You might also like
- MEB001 FundsAtWork Umbrella Funds Withdrawal FormDocument5 pagesMEB001 FundsAtWork Umbrella Funds Withdrawal FormdlndlaminiNo ratings yet
- Retirement Notification FormDocument2 pagesRetirement Notification FormAbongile PhinyanaNo ratings yet
- Zamara Notification of Exit-DC or Provident FormDocument3 pagesZamara Notification of Exit-DC or Provident Formwaruu769No ratings yet
- 12benefit Payment FormDocument5 pages12benefit Payment Formemmanuelkorli1No ratings yet
- Application Form Enwealth New AccountDocument2 pagesApplication Form Enwealth New AccounticttumainiNo ratings yet
- Staff Retirement BenefitsDocument2 pagesStaff Retirement BenefitsEthan LynnNo ratings yet
- C6575 OMC ISASA Retirement Benefit Claim Form WR 1Document4 pagesC6575 OMC ISASA Retirement Benefit Claim Form WR 1Lungisani MtshaliNo ratings yet
- Fixed Deposit FormDocument2 pagesFixed Deposit FormNikita JainNo ratings yet
- Hekima Plan Application Form-EDocument4 pagesHekima Plan Application Form-ExeniaNo ratings yet
- Intimation of Retirement/Death/Leaving Service: Sample FormDocument9 pagesIntimation of Retirement/Death/Leaving Service: Sample FormDeliver rNo ratings yet
- Partial Withdrawal Form1Document2 pagesPartial Withdrawal Form1KANGSA banikNo ratings yet
- Pre-Mature Exit Form Jan 19Document2 pagesPre-Mature Exit Form Jan 19antriksh82No ratings yet
- SBI Life - Swarna Jeevan Plus - V03 - Proposal FormDocument4 pagesSBI Life - Swarna Jeevan Plus - V03 - Proposal FormPrudvi ReddyNo ratings yet
- Partial Withdrawal Form For Tier I Account Under NPSDocument3 pagesPartial Withdrawal Form For Tier I Account Under NPSSanthosh ShivamNo ratings yet
- IP Enrollment FormDocument2 pagesIP Enrollment FormSrigandh's WealthNo ratings yet
- Maturity-Survival Claim FormDocument3 pagesMaturity-Survival Claim FormAccuntsofficer Legal100% (1)
- Surrender FormDocument2 pagesSurrender FormpghoshNo ratings yet
- Absa Consultants and Actuaries Afrimat Pension Fund (Withdrawal) - 101456903 PDFDocument3 pagesAbsa Consultants and Actuaries Afrimat Pension Fund (Withdrawal) - 101456903 PDFAlvin JantjiesNo ratings yet
- Bosa Loan FormDocument4 pagesBosa Loan FormIsaac OkotNo ratings yet
- UntitledDocument8 pagesUntitledGurpreet SinghNo ratings yet
- Standard Withdrawal FormDocument8 pagesStandard Withdrawal FormAntónio MoreiraNo ratings yet
- Loan Application Form 1. Applicant'S Personal InformationDocument2 pagesLoan Application Form 1. Applicant'S Personal InformationWingadianLeviOsa100% (5)
- Bosa Loan Application FormDocument2 pagesBosa Loan Application Formal lakwena100% (1)
- Form 601-Partial Withdrawal Under NPSDocument3 pagesForm 601-Partial Withdrawal Under NPSRanga Nayak PaltyaNo ratings yet
- Myplan 2018 - EnglishDocument1 pageMyplan 2018 - EnglishkleansoulNo ratings yet
- PF ClaimDocument4 pagesPF ClaimAmarjeet TakNo ratings yet
- Interben Trustees Limited Withdrawal FormDocument8 pagesInterben Trustees Limited Withdrawal FormAmenAllah DghimNo ratings yet
- Sampoorn Suraksha - Master Proposal Form - NEE - 22422Document4 pagesSampoorn Suraksha - Master Proposal Form - NEE - 22422ANIL TIWARINo ratings yet
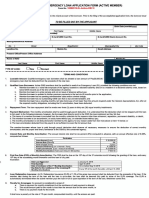
- Emergency Loan Application Form (Active Member) : Last Name Middle NameDocument2 pagesEmergency Loan Application Form (Active Member) : Last Name Middle NameGian Paula MonghitNo ratings yet
- Emergency Loan Application Form (Active Member) : Last Name Middle NameDocument2 pagesEmergency Loan Application Form (Active Member) : Last Name Middle NameKarena WahimanNo ratings yet
- 20200403-Forms-EML Active Fillable PDFDocument2 pages20200403-Forms-EML Active Fillable PDFKarena WahimanNo ratings yet
- 20200403-Forms-EML Active Fillable PDFDocument2 pages20200403-Forms-EML Active Fillable PDFBusyMae CabadonNo ratings yet
