You might also like
- Disorders of the Patellofemoral Joint: Diagnosis and ManagementFrom EverandDisorders of the Patellofemoral Joint: Diagnosis and ManagementNo ratings yet
- Fractures of the Wrist: A Clinical CasebookFrom EverandFractures of the Wrist: A Clinical CasebookNirmal C. TejwaniNo ratings yet
- 10 1016@j Jse 2019 10 013Document12 pages10 1016@j Jse 2019 10 013Gustavo BECERRA PERDOMONo ratings yet
- Radiofrequency Microtenotomy Relieves Achilles TendinopathyDocument4 pagesRadiofrequency Microtenotomy Relieves Achilles TendinopathyPe T. ErNo ratings yet
- Colin 2014Document6 pagesColin 2014Negru TeodorNo ratings yet
- Functiuonal Out5come After Sugical Tratment of Ankle Fracture Using Baird Jackon ScoreDocument4 pagesFunctiuonal Out5come After Sugical Tratment of Ankle Fracture Using Baird Jackon ScoreAxell C MtzNo ratings yet
- Chen Et Al Large Review of AvulsionDocument6 pagesChen Et Al Large Review of Avulsionm lNo ratings yet
- Semiconstrained Total Elbow Arthroplasty-1Document6 pagesSemiconstrained Total Elbow Arthroplasty-1Ευαγγελια ΚιμπαρηNo ratings yet
- Surgical Outcomes After Traumatic Open Knee Dislocation: Ó Springer-Verlag 2009Document6 pagesSurgical Outcomes After Traumatic Open Knee Dislocation: Ó Springer-Verlag 2009agus sukarnaNo ratings yet
- Surgical Treatment of Chronic Elbow Dislocation Allowing For Early Range of Motion: Operative Technique and Clinical ResultsDocument8 pagesSurgical Treatment of Chronic Elbow Dislocation Allowing For Early Range of Motion: Operative Technique and Clinical ResultsLuis Carlos HernandezNo ratings yet
- Dloen-Treatment Diaphyseal Non Union Unal RadiusDocument7 pagesDloen-Treatment Diaphyseal Non Union Unal RadiusAngélica RamírezNo ratings yet
- Degenerative Meniscal Tears (Graaf Et Al 2019)Document7 pagesDegenerative Meniscal Tears (Graaf Et Al 2019)nsboyadzhievNo ratings yet
- 10 1016@j Arthro 2006 07 006Document8 pages10 1016@j Arthro 2006 07 006YoshitaNo ratings yet
- HTTPS://WWW Mendeley Com/reference-Manager/readerDocument6 pagesHTTPS://WWW Mendeley Com/reference-Manager/readerIJAR JOURNALNo ratings yet
- Analysis of Surgical Management of Proximal Humeral FracturesDocument5 pagesAnalysis of Surgical Management of Proximal Humeral FracturesRhizka djitmauNo ratings yet
- HNPDocument10 pagesHNPNico LieNo ratings yet
- Treatment of Distal Humerus FracturedDocument10 pagesTreatment of Distal Humerus Fracturedauliya ningsihNo ratings yet
- Elmoumni2012 Long-Term Functional Outcome Following Intramedullary Nailing ofDocument5 pagesElmoumni2012 Long-Term Functional Outcome Following Intramedullary Nailing ofJian Wei LowNo ratings yet
- Review of Intramedullary Interlocked Nailing in Closed & Grade I Open Tibial FracturesDocument4 pagesReview of Intramedullary Interlocked Nailing in Closed & Grade I Open Tibial FracturesInternational Organization of Scientific Research (IOSR)No ratings yet
- Functional Treatment Versus Plaster For Simple Elbow Dislocations (Funcsie) : A Randomized TrialDocument7 pagesFunctional Treatment Versus Plaster For Simple Elbow Dislocations (Funcsie) : A Randomized TrialTekhaDwiNo ratings yet
- Bernarddedompsure 2010Document8 pagesBernarddedompsure 2010liearenNo ratings yet
- Primary Total Shoulder Arthroplasty Performed Entirely Thru The Rotator Interval - Technique and Minimum Two-Year OutcomesDocument10 pagesPrimary Total Shoulder Arthroplasty Performed Entirely Thru The Rotator Interval - Technique and Minimum Two-Year OutcomesmotohumeresNo ratings yet
- 2023 JOT Radiological and Long Term Functional Outcomes of Displaced Distal Clavicle FracturesDocument7 pages2023 JOT Radiological and Long Term Functional Outcomes of Displaced Distal Clavicle FracturesjcmarecauxlNo ratings yet
- External Rotation Method Reduces Anterior Shoulder DislocationsDocument4 pagesExternal Rotation Method Reduces Anterior Shoulder DislocationsBasmah Al-DhafarNo ratings yet
- Tur CicaDocument8 pagesTur CicazubayetarkoNo ratings yet
- Percutaneous Endoscopic Decompression Via Transforaminal Approach For Lumbar Lateral Recess Stenosis in Geriatric PatientsDocument7 pagesPercutaneous Endoscopic Decompression Via Transforaminal Approach For Lumbar Lateral Recess Stenosis in Geriatric PatientsAmina GoharyNo ratings yet
- A Long Term Follow Up Study of Total Meniscectomy.30Document5 pagesA Long Term Follow Up Study of Total Meniscectomy.30Anshal GuptaNo ratings yet
- Artrosis glenohumeral despues de artroscopia Bankart repair a long-term follow-up of 13 yearsDocument6 pagesArtrosis glenohumeral despues de artroscopia Bankart repair a long-term follow-up of 13 yearsmarcelogascon.oNo ratings yet
- Accepted Manuscript: 10.1016/j.jcms.2017.12.013Document16 pagesAccepted Manuscript: 10.1016/j.jcms.2017.12.013stoia_sebiNo ratings yet
- Operative Treatment of Terrible Triad of TheDocument8 pagesOperative Treatment of Terrible Triad of TheAndrea OsborneNo ratings yet
- Obesity PDFDocument21 pagesObesity PDFIka Elwinda DariseNo ratings yet
- Calcanectomy For OsteomyelitisDocument7 pagesCalcanectomy For OsteomyelitisCleff FlowersNo ratings yet
- The Functional Outcome of Blow-Out Fractures Managed Surgically and Conservatively: Our Experience in 100 PatientsDocument5 pagesThe Functional Outcome of Blow-Out Fractures Managed Surgically and Conservatively: Our Experience in 100 Patientsstoia_sebiNo ratings yet
- mcrae2015Document8 pagesmcrae2015Ananth BalakrishnanNo ratings yet
- El BatrawypaperDocument7 pagesEl BatrawypaperabdallahalshallNo ratings yet
- Functional Outcome of Operative Management of Humeral Shaft FracturesDocument5 pagesFunctional Outcome of Operative Management of Humeral Shaft FracturesDr JunaidNo ratings yet
- Age-Based Outcomes of Cheilectomy For The Treatment of Hallux RigidusDocument6 pagesAge-Based Outcomes of Cheilectomy For The Treatment of Hallux RigidusmilenabogojevskaNo ratings yet
- Endoscopic Resection of Symptomatic Osteochondroma of The Distal FemurDocument4 pagesEndoscopic Resection of Symptomatic Osteochondroma of The Distal FemurAlex CirlanNo ratings yet
- Transforaminal Lumbar Interbody Fusion (TLIF) : Assessment of Clinical and Radiological OutcomeDocument6 pagesTransforaminal Lumbar Interbody Fusion (TLIF) : Assessment of Clinical and Radiological OutcomeJosh JoshiNo ratings yet
- AJPMR - Prosthetic Rehabilitation After Hip Disarticulation or Hemipelvectomy PDFDocument6 pagesAJPMR - Prosthetic Rehabilitation After Hip Disarticulation or Hemipelvectomy PDFSergio Navarrete VidalNo ratings yet
