You might also like
- Consent Teeth WhiteningDocument1 pageConsent Teeth WhiteningDOCTOR100% (1)
- ACLS Pre Test AnswersDocument10 pagesACLS Pre Test AnswersAirene SibleNo ratings yet
- Nursing Care Plan For SarsDocument5 pagesNursing Care Plan For SarsRhea Princess Tadeo88% (8)
- Education Brochure Autosaved 1Document2 pagesEducation Brochure Autosaved 1api-268623902100% (2)
- English For Doctors Customer BookletDocument23 pagesEnglish For Doctors Customer BookletFrugeo GRI Limited70% (10)
- VAN HILTEN, Meindert Onno - Covid-19 and NCDs - PUBLISHED (23 March 2020) PDFDocument2 pagesVAN HILTEN, Meindert Onno - Covid-19 and NCDs - PUBLISHED (23 March 2020) PDFPriyanka BindaNo ratings yet
- COVID19Document79 pagesCOVID19Mohamad El SharNo ratings yet
- Home Care For Patients With COVID-19 Presenting With Mild Symptoms and Management of Their ContactsDocument5 pagesHome Care For Patients With COVID-19 Presenting With Mild Symptoms and Management of Their ContactsNur MaliaNo ratings yet
- Archivo Covid 2Document4 pagesArchivo Covid 2Jorge Ferney Pineda BertelNo ratings yet
- CCRH - Revised Guidelines For Homeopathy Practitioners For Home Isolated COVID 19 Patient-FDocument4 pagesCCRH - Revised Guidelines For Homeopathy Practitioners For Home Isolated COVID 19 Patient-FTisil KodithottamNo ratings yet
- Clinical Management Protocol PDFDocument7 pagesClinical Management Protocol PDFAJEET KUMAR PANDEYNo ratings yet
- Novel Coronavirus Update A Physician Perspective: Presented by Dr. Mohammad Amzarul M.D. (Medicine)Document35 pagesNovel Coronavirus Update A Physician Perspective: Presented by Dr. Mohammad Amzarul M.D. (Medicine)dramzarulNo ratings yet
- Elsevier Order Sets: COVID-19 - Ward (2.2)Document36 pagesElsevier Order Sets: COVID-19 - Ward (2.2)Bryam PradoNo ratings yet
- Respiratory Syndrome Coronavirus 2 (Sars-Cov-2) That Can Cause Symptoms From Common Cold ToDocument4 pagesRespiratory Syndrome Coronavirus 2 (Sars-Cov-2) That Can Cause Symptoms From Common Cold ToARISNo ratings yet
- 1.nurse Preparedness Training Against 3rd Wave of CovidDocument52 pages1.nurse Preparedness Training Against 3rd Wave of CovidyeshumasihNo ratings yet
- Presentasi Dr. Basuki Rachmad, Sp. An. KICDocument39 pagesPresentasi Dr. Basuki Rachmad, Sp. An. KICFirdaus FamilyNo ratings yet
- Presentasi Dr. Basuki Rachmad, Sp. An. KICDocument39 pagesPresentasi Dr. Basuki Rachmad, Sp. An. KICinstalasi kamar bedah RSMINo ratings yet
- Edited COVID19 HANDOUT Requina SindiongDocument5 pagesEdited COVID19 HANDOUT Requina SindiongJannen CasasNo ratings yet
- Elsevier Order Sets: COVID-19 - Ward (3.0)Document36 pagesElsevier Order Sets: COVID-19 - Ward (3.0)LyleChristineNo ratings yet
- WHO Covid19 HomeCare 2020.3 EngDocument4 pagesWHO Covid19 HomeCare 2020.3 EngReggie CastroNo ratings yet
- Disease Outbreak Case StudyDocument8 pagesDisease Outbreak Case StudyFoxtrot NursingNo ratings yet
- Neumonia y Bronquiolitis 22Document14 pagesNeumonia y Bronquiolitis 22Rafael Florez HernandezNo ratings yet
- Covid NCPDocument4 pagesCovid NCPGabrelle AbalosNo ratings yet
- Nursing and Covid-19Document12 pagesNursing and Covid-19AlNo ratings yet
- COVID-19 Critical Care: TerminologyDocument15 pagesCOVID-19 Critical Care: TerminologyLuis TKDNo ratings yet
- Bronchiolitis: Dr. Mustafa Mohamed Ahmed MBBS, MDDocument37 pagesBronchiolitis: Dr. Mustafa Mohamed Ahmed MBBS, MDYuusuf MubarikNo ratings yet
- Fresh H1N1 Guidelines 1 - 1-18Document15 pagesFresh H1N1 Guidelines 1 - 1-18Shahid IqbalNo ratings yet
- Pahonmhnvcovid 19200021 EngDocument7 pagesPahonmhnvcovid 19200021 EngBudi AnugrahNo ratings yet
- A3132020184314919 PDFDocument20 pagesA3132020184314919 PDFAnushka SoniNo ratings yet
- China CDC Covid-19 Diagnosis and TreatmentDocument8 pagesChina CDC Covid-19 Diagnosis and TreatmentGraham Caswell100% (2)
- Revised Guidelines For Homoeopathy Practitioners For Prophylaxis and Symptomatic Management of COVID-19 Patients in Home IsolationDocument6 pagesRevised Guidelines For Homoeopathy Practitioners For Prophylaxis and Symptomatic Management of COVID-19 Patients in Home IsolationBABUNo ratings yet
- COVID19 in Sickle Cell DiseaseDocument7 pagesCOVID19 in Sickle Cell DiseaseMohamed Ahmed FouadNo ratings yet
- TNSOP 6 Clinical GuidelinesDocument14 pagesTNSOP 6 Clinical Guidelinesazar103No ratings yet
- ANGLO - Jayson Joseph - Acute CoughDocument5 pagesANGLO - Jayson Joseph - Acute CoughJayson Joseph AngloNo ratings yet
- BTS Advice For Healthcare Professionals Treating Patients With AsthmaDocument3 pagesBTS Advice For Healthcare Professionals Treating Patients With AsthmaIzamar RomeroNo ratings yet
- Omar Taha - Nishteman Farzad - Ahmed Gaeib - Aven Majeed - Abdulwahab Ahmed - Lavan Majeed - Tabark KhawlanDocument45 pagesOmar Taha - Nishteman Farzad - Ahmed Gaeib - Aven Majeed - Abdulwahab Ahmed - Lavan Majeed - Tabark KhawlanAhmed HusseinNo ratings yet
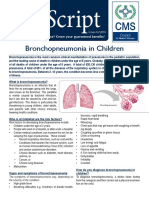
- Bronchopneumonia in ChildrenDocument3 pagesBronchopneumonia in ChildrenputraNo ratings yet
- Ayurveda PDFDocument46 pagesAyurveda PDFSiddhartha KumarNo ratings yet
- Clinical Management of COVID-19 Patients - v1Document18 pagesClinical Management of COVID-19 Patients - v1rohitNo ratings yet
- Clinical PracticeDocument10 pagesClinical PracticeCarlos AlvarezNo ratings yet
- Disease Outbreak Case StudyDocument7 pagesDisease Outbreak Case StudyFoxtrot NursingNo ratings yet
- Whats New in GINA 2021 - Final - V2Document52 pagesWhats New in GINA 2021 - Final - V2Wialda Dwi rodyahNo ratings yet
- The Journal For Nurse PractitionersDocument5 pagesThe Journal For Nurse Practitionersagstri lestariNo ratings yet
- Swine Flu Swine Flu: Ministry of Health and Family Welfare Government of IndiaDocument19 pagesSwine Flu Swine Flu: Ministry of Health and Family Welfare Government of IndiagirismgNo ratings yet
- Clinical Management Protocol For Covid-19: (In Adults)Document22 pagesClinical Management Protocol For Covid-19: (In Adults)Ahmed TarigNo ratings yet
- SJDH Chester Kyle Fernandez Risk AssessmentDocument8 pagesSJDH Chester Kyle Fernandez Risk AssessmentChester KyleNo ratings yet
- Muhimbili COVID SummaryDocument7 pagesMuhimbili COVID SummaryMeNo ratings yet
- 5 March 2021: An EDSS ScoreDocument8 pages5 March 2021: An EDSS ScorerobsonanselmoNo ratings yet
- Case Study For COVID 19 PatientDocument6 pagesCase Study For COVID 19 PatientNoelie Mae IglupasNo ratings yet
- SPH Lecture COVID19 2021Document16 pagesSPH Lecture COVID19 2021Ayisi BediakoNo ratings yet
- E. Nursing Management (Highlight The Priority Nursing Interventions)Document6 pagesE. Nursing Management (Highlight The Priority Nursing Interventions)Johanisa SultanNo ratings yet
- Clinical Management Protocol and Infection Control GuidelinesDocument16 pagesClinical Management Protocol and Infection Control Guidelinesalfaz lakhaniNo ratings yet
- Severe Covid-19: Clinical PracticeDocument10 pagesSevere Covid-19: Clinical Practicemarcelocarvalhoteacher2373No ratings yet
- Guidelines On Clinical Management of Covid - 19Document15 pagesGuidelines On Clinical Management of Covid - 19shah007zaadNo ratings yet
- Covid and Endocrine Diseases Ese Statement Final - 23032020Document7 pagesCovid and Endocrine Diseases Ese Statement Final - 23032020Oscar Lionel Echeverría OrellanaNo ratings yet
- Recommended Use of AntiviralsDocument4 pagesRecommended Use of AntiviralsMelroy D'souzaNo ratings yet
- Guidelines On Clinical Management of Severe Acute Respiratory Illness PDFDocument11 pagesGuidelines On Clinical Management of Severe Acute Respiratory Illness PDFSandeepNo ratings yet
- Advice For People With MSDocument10 pagesAdvice For People With MSAsma Al-MahmoudNo ratings yet
- 63e61cbd0e9c35001a1a86df 1676025084 CoViDDocument21 pages63e61cbd0e9c35001a1a86df 1676025084 CoViDAlthea Delos reyesNo ratings yet
- NEJM Severe COVIDDocument10 pagesNEJM Severe COVIDErick Roa GandicaNo ratings yet
- Neumonía en Niños - Tratamiento Hospitalario - UpToDateDocument42 pagesNeumonía en Niños - Tratamiento Hospitalario - UpToDatepao.pearanda1998No ratings yet
- Coronavirus: Novel Coronavirus (COVID-19) Infection: TerminologyDocument16 pagesCoronavirus: Novel Coronavirus (COVID-19) Infection: TerminologydeviNo ratings yet
- Professional Portfolio 2020Document10 pagesProfessional Portfolio 2020api-510438464No ratings yet
- Surface Anatomy of The HeartDocument5 pagesSurface Anatomy of The HeartEglNo ratings yet
- Devotion To Healthy Life & Leader of Healthcare Industry: GenediaDocument2 pagesDevotion To Healthy Life & Leader of Healthcare Industry: GenediaHaliun AltangerelNo ratings yet
- Transient Ischemic AttackDocument5 pagesTransient Ischemic AttackVijayabala JeevaganNo ratings yet
- The Structure and Function of White Blood CellsDocument8 pagesThe Structure and Function of White Blood CellsNaiomiNo ratings yet
- Current Medical Diagnosis and Treatment 2021 Maxine A Papadakis Full ChapterDocument67 pagesCurrent Medical Diagnosis and Treatment 2021 Maxine A Papadakis Full Chapterbill.groff554100% (3)
- Diabetes Transformation Summit 2022 Day 3Document5 pagesDiabetes Transformation Summit 2022 Day 3Paul Ioan PopescuNo ratings yet
- Demo Lab Report PDFDocument5 pagesDemo Lab Report PDFClintson PaulNo ratings yet
- Bacterial Men CPGDocument42 pagesBacterial Men CPGKarl Jimenez SeparaNo ratings yet
- Certificate PDFDocument1 pageCertificate PDFSanjay KudadaNo ratings yet
- Pembahasan Semester 4-5 Maret 2022Document21 pagesPembahasan Semester 4-5 Maret 2022Angger SatriaNo ratings yet
- DISPENSINGmanual Act. 2Document4 pagesDISPENSINGmanual Act. 2sybyl formenteraNo ratings yet
- Sales LiteratureDocument15 pagesSales Literaturehimanshu200k5154No ratings yet
- PN 1781 MolecuLight Overview Flyer A4 PRINTDocument2 pagesPN 1781 MolecuLight Overview Flyer A4 PRINTaaaaaaaaaNo ratings yet
- Answers and RationaleDocument6 pagesAnswers and RationaleSheana TmplNo ratings yet
- New List of Hospitals Empanelled Under DghsDocument9 pagesNew List of Hospitals Empanelled Under DghsHarish Delhi Govt.No ratings yet
- Simplifying Cheek Reconstruction A Review Of.11Document9 pagesSimplifying Cheek Reconstruction A Review Of.11royvillafrancaNo ratings yet
- Buy Nitrazepam OnlineDocument5 pagesBuy Nitrazepam OnlineShakilur RahmanNo ratings yet
- Kawasaki DiseaseDocument58 pagesKawasaki DiseaseLei OhNo ratings yet
- Schizophrenia Spectrum and Other Psychotic DisordersDocument8 pagesSchizophrenia Spectrum and Other Psychotic Disordersnaji santiagoNo ratings yet
- Nasogastric IntubationDocument4 pagesNasogastric IntubationDaphnie Mikaela Belarmino LayuganNo ratings yet
- Optical Neuritis: By: Antia Ayudika Supervisor M. Diana Rahim, MDDocument9 pagesOptical Neuritis: By: Antia Ayudika Supervisor M. Diana Rahim, MDdianarahimmNo ratings yet
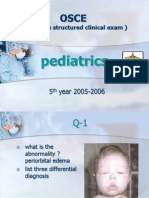
- Pediatrics Osce 2005-2006Document15 pagesPediatrics Osce 2005-2006marzieh_aa75% (4)
- The Role of A Hospital Pharmacist: Medicine ManagementDocument6 pagesThe Role of A Hospital Pharmacist: Medicine Managementsubhankar pradhan100% (1)
- Kuliah Pakar Modul 3.1Document68 pagesKuliah Pakar Modul 3.1Pramesti DarojahNo ratings yet
- Laryngo Tracheo BronchitisDocument4 pagesLaryngo Tracheo BronchitisNichole CollinsNo ratings yet