra KainaatNo ratings yet
- Popular Diets: A Scientific Review: Obesity Research March 2001Document41 pagesPopular Diets: A Scientific Review: Obesity Research March 2001Akash.SNo ratings yet
- Obesityasadisease: Jagriti Upadhyay,, Olivia Farr,, Nikolaos Perakakis,, Wael Ghaly,, Christos MantzorosDocument21 pagesObesityasadisease: Jagriti Upadhyay,, Olivia Farr,, Nikolaos Perakakis,, Wael Ghaly,, Christos MantzorosAlejandra RamirezNo ratings yet
- Eckel 2018Document11 pagesEckel 2018dr.martynchukNo ratings yet
- Eating Behavior Correlates of Adult Weight Gain and Obesity in Healthy Women Aged 55-65 yDocument8 pagesEating Behavior Correlates of Adult Weight Gain and Obesity in Healthy Women Aged 55-65 yWahyuningsih HamidNo ratings yet
- Morbidity and Mortality Weekly ReportDocument27 pagesMorbidity and Mortality Weekly ReportsyaymaNo ratings yet
- Obesity in PlaDocument7 pagesObesity in PlaNadia AmroNo ratings yet
- Overweight and Obesity: Prevalence, Consequences, and Causes of A Growing Public Health ProblemDocument8 pagesOverweight and Obesity: Prevalence, Consequences, and Causes of A Growing Public Health ProblemSahrul FajarNo ratings yet
- Mehu131 U1 T6 Obesidad4Document16 pagesMehu131 U1 T6 Obesidad4Valeria Moretto VegaNo ratings yet
- Television Whatching and Other SedentaryDocument7 pagesTelevision Whatching and Other SedentaryROSIANE RONCHI NASCIMENTONo ratings yet
- RRL3 RLRLDocument18 pagesRRL3 RLRLRowena BayalanNo ratings yet
- Obesity 2019 AIMDocument17 pagesObesity 2019 AIMAndrea CorderoNo ratings yet
- jbr20304 76 79Document4 pagesjbr20304 76 79Jaime BusquetNo ratings yet
- Pearl 2017Document6 pagesPearl 2017Jes BakerNo ratings yet
- Preconception Care ofDocument11 pagesPreconception Care ofsipen poltekkesbdgNo ratings yet
- SJ Ijo 0800495Document23 pagesSJ Ijo 0800495Mohammad shaabanNo ratings yet
- Manu Et Al-2015-Acta Psychiatrica ScandinavicaDocument12 pagesManu Et Al-2015-Acta Psychiatrica ScandinavicamerianaNo ratings yet
- Health Impacts of ObesityDocument4 pagesHealth Impacts of Obesityhoneybee2005No ratings yet
- Glycemic index, glycemic load, and dietary fiber intakeDocument9 pagesGlycemic index, glycemic load, and dietary fiber intakeAlter EgoNo ratings yet
- Nej Mo A 1304501aasDocument12 pagesNej Mo A 1304501aasHadiyana Arief HafizNo ratings yet
- Precision Medicine of Obesity As An Integral Part of Type 2 Diabetes Management - Past, Present, and FutureDocument18 pagesPrecision Medicine of Obesity As An Integral Part of Type 2 Diabetes Management - Past, Present, and FutureAlexandra IstrateNo ratings yet
- Obesity and Hypertension Heart Failure ADocument9 pagesObesity and Hypertension Heart Failure Amercuryboss90No ratings yet
- Mediterranean Diet Intervention for Hispanic Women Reduces CVD RiskDocument21 pagesMediterranean Diet Intervention for Hispanic Women Reduces CVD RiskJanine RiofloridoNo ratings yet
- Exercise Is MedicineDocument5 pagesExercise Is MedicineGabriel FamaNo ratings yet
- 10 1016@j Jacc 2017 11 011Document16 pages10 1016@j Jacc 2017 11 011Anita YolandhaNo ratings yet
- Artigo 4Document2 pagesArtigo 4daisyscholliersNo ratings yet