- Clinical and Radiological Outcomes of Osteoarth 2019 Orthopaedics TraumatoDocument6 pagesClinical and Radiological Outcomes of Osteoarth 2019 Orthopaedics TraumatodrelvNo ratings yet
- Two-Stage Bone Lengthening With Reuse of A Single Intramedullary Telescopic Nail in Patients With AchondroplasiaDocument7 pagesTwo-Stage Bone Lengthening With Reuse of A Single Intramedullary Telescopic Nail in Patients With AchondroplasiaLizza Mora RNo ratings yet
- 1-s2.0-S0901502716300728-mainDocument4 pages1-s2.0-S0901502716300728-mainCaio GonçalvesNo ratings yet
- Ganesh 2011Document5 pagesGanesh 2011Giang Nguyễn NgânNo ratings yet
- 268 2011 Article 1088 PDFDocument6 pages268 2011 Article 1088 PDFIoel Tovar TrovaNo ratings yet
- Modified 2 CM Super Single Port vs. The Traditional 3 CM Single Port For Video Assisted Thoracoscopic Surgery LobectomyDocument8 pagesModified 2 CM Super Single Port vs. The Traditional 3 CM Single Port For Video Assisted Thoracoscopic Surgery LobectomyAlin Ionut BurlacuNo ratings yet
- Jurnal Eng 5Document6 pagesJurnal Eng 5Hendra SaputraNo ratings yet
- Wolff 2019Document7 pagesWolff 2019Christopher BermeoNo ratings yet
- Alesina et al., 2021Document9 pagesAlesina et al., 2021NyomantrianaNo ratings yet
- 223654-Article Text-546414-1-10-20220403Document6 pages223654-Article Text-546414-1-10-20220403Christopher Freddy Bermeo RiveraNo ratings yet
- 08 Subasi NecmiogluDocument7 pages08 Subasi Necmiogludoos1No ratings yet
- SEGUIMIENTO A 5 AÑOS PTGH REVERSADocument7 pagesSEGUIMIENTO A 5 AÑOS PTGH REVERSAmarcelogascon.oNo ratings yet
- Nejm Achiles Surgery Vs NonDocument12 pagesNejm Achiles Surgery Vs NonShandy MahardikaNo ratings yet
- Stadhouder PDFDocument7 pagesStadhouder PDFPramod N KNo ratings yet
- Acta Orthopaedica Et Traumatologica Turcica: C. Sahin, Y. Oc, N. Ediz, M. Alt Inay, A.H. BayrakDocument6 pagesActa Orthopaedica Et Traumatologica Turcica: C. Sahin, Y. Oc, N. Ediz, M. Alt Inay, A.H. BayrakPoji RazaliNo ratings yet
- FandAC - 2017 - Hamid - Chronic Rupture of Peroneal TendonsDocument8 pagesFandAC - 2017 - Hamid - Chronic Rupture of Peroneal TendonsJacob DoughertyNo ratings yet
- FxAcromion PDFDocument8 pagesFxAcromion PDFPenélope CrespoNo ratings yet
- Results of Surgical TreatmentDocument4 pagesResults of Surgical TreatmentChristine Yohana SianturiNo ratings yet
- Surgery Corec Revizuit 1tDocument28 pagesSurgery Corec Revizuit 1tRoxana Alexandra BogosNo ratings yet
- A Clinical Prediction Rule For Meniscal Tears in Primary CareDocument7 pagesA Clinical Prediction Rule For Meniscal Tears in Primary CareDeivisonNo ratings yet
- List of Visiting DoctorDocument3 pagesList of Visiting Doctordulal pramanickNo ratings yet
- Glucosamine PDFDocument6 pagesGlucosamine PDFChrist FarandyNo ratings yet
- Sylvia PlathDocument12 pagesSylvia Plathapi-534201968No ratings yet
- Case Study Attendance Score DisputeDocument3 pagesCase Study Attendance Score DisputeSyed Aamir Ahmed0% (2)
- Introduction To Architectural ProgrammingDocument34 pagesIntroduction To Architectural ProgrammingbalaNo ratings yet
- Industrial Security Management SyllabusDocument7 pagesIndustrial Security Management SyllabusZefren Botilla100% (2)
- Professional Adjustment GuideDocument57 pagesProfessional Adjustment Guidemark OrpillaNo ratings yet
- Board and Reviewer Assignments for Convened IRB ReviewDocument5 pagesBoard and Reviewer Assignments for Convened IRB ReviewMuhammad Zaryab KhanNo ratings yet
- NEW - Hormone Balancing DrinkDocument9 pagesNEW - Hormone Balancing DrinkTAE'S POTATONo ratings yet
- Approach To Child With Headache: Dr. Vijaya Kumar Chikanbanjar 2nd Year Resident Department of PediatricsDocument49 pagesApproach To Child With Headache: Dr. Vijaya Kumar Chikanbanjar 2nd Year Resident Department of Pediatricsar bindraNo ratings yet
- Example For Attendance Rate CalculationDocument1 pageExample For Attendance Rate CalculationSuresh kumar100% (1)
- Effects of A Capacitive-Resistive Electric Transfer Therapy OnDocument8 pagesEffects of A Capacitive-Resistive Electric Transfer Therapy OnAnna Lygia LunardiNo ratings yet
- Nursing Health AssessmentDocument19 pagesNursing Health AssessmentAHMAD HASIMI BIN ABDUL GHANI STUDENTNo ratings yet
- SEMI FINAL FINAL NCM 113 NotesDocument1 pageSEMI FINAL FINAL NCM 113 Notesmblanco.dchNo ratings yet
- Employees' Financial Literacy, Behavior, Stress and WellnessDocument12 pagesEmployees' Financial Literacy, Behavior, Stress and WellnessYong Leigh LocusamNo ratings yet
- Nursing Leadership Roles ResponsibilitiesDocument2 pagesNursing Leadership Roles ResponsibilitiesDan Dan ManaoisNo ratings yet
- ACUTE KIDNEY INJURY SIGNS, SYMPTOMS, AND CAUSESDocument10 pagesACUTE KIDNEY INJURY SIGNS, SYMPTOMS, AND CAUSESYanti TandjungNo ratings yet
- Legalize ItDocument2 pagesLegalize Itaisar aisarNo ratings yet
- List of Allianz Efu Network (Panel) Hospitals: Hospital Name Address Telephone # KarachiDocument6 pagesList of Allianz Efu Network (Panel) Hospitals: Hospital Name Address Telephone # KarachiFaizan BasitNo ratings yet
- SRNT 2015 Abstracts WEBDocument362 pagesSRNT 2015 Abstracts WEBSatya Ashok KumarNo ratings yet
- Explaining Medication To Patients: Ni Kadek Ary Susandi, S.S., M.App - LingDocument11 pagesExplaining Medication To Patients: Ni Kadek Ary Susandi, S.S., M.App - LingmirahayuuNo ratings yet
- Measuring Hierarchy of Basic Needs Among Adults: Yadolla Saeednia, Mariani MD NORDocument4 pagesMeasuring Hierarchy of Basic Needs Among Adults: Yadolla Saeednia, Mariani MD NORRodrigo FerreiraNo ratings yet
- Noncompliance Unilateral Maxillary Molar DistalizationDocument6 pagesNoncompliance Unilateral Maxillary Molar Distalizationaa bbNo ratings yet
- 1st Summative Test in in English 6 Q1 Answer KeyDocument4 pages1st Summative Test in in English 6 Q1 Answer KeyGessle GamirNo ratings yet
- Hospital Business ModelsDocument8 pagesHospital Business ModelsPOLOKO MHUSIWANo ratings yet
- ProteinDocument89 pagesProteinAki OtaniNo ratings yet
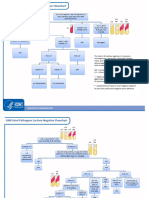
- GNR Stool Pathogens Lactose Negative FlowchartDocument2 pagesGNR Stool Pathogens Lactose Negative FlowchartKeithNo ratings yet
- Study Skills GroupDocument25 pagesStudy Skills Groupapi-654376760No ratings yet
- De-Escalation - Aggression Management TechniquesDocument14 pagesDe-Escalation - Aggression Management Techniquesparis emmaNo ratings yet
- Lecture PATHFT2Document7 pagesLecture PATHFT2Gniese Stephanie Gallema AlsayNo ratings yet