- 20200403-Forms-EML Active FillableDocument2 pages20200403-Forms-EML Active FillableChesca Angel ReyesNo ratings yet
- Emergency Loan Application Form (Active Member) : Last Name Middle NameDocument2 pagesEmergency Loan Application Form (Active Member) : Last Name Middle NameDeese Marie ZabalaNo ratings yet
- Withdrawal Claim FormDocument5 pagesWithdrawal Claim FormLungisani MtshaliNo ratings yet
- CIBI Report - Form BDocument4 pagesCIBI Report - Form BJose Rico ColigadoNo ratings yet
- New IT Declaration FormDocument2 pagesNew IT Declaration FormMahakaal Digital PointNo ratings yet
- Emergency Loan Application Form (Active Member) : Last Name Middle NameDocument2 pagesEmergency Loan Application Form (Active Member) : Last Name Middle NamePhebe Zhie Zhia CampeñaNo ratings yet
- ELIB Group Claims Claimant Statement FormDocument2 pagesELIB Group Claims Claimant Statement FormPnk Telok KemangNo ratings yet
- Partial Withdrawal Form - 601Document3 pagesPartial Withdrawal Form - 601mahenderNo ratings yet
- Service-Request-Form DBS BankDocument3 pagesService-Request-Form DBS BanketishreddyNo ratings yet
- LTA Reimbursement Claim Form For 2020-2021: Company NameDocument3 pagesLTA Reimbursement Claim Form For 2020-2021: Company NameAnish JainNo ratings yet
- Provident New Edited 2021Document2 pagesProvident New Edited 2021Edison Castillo GutierrezNo ratings yet
- Sav3062 4Document6 pagesSav3062 4MichaelNo ratings yet
- Annexure - Common Loan Application Form With Formats I, II and III-EnglishDocument12 pagesAnnexure - Common Loan Application Form With Formats I, II and III-EnglishThe LoanWalaNo ratings yet
- MifDocument2 pagesMifpatilshashiNo ratings yet
- Dpban1906190107341 Ad Insur PRSPL PG1 Nitesh Soni 19810325Document1 pageDpban1906190107341 Ad Insur PRSPL PG1 Nitesh Soni 19810325Digi CreditNo ratings yet
- Premature Withdrawal Form - 102Document8 pagesPremature Withdrawal Form - 102sher singhNo ratings yet
- Group Hospital and Surgical Claim FormDocument4 pagesGroup Hospital and Surgical Claim FormYiki TanNo ratings yet
- Senior Citizens and Disabled Persons Rate Rebate Application Form EnglishDocument2 pagesSenior Citizens and Disabled Persons Rate Rebate Application Form EnglishGiovanni RossiNo ratings yet
- SBI Life - Assignment FormDocument2 pagesSBI Life - Assignment FormAgrawal DeekshaNo ratings yet
- New Hire TemplateDocument1 pageNew Hire TemplateSaurabh SinghNo ratings yet
- GPF FinaDocument8 pagesGPF Finateja ptoNo ratings yet
- Sav 5336Document9 pagesSav 5336Michael100% (1)
- HR 107 A Retirement Form PDFDocument6 pagesHR 107 A Retirement Form PDFLexNo ratings yet
- NEW HSBC Loan FormDocument4 pagesNEW HSBC Loan FormEdrick EstradaNo ratings yet
- SBP Prescribed Application Form For Governments Profit Subsidy Facility (English)Document6 pagesSBP Prescribed Application Form For Governments Profit Subsidy Facility (English)muhammadTzNo ratings yet
- PAD DocumentDocument2 pagesPAD DocumentBhupender Kaur MadhokNo ratings yet
- TermSukuk App Form Individual E Mrs ANISHADocument2 pagesTermSukuk App Form Individual E Mrs ANISHAsunij.chackoNo ratings yet
- How To File Your Own Bankruptcy: The Step-by-Step Handbook to Filing Your Own Bankruptcy PetitionFrom EverandHow To File Your Own Bankruptcy: The Step-by-Step Handbook to Filing Your Own Bankruptcy PetitionNo ratings yet
- African Spa CollectionDocument1 pageAfrican Spa CollectionLungisani MtshaliNo ratings yet
- Advert Traffic Officer 20 March 2023Document2 pagesAdvert Traffic Officer 20 March 2023Lungisani MtshaliNo ratings yet
- Withdrawal Claim FormDocument5 pagesWithdrawal Claim FormLungisani MtshaliNo ratings yet
- Mtshali : Surname Initials Identification Type Identification NumberDocument1 pageMtshali : Surname Initials Identification Type Identification NumberLungisani MtshaliNo ratings yet
- Practice SumsDocument9 pagesPractice SumsThanuja BhaskarNo ratings yet
- Homework 7 - Leases (Lessor - S Books)Document1 pageHomework 7 - Leases (Lessor - S Books)alvarezxpatriciaNo ratings yet
- AdvanceReceipt2021 05 02 18 22 31Document2 pagesAdvanceReceipt2021 05 02 18 22 31ShubhamNo ratings yet
- Investment Analysis and Portfolio ManagementDocument26 pagesInvestment Analysis and Portfolio Managementkumar sahityaNo ratings yet
- Ch13-Cash Flow STMDocument44 pagesCh13-Cash Flow STMAnonymous zXWxWmgZENo ratings yet
- Impact of Digitalization On Indian Rural Banking Customer: With Reference To Payment SystemsDocument11 pagesImpact of Digitalization On Indian Rural Banking Customer: With Reference To Payment SystemsNikhil RajNo ratings yet
- Chapter 8 Debentures and ChargesDocument2 pagesChapter 8 Debentures and ChargesNahar Sabirah100% (1)
- TC Visa CashbackDocument10 pagesTC Visa Cashbackioi123No ratings yet
- IFS - Chapter 4Document28 pagesIFS - Chapter 4riashahNo ratings yet
- 3 Money CreationDocument10 pages3 Money CreationEleine AlvarezNo ratings yet
- 7 Different Types of Journal in Accounting With ExamplesDocument8 pages7 Different Types of Journal in Accounting With ExamplesHaroon YousafNo ratings yet
- Credit Default Swaps (CDS) and Financial Guarantee (FG) InsuranceDocument33 pagesCredit Default Swaps (CDS) and Financial Guarantee (FG) InsuranceGeorge Lekatis100% (1)
- MathDocument3 pagesMathMaRia CaroLina PollarcaNo ratings yet
- Your Adv Safebalance Banking: Account SummaryDocument6 pagesYour Adv Safebalance Banking: Account SummaryJeremy White100% (1)
- Acccob2 Quiz 2 1203 Acccob2 k44 Financial AccountingDocument18 pagesAcccob2 Quiz 2 1203 Acccob2 k44 Financial AccountingChelcy Mari GugolNo ratings yet
- Credit and Lending Policies in The PhilippinesDocument2 pagesCredit and Lending Policies in The Philippinesmari bellogaNo ratings yet
- Chapter 11 Capital N SurplusDocument12 pagesChapter 11 Capital N SurplusCiciNo ratings yet
- Chapter 1. Overview of International Settlement1.Document4 pagesChapter 1. Overview of International Settlement1.BipNo ratings yet
- Summary PBI Regulation in Regard To The Reporting of Offshore BorrowingDocument3 pagesSummary PBI Regulation in Regard To The Reporting of Offshore BorrowingAditya NuramaliaNo ratings yet
- Kendriya Vidyalaya No.1 Kunjaban, Agartala Tripura: Submitted By: Aboya DebbarmaDocument12 pagesKendriya Vidyalaya No.1 Kunjaban, Agartala Tripura: Submitted By: Aboya Debbarmaakash debbarmaNo ratings yet
- 01 CashandCashEquivalentsNotesDocument7 pages01 CashandCashEquivalentsNotesVeroNo ratings yet
- Sec Form LcfsDocument15 pagesSec Form LcfsMeanne Waga Salazar100% (1)
- Corporate FinanceDocument20 pagesCorporate FinanceChelseyNo ratings yet
- Financial Literacy PowerpointDocument17 pagesFinancial Literacy Powerpointapi-40190669833% (3)
- Lobj18 0007008 Question Bank of AccountingDocument223 pagesLobj18 0007008 Question Bank of AccountingMỹ NhiNo ratings yet
- Date Issued: 05.19.2006 Number: 0530 Circular No. 530 Series of 2006Document1 pageDate Issued: 05.19.2006 Number: 0530 Circular No. 530 Series of 2006Jesse Myl MarciaNo ratings yet
- Ratio Analysis Cheat SheetDocument1 pageRatio Analysis Cheat SheetAtharva Gore100% (1)
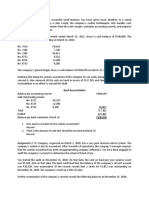
- Assignment 1. Your Client, A Successful Small Business, Has Never Given Much Attention To A SoundDocument6 pagesAssignment 1. Your Client, A Successful Small Business, Has Never Given Much Attention To A SoundThricia Mae Lorenzo IgnacioNo ratings yet
- Bank Statement GeneratorDocument1 pageBank Statement GeneratorLeslie AtehNo ratings yet
- Operations Management Operations Management: How This Book Is OrganizedDocument13 pagesOperations Management Operations Management: How This Book Is OrganizedNguyên BùiNo ratings yet