- Comparison of Weight-Loss Diets With Different Compositions of Fat, Protein, and CarbohydratesDocument15 pagesComparison of Weight-Loss Diets With Different Compositions of Fat, Protein, and CarbohydratesMichael HubbertNo ratings yet
- Nutritional AssessmentDocument8 pagesNutritional AssessmentOutour KhNo ratings yet
- LowcarbdietinmanDocument7 pagesLowcarbdietinmanJoão DinizNo ratings yet
- Articulo HistologíaDocument10 pagesArticulo HistologíaBrenda RomeroNo ratings yet
- IMC-Dexa-gordura-Measuring Adiposity in Patients - The Utility of Body Mass Index (BMI), Percent Body Fat, and LeptinDocument8 pagesIMC-Dexa-gordura-Measuring Adiposity in Patients - The Utility of Body Mass Index (BMI), Percent Body Fat, and LeptinFabrício Boscolo Del VecchioNo ratings yet
- Obesity's Impacts on Health, Mental Health and SocietyDocument7 pagesObesity's Impacts on Health, Mental Health and SocietyLukaNo ratings yet
- Associations of diabesity with all‐cause and cardiovascular disease mortalityDocument10 pagesAssociations of diabesity with all‐cause and cardiovascular disease mortalityluis sanchezNo ratings yet
- Circulationaha 106 171016Document21 pagesCirculationaha 106 171016César Gonzalvo DíazNo ratings yet
- Chapter 1Document7 pagesChapter 1takumikurodaNo ratings yet
- Obesity A Review of Pathophysiology and Classific - 2023 - Mayo Clinic ProceediDocument16 pagesObesity A Review of Pathophysiology and Classific - 2023 - Mayo Clinic Proceedialerta.bfcmNo ratings yet
- Womenshealth & NutritionDocument5 pagesWomenshealth & Nutritionbragaru.vladNo ratings yet
- Kes Glop Aksu DiDocument8 pagesKes Glop Aksu DiNur AnniesaNo ratings yet
- A Prospective Study of Egg Consumption and Risk of Cardiovascular Disease in Men and WomenDocument8 pagesA Prospective Study of Egg Consumption and Risk of Cardiovascular Disease in Men and Womenkrazyj123No ratings yet
- Adipokines in Patients With Cancer Anorexia and Cachexia: Riginal RticleDocument7 pagesAdipokines in Patients With Cancer Anorexia and Cachexia: Riginal RticleAnna GozaliNo ratings yet
- Normal Weight Obesity SyndromeDocument13 pagesNormal Weight Obesity SyndromeMarcelo SabbatiniNo ratings yet
- Aula 1 - Comparison of Weight-Loss Diets With Different Compositions of Fat, Protein, and CarbohydrateDocument15 pagesAula 1 - Comparison of Weight-Loss Diets With Different Compositions of Fat, Protein, and CarbohydrateRayane SilvaNo ratings yet
- METAANALISISDocument15 pagesMETAANALISISjotame87No ratings yet
- The Role of Diabetes, Obesity, and Metabolic Syndrome in StrokeDocument7 pagesThe Role of Diabetes, Obesity, and Metabolic Syndrome in StrokeEmir SaricNo ratings yet
- 营养:疾病预防和治疗Document12 pages营养:疾病预防和治疗张芬No ratings yet
- Trends in Cardiovascular Health Metrics in Obese Adults: National Health and Nutrition Examination Survey (NHANES), 1988 - 2014Document20 pagesTrends in Cardiovascular Health Metrics in Obese Adults: National Health and Nutrition Examination Survey (NHANES), 1988 - 2014Desy YardinaNo ratings yet
- Pe Project Obesity: Name: Manas Kadam Class: XII A Commerce Roll No - 87Document32 pagesPe Project Obesity: Name: Manas Kadam Class: XII A Commerce Roll No - 87sahilNo ratings yet
- Meal Frequency and Timing Are Associated With Changes in Body Mass Index in Adventist Health Study 2Document7 pagesMeal Frequency and Timing Are Associated With Changes in Body Mass Index in Adventist Health Study 2Cristi CapetisNo ratings yet
- Solving Population-Wide Obesity - Progress and Future ProspectsDocument4 pagesSolving Population-Wide Obesity - Progress and Future ProspectsOumaima Ahaddouch ChiniNo ratings yet
- Obesity and CVDDocument19 pagesObesity and CVDAnindira RustandiNo ratings yet
- Diabetes and CancerDocument15 pagesDiabetes and CancerAriHendraWijayanti100% (1)
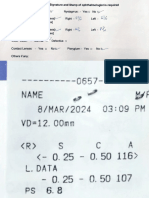
- Dipak Patil Opthalmic ReportsDocument5 pagesDipak Patil Opthalmic ReportsRajan JattNo ratings yet
- Safari(7)Document137 pagesSafari(7)Rajan JattNo ratings yet
- Https:%2Fmdpi Res.com%2Fd Attachment%2Fijms%2Fijms 20 04976%2Farticle Deploy%2FiDocument15 pagesHttps:%2Fmdpi Res.com%2Fd Attachment%2Fijms%2Fijms 20 04976%2Farticle Deploy%2FiRajan JattNo ratings yet
- Autism and Vaccination (Final)Document8 pagesAutism and Vaccination (Final)Rajan JattNo ratings yet
- ISBPlacements Report 2023Document24 pagesISBPlacements Report 2023Gaurav RawatNo ratings yet
- Drug InteractionsDocument13 pagesDrug InteractionsRajan JattNo ratings yet
- Company Profile PXCDocument6 pagesCompany Profile PXCRajan JattNo ratings yet
- Introduction Biochemical Engineering PT 530Document82 pagesIntroduction Biochemical Engineering PT 530Rajan JattNo ratings yet
- PhotoDocument1 pagePhotoRajan JattNo ratings yet
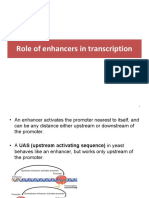
- 8 ROle of Enhancers in Trancription PDFDocument14 pages8 ROle of Enhancers in Trancription PDFRajan JattNo ratings yet
- Https:/twin Sci-Hub Se/5948//howlett2008Document15 pagesHttps:/twin Sci-Hub Se/5948//howlett2008Rajan JattNo ratings yet
- Pharma Earnings 2023 Q1Document20 pagesPharma Earnings 2023 Q1nimsi encisoNo ratings yet
- Aerosol Gpat NotesDocument9 pagesAerosol Gpat NotesRajan JattNo ratings yet
- Continuous CultureDocument33 pagesContinuous CultureRajan JattNo ratings yet
- Important QuestionsDocument11 pagesImportant QuestionsRajan JattNo ratings yet
- DTU Casebook 2021-22Document136 pagesDTU Casebook 2021-22Prashant MishraNo ratings yet
- Macro CalculatorDocument1 pageMacro CalculatorrutNo ratings yet
- Author: Phil Campbell: The Key To Longevity - Lengthen Your Telomeres With Sprint 8Document2 pagesAuthor: Phil Campbell: The Key To Longevity - Lengthen Your Telomeres With Sprint 8Pedro Alberto FontaniveNo ratings yet
- Risk Factors For Non-Communicable Diseases Among Adults of 25-65 Years at Kakamega County General Hospital, KenyaDocument9 pagesRisk Factors For Non-Communicable Diseases Among Adults of 25-65 Years at Kakamega County General Hospital, KenyaIJPHSNo ratings yet
- School Form 8 SF8 Learner Basic Health and Nutrition ReportDocument4 pagesSchool Form 8 SF8 Learner Basic Health and Nutrition Reportbeatrice kate m. lattao0% (1)
- CVD Risk Factors and PreventionDocument15 pagesCVD Risk Factors and PreventionKamalini Khanna 10-CNo ratings yet
- Sf8 Nutritional Status Grade 3 Del PilarDocument8 pagesSf8 Nutritional Status Grade 3 Del PilarYesha Lucas AcuñaNo ratings yet
- ANTI OBESITY CAMPDocument13 pagesANTI OBESITY CAMPgirishlambaNo ratings yet
- Nephrotic SyndromeDocument5 pagesNephrotic SyndromeMahmoud SalmanNo ratings yet
- Post Guidelines - June 16Document52 pagesPost Guidelines - June 16kevin clone1No ratings yet
- Fat PercentageDocument2 pagesFat PercentageGanesha Ram GNo ratings yet
- AlimiDocument10 pagesAlimiAhmad FarisNo ratings yet
- Sf8 Advisers Nutritional StatusDocument9 pagesSf8 Advisers Nutritional StatusKrizzia Bendiola100% (4)
- List Pasien USG TerbaruDocument4 pagesList Pasien USG Terbaruzayed norwantoNo ratings yet
- Relationship between foot mobilization exercises and wound healing rates in diabetic patientsDocument5 pagesRelationship between foot mobilization exercises and wound healing rates in diabetic patientsYenniNo ratings yet
- Screening and Management of DyslipidemiaDocument16 pagesScreening and Management of DyslipidemiaSakina GhaziNo ratings yet
- Approach to Dyslipidemia Based on 2015 CPGDocument26 pagesApproach to Dyslipidemia Based on 2015 CPGRenzy SalumbreNo ratings yet
- Analytical Exposition Text Kel 5Document11 pagesAnalytical Exposition Text Kel 5Oja JamaludinNo ratings yet
- DIAGNOSIS OverweightDocument7 pagesDIAGNOSIS OverweightWappy WepwepNo ratings yet
- Obesity Prevention and Control StrategiesDocument12 pagesObesity Prevention and Control StrategiesThianesh tyNo ratings yet
- Afzal Khan SahibDocument17 pagesAfzal Khan SahibhaidersarwarNo ratings yet
- Nilai NormalDocument1 pageNilai NormalAlbertson De'eNo ratings yet
- Body Goals Tracking SheetDocument4 pagesBody Goals Tracking Sheetska37927316No ratings yet
- R. K. Life Services Private Limited (Department of Laboratory Medicine)Document1 pageR. K. Life Services Private Limited (Department of Laboratory Medicine)Aniruddha ChatterjeeNo ratings yet
- Module 3 - Exercise PrescriptionDocument2 pagesModule 3 - Exercise PrescriptionNicole FinuliarNo ratings yet
- BNJ study finds progressive muscle relaxation reduces blood sugarDocument8 pagesBNJ study finds progressive muscle relaxation reduces blood sugarSemi MardiaNo ratings yet
- Nutritional Status Report of Dapdap Elementary High School: TotalDocument2 pagesNutritional Status Report of Dapdap Elementary High School: TotalAnalyn PenarandaNo ratings yet
- Mentoring Ukom Perawat: Meet 2Document19 pagesMentoring Ukom Perawat: Meet 2Khairina SiswantyNo ratings yet
- Metabolism Clinical and Experimental: Anatoli Petridou, Aikaterina Siopi, Vassilis MougiosDocument7 pagesMetabolism Clinical and Experimental: Anatoli Petridou, Aikaterina Siopi, Vassilis MougiosUjian LancarNo ratings yet
- Faktor-Faktor Yang Mempengaruhi Gangguan Tidur Pada Pasien Diabetes MelitusDocument6 pagesFaktor-Faktor Yang Mempengaruhi Gangguan Tidur Pada Pasien Diabetes MelitusImron BuhoriNo ratings yet
- Facility Risk Assessement Form 2016Document1 pageFacility Risk Assessement Form 2016kojiki67% (3)