You might also like
- A Guide To DSM 5 Criteria For Substance Use DisordersDocument4 pagesA Guide To DSM 5 Criteria For Substance Use DisordersVergel MayoNo ratings yet
- 3 Soubliere - S APA 7th Template For DSM Summaries-1Document13 pages3 Soubliere - S APA 7th Template For DSM Summaries-1Sara SoubliereNo ratings yet
- Drug Abuse QuestionnaireDocument31 pagesDrug Abuse QuestionnaireAnjali Gulati100% (1)
- Substance Related SummaryDocument15 pagesSubstance Related SummaryMG SarabosingNo ratings yet
- Substance RelatedDocument12 pagesSubstance RelatedJoyce VillalesNo ratings yet
- Drug and Substance AbuseDocument16 pagesDrug and Substance Abuseangela marie abadillaNo ratings yet
- APA DSM5TR Level2SubstanceUseAdultDocument3 pagesAPA DSM5TR Level2SubstanceUseAdultGNo ratings yet
- Drug Dependence and Addiction: Understanding Stages, Costs, and TreatmentDocument65 pagesDrug Dependence and Addiction: Understanding Stages, Costs, and TreatmentSajjul KhanNo ratings yet
- Effects of Drugs - Comparing ConceptsDocument7 pagesEffects of Drugs - Comparing Conceptsgudy hurtadoNo ratings yet
- MapehDocument7 pagesMapehTala GinezNo ratings yet
- Substance Related DisorderDocument119 pagesSubstance Related DisorderSrea AgnesNo ratings yet
- DSM-5 Diagnosis Reference GuideDocument2 pagesDSM-5 Diagnosis Reference GuideDeAn White100% (1)
- English Asi PDFDocument3 pagesEnglish Asi PDFrujaklutisNo ratings yet
- Heroin AddictionDocument25 pagesHeroin AddictiondrsachinparabNo ratings yet
- Substance-Related and Addictive DisordersDocument28 pagesSubstance-Related and Addictive DisordersPersius NavalNo ratings yet
- Substance Use DisorderDocument5 pagesSubstance Use DisorderPATRICK OTIATONo ratings yet
- Abuse You LoseDocument16 pagesAbuse You LoseJayla BeckwithNo ratings yet
- DrogadiccionDocument5 pagesDrogadiccionYozeliin AltamiiranoNo ratings yet
- HLSC 1F90 November 7Document5 pagesHLSC 1F90 November 7Michael TruongNo ratings yet
- Drug Addiction GuideDocument18 pagesDrug Addiction GuideChrystall CaminadeNo ratings yet
- Drug Awareness Seminar: Police Community Relations LectureDocument93 pagesDrug Awareness Seminar: Police Community Relations LectureQuelly100% (3)
- Chap 12 - Hea201Document29 pagesChap 12 - Hea201Pierre BoutrosNo ratings yet
- Hallucinogen Disorders GuideDocument13 pagesHallucinogen Disorders GuideHillary BalderasNo ratings yet
- Hallucinogen-Related Disorders: Reported By: Hillary N. BalderasDocument13 pagesHallucinogen-Related Disorders: Reported By: Hillary N. BalderasHillary BalderasNo ratings yet
- Substance Use DisorderDocument28 pagesSubstance Use Disorderv.s rawatNo ratings yet
- Addiction to Marihuana: Symptoms, Withdrawal & Reasons to StopDocument3 pagesAddiction to Marihuana: Symptoms, Withdrawal & Reasons to StopVivi Ortiz BlancoNo ratings yet
- Prescription DrugsDocument14 pagesPrescription Drugsapi-302830378No ratings yet
- Clinical Assessment of Dual Disorder-9Document25 pagesClinical Assessment of Dual Disorder-9ruziyanaNo ratings yet
- DRUG ABUSE: CAUSES, SIGNS AND TREATMENT OPTIONSDocument27 pagesDRUG ABUSE: CAUSES, SIGNS AND TREATMENT OPTIONSRahul SharmaNo ratings yet
- Drug Education (Aj)Document17 pagesDrug Education (Aj)Jeanette FormenteraNo ratings yet
- MODULE 4 Drug Addiction and PreventionDocument15 pagesMODULE 4 Drug Addiction and PreventionSamuel ValdezNo ratings yet
- Substance Abuse DisorderDocument3 pagesSubstance Abuse DisorderZubiaNo ratings yet
- Unit VDocument67 pagesUnit VPriyaNo ratings yet
- Substance Abuse YouDocument59 pagesSubstance Abuse YouChristine Estemeso MadronaNo ratings yet
- Substance Abuse Disorders ExplainedDocument43 pagesSubstance Abuse Disorders ExplainedRahul Kumar Diwakar100% (1)
- Substance Related and Addictive DisorderDocument49 pagesSubstance Related and Addictive DisorderESPALMADO, Dianne N.No ratings yet
- DSM-5 Update: Substance-Related and Addictive Disorders: Presented By: Nick Lessa, LCSW, MA, CASACDocument67 pagesDSM-5 Update: Substance-Related and Addictive Disorders: Presented By: Nick Lessa, LCSW, MA, CASACrikunataNo ratings yet
- Drug Abuse BasicsDocument8 pagesDrug Abuse BasicssbanarjeeNo ratings yet
- Anshika5 OdtDocument19 pagesAnshika5 Odtanshika sharmaNo ratings yet
- DRUGDocument30 pagesDRUGKarl Louie PagaNo ratings yet
- Case ReportDocument58 pagesCase ReportMahnoor MalikNo ratings yet
- MAPEH 2nd HandoutsDocument5 pagesMAPEH 2nd HandoutsJesrhel Kate BelloNo ratings yet
- Chapter 10Document5 pagesChapter 10pairednursingNo ratings yet
- Module 2 Drug Education: The Nature of Drug and Drug AbuseDocument16 pagesModule 2 Drug Education: The Nature of Drug and Drug AbuseLoida MagallanesNo ratings yet
- Substance-Related Disorders DSM-V: A. Brain Changes Due To Substance Use 1. Autonomic/Limbic System ResponsesDocument7 pagesSubstance-Related Disorders DSM-V: A. Brain Changes Due To Substance Use 1. Autonomic/Limbic System ResponsesIngrid Karina GARCIA SANABRIANo ratings yet
- S.S. Jain Subodh Law Collage Dr. Bhimrao Ambedkar Law UniversityDocument18 pagesS.S. Jain Subodh Law Collage Dr. Bhimrao Ambedkar Law UniversityHimanshu GurjarNo ratings yet
- Week-10 NSTPDocument16 pagesWeek-10 NSTPRizielyn TorresNo ratings yet
- Drug Education: Bayani SartorioDocument12 pagesDrug Education: Bayani SartorioZhairra Marie DionsonNo ratings yet
- Penyalaggunaan Obat SedativeDocument8 pagesPenyalaggunaan Obat SedativeMarstaRavitriNo ratings yet
- Module 6 Drug Abuse Prevention and ControlDocument29 pagesModule 6 Drug Abuse Prevention and ControlAmon AmonNo ratings yet
- 10 Types of Substance Use DisordersDocument3 pages10 Types of Substance Use DisordersAlbert SamanteNo ratings yet
- How Drugs Work & Harm Reduction StrategiesDocument20 pagesHow Drugs Work & Harm Reduction StrategiesMaria Pia Sanchez ArroyoNo ratings yet
- Drug Addiction Causes and Remedial MeasuresDocument15 pagesDrug Addiction Causes and Remedial Measuresnitin0010No ratings yet
- PSYC 2300 042523 Lecture SlidesDocument19 pagesPSYC 2300 042523 Lecture SlidesCristinaNo ratings yet
- Investigatory Project on Drugs and its ClassificationDocument17 pagesInvestigatory Project on Drugs and its ClassificationSmileNo ratings yet
- Mental Health Module on Substance Abuse EffectsDocument30 pagesMental Health Module on Substance Abuse EffectsViolet CrimsonNo ratings yet
- Drug Education: REPUBLIC ACT NO. 9165 of June 7, 2002Document25 pagesDrug Education: REPUBLIC ACT NO. 9165 of June 7, 2002Jasmine Ayso Sinogaya100% (1)
- Substance - Related Addictive DisordersDocument43 pagesSubstance - Related Addictive DisordersMarinel June PalerNo ratings yet
- Teacher Quality and Student AchievementDocument44 pagesTeacher Quality and Student AchievementEducation JusticeNo ratings yet
- Paulo Freire and The Crisis of The PoliticalDocument7 pagesPaulo Freire and The Crisis of The PoliticalYenThiLeNo ratings yet
- An Islamic Perspective of Teaching Philosophy: A Personal JustificationDocument12 pagesAn Islamic Perspective of Teaching Philosophy: A Personal JustificationIOSRjournalNo ