You might also like
- Bake N Fill Cake PanDocument31 pagesBake N Fill Cake PanMarisaBerger75% (4)
- WSET L1 Award in Wines PresentationDocument49 pagesWSET L1 Award in Wines PresentationClaire DrinksNo ratings yet
- McCance Widdowsons Composition of Foods Integrated Dataset 2019Document3,691 pagesMcCance Widdowsons Composition of Foods Integrated Dataset 2019Nicoleta RotaruNo ratings yet
- Evolving Solutions For Automotive Industries: Fontus Water Pvt. LTDDocument2 pagesEvolving Solutions For Automotive Industries: Fontus Water Pvt. LTDKedar PatwardhanNo ratings yet
- Brochure InnoventurePlusDocument13 pagesBrochure InnoventurePlusabhishekdownloadNo ratings yet
- SE Annual Report 2020Document237 pagesSE Annual Report 2020Michael ScottNo ratings yet
- Operating Manual M1T - 371Document359 pagesOperating Manual M1T - 371Harshal ParikhNo ratings yet
- Prism Johnson FY20Document236 pagesPrism Johnson FY20PratikNo ratings yet
- Placing Boom SPB32 SPB35 Bro2018 - 0Document4 pagesPlacing Boom SPB32 SPB35 Bro2018 - 0Jonathan MendozaNo ratings yet
- Air Emissions 20 Indian CitiesDocument63 pagesAir Emissions 20 Indian CitiesBandish PatelNo ratings yet
- Delhi Metro Rail Network 2019Document1 pageDelhi Metro Rail Network 2019HIMAKSHI BHATIANo ratings yet
- Stationary Pump SP2509 SP2800 Bro2018Document4 pagesStationary Pump SP2509 SP2800 Bro2018p22ct004No ratings yet
- ASGI Price List 2019Document99 pagesASGI Price List 2019AMAZON SCIENTIFICNo ratings yet
- Line Pump 350 1000 1200 1400 1800 Bro2018 - 1Document4 pagesLine Pump 350 1000 1200 1400 1800 Bro2018 - 1Ravindra singh TanwarNo ratings yet
- Opportunities in Dairy Sector in IndiaDocument8 pagesOpportunities in Dairy Sector in IndiaPiyush GuptaNo ratings yet
- Digiscan SeriesDocument12 pagesDigiscan SeriesHugoNo ratings yet
- Two Wheeler Catalogue 2019 - FINAL PDFDocument24 pagesTwo Wheeler Catalogue 2019 - FINAL PDFGawade 414No ratings yet
- SJ - Holiday List 2017Document1 pageSJ - Holiday List 2017DIBINo ratings yet
- AIPMST Primary of Information BrochureDocument40 pagesAIPMST Primary of Information BrochureAIPMST PRIMARYNo ratings yet
- Supply & Demand Growth For Six Cities: RevparDocument2 pagesSupply & Demand Growth For Six Cities: RevparsanthoshNo ratings yet
- Awani Panwar FinalDocument11 pagesAwani Panwar FinalRohit PandeyNo ratings yet
- Super Six Product BrochureDocument2 pagesSuper Six Product BrochureravikumarrampurNo ratings yet
- MeaningDocument1 pageMeaningSuresh JadhavNo ratings yet
- Wurth Anchor Technology Catalogue 2019Document71 pagesWurth Anchor Technology Catalogue 2019nunnaraoNo ratings yet
- Gas Infrastructure Moi 17032021Document1 pageGas Infrastructure Moi 17032021Insta SriNo ratings yet
- CBT Test Center CitiesDocument1 pageCBT Test Center CitiesAnshul chauhanNo ratings yet
- The Lake BrochureDocument12 pagesThe Lake BrochureAtul DevNo ratings yet
- Particle - MDHMR - MDF Board: ToughDocument16 pagesParticle - MDHMR - MDF Board: ToughDeepu VijayanNo ratings yet
- BPCL Engineer ProfilesDocument14 pagesBPCL Engineer ProfilesPritesh KumarNo ratings yet
- Opportunities in Food Processing Sector in IndiaDocument24 pagesOpportunities in Food Processing Sector in IndiaPrakash KcNo ratings yet
- TH ABD AurangabadDocument1 pageTH ABD AurangabadLAXMAN HIWALE100% (1)
- Toll Rates From 1st April 2023 22x22 15.12.2022 For TOT Monthly PassDocument6 pagesToll Rates From 1st April 2023 22x22 15.12.2022 For TOT Monthly PassPradeep ReddyNo ratings yet
- Fully Automated ESR Analyzer: Service More Benefits Better ResultsDocument2 pagesFully Automated ESR Analyzer: Service More Benefits Better ResultsLokesh HoneyNo ratings yet
- Labsix Maptwo India Perceptualscaling 17875667Document1 pageLabsix Maptwo India Perceptualscaling 17875667api-530486411No ratings yet
- Toll Rates From 1st April 2023 22x22 15.12.2022 For TOT Toll RatesDocument6 pagesToll Rates From 1st April 2023 22x22 15.12.2022 For TOT Toll Ratesgoutam suryadeveraNo ratings yet
- Holiday Calendar - 2019Document1 pageHoliday Calendar - 2019Ravi RanjanNo ratings yet
- AIPMST SECONDARY Information BrochureDocument36 pagesAIPMST SECONDARY Information BrochureAIPMST SecondaryNo ratings yet
- TH MUS Kurla PDFDocument1 pageTH MUS Kurla PDFBilal KhanNo ratings yet
- World Bank ReportREPL PUBLIC WBG Blue Economy Report Bangladesh Nov2018Document96 pagesWorld Bank ReportREPL PUBLIC WBG Blue Economy Report Bangladesh Nov2018Shahriar KhandakerNo ratings yet
- Screw Air Compressor CatalogDocument6 pagesScrew Air Compressor CatalogRavi RathodNo ratings yet
- Shipping IndiaDocument2 pagesShipping IndiaSandipanBiswasNo ratings yet
- Directory Govt of OdishaDocument100 pagesDirectory Govt of OdishaBabulalSahu100% (1)
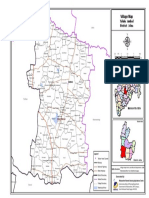
- Village Map: Taluka: Bid District: BidDocument1 pageVillage Map: Taluka: Bid District: BidAkshay NagarajaNo ratings yet
- SRF PresentationDocument28 pagesSRF PresentationSajeev KumarNo ratings yet
- Village Map: Taluka: Phaltan District: SataraDocument1 pageVillage Map: Taluka: Phaltan District: Satarasagar patoleNo ratings yet
- C 20220628 Parbhani DPR DrawingsDocument62 pagesC 20220628 Parbhani DPR DrawingsPrabaldeep GautamNo ratings yet
- Lvpei Ar 2015 16Document112 pagesLvpei Ar 2015 16Rational NationalNo ratings yet
- 0.28834300 1586976370 Hotspots-IndiaDocument1 page0.28834300 1586976370 Hotspots-IndiaMd FahimNo ratings yet
- Anantapur RegionDocument8 pagesAnantapur RegionNUTHI SIVA SANTHANNo ratings yet
- HitachiDocument8 pagesHitachiTan Sen WieNo ratings yet
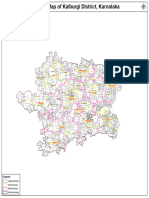
- District Kalburgi 1Document1 pageDistrict Kalburgi 1appaeducationtrust2015No ratings yet
- TH AMT Daryapur PDFDocument1 pageTH AMT Daryapur PDFpranav2304No ratings yet
- Village Map: Taluka: Ahmednagar District: AhmednagarDocument1 pageVillage Map: Taluka: Ahmednagar District: Ahmednagararunghandwal100% (1)
- 15674905675d6e0207e92d0TH STR KhandalaDocument1 page15674905675d6e0207e92d0TH STR KhandalaSachin LeleNo ratings yet
- Fruits & VegetablesDocument12 pagesFruits & VegetablesSurabhi SethiNo ratings yet
- About MaharashtraDocument20 pagesAbout MaharashtraPrasad RahateNo ratings yet
- AtpadiDocument1 pageAtpadiManisha PotdarNo ratings yet
- Aser 2005 ReportDocument150 pagesAser 2005 ReportBinoy AravindakshanNo ratings yet
- JFF Inma 2020Document15 pagesJFF Inma 2020Vibhor KwatraNo ratings yet
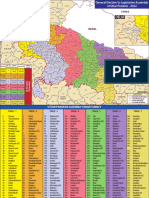
- Uttar Pradesh MapDocument2 pagesUttar Pradesh Mapdadan vishwakarmaNo ratings yet
- Relationship-Building: in Company Upper-Intermediate - Second Edition Answer Key: Unit 9Document5 pagesRelationship-Building: in Company Upper-Intermediate - Second Edition Answer Key: Unit 9AndriiNo ratings yet
- NPD - Oreo 12th Report - Final VersionDocument43 pagesNPD - Oreo 12th Report - Final VersionChat GptNo ratings yet
- Reviewer in Cookery 10Document93 pagesReviewer in Cookery 10Arneil RealizaNo ratings yet
- PURPLE CORN FLOUR STA MARIA THESIS OUTLINE Final Revised2Document43 pagesPURPLE CORN FLOUR STA MARIA THESIS OUTLINE Final Revised2Jain EpifanioNo ratings yet
- Crunchy Critters: From Icky To Yummy: NameDocument13 pagesCrunchy Critters: From Icky To Yummy: NameJKL PRO WRESTLINGNo ratings yet
- The Study of English Style: British English and American English WordsDocument12 pagesThe Study of English Style: British English and American English WordsRika MenkhinNo ratings yet
- Chocolate Order FormDocument9 pagesChocolate Order FormSamantha CottrellNo ratings yet
- Oreo in India and ChinaDocument5 pagesOreo in India and ChinaGAYATHRI S SNo ratings yet
- Pringles - Brand ManagementDocument14 pagesPringles - Brand ManagementShahzod KuchimovNo ratings yet
- Jiven HadloconDocument11 pagesJiven HadloconKim CarsonNo ratings yet
- Foods: Influence of Flour Particle Size Distribution On The Quality of Maize Gluten-Free CookiesDocument9 pagesFoods: Influence of Flour Particle Size Distribution On The Quality of Maize Gluten-Free CookiesAkmal AriffinNo ratings yet
- Soal Pat Sma Bahasa Inggris Kelas 11Document6 pagesSoal Pat Sma Bahasa Inggris Kelas 11Fathur RahmanNo ratings yet
- Copy33 SLG VegtablesDocument7 pagesCopy33 SLG VegtablesVasu SwarupNo ratings yet
- Buying Guide 2018: Appliances - EU - Cover - Indd 2 22/06/2017 12:35:39Document100 pagesBuying Guide 2018: Appliances - EU - Cover - Indd 2 22/06/2017 12:35:39Thomas PreeceNo ratings yet
- Technology and Livelihood Education G7-Bread and Pastry ProductionDocument3 pagesTechnology and Livelihood Education G7-Bread and Pastry ProductionJohn Harvey MagosNo ratings yet
- Melt-in-Mouth Butter Cookies (Egyptian Ghorayebah) - The Mediterranean DishDocument2 pagesMelt-in-Mouth Butter Cookies (Egyptian Ghorayebah) - The Mediterranean DishCarmen NelNo ratings yet
- Department of Education: Republic of The PhilippinesDocument24 pagesDepartment of Education: Republic of The PhilippinesFroilan MatutinoNo ratings yet
- Sizzante Sizzlers MenuDocument8 pagesSizzante Sizzlers Menuminesh desaiNo ratings yet
- Teks ProduceDocument4 pagesTeks ProduceReza KonioNo ratings yet
- GrammarDocument2 pagesGrammarMonicaNo ratings yet
- Quiz#1 TEST 1. (10 Points) (2 Points Each)Document2 pagesQuiz#1 TEST 1. (10 Points) (2 Points Each)Krizza Mae Yambao TayagNo ratings yet
- TLE Cookery10 Q4 W3 V4Document7 pagesTLE Cookery10 Q4 W3 V4Maria Rose Tariga Aquino100% (2)
- De Thi Hoc Ky 1 Mon Tieng Anh Lop 2 Co Dap An 1Document10 pagesDe Thi Hoc Ky 1 Mon Tieng Anh Lop 2 Co Dap An 1Lục ThủyNo ratings yet
- Faux's Ironman Barrows Gloves List - Quest ListDocument3 pagesFaux's Ironman Barrows Gloves List - Quest Listerick peñaNo ratings yet
- A Level Pin Grammar Pack Student'sDocument16 pagesA Level Pin Grammar Pack Student'sUmut TurNo ratings yet
- File Test 9Document7 pagesFile Test 9fortiz241079No ratings yet
- Plurals - Countable / Uncountable Nouns Test A1 - A2 Grammar ExercisesDocument4 pagesPlurals - Countable / Uncountable Nouns Test A1 - A2 Grammar ExercisesNurul FathihahNo ratings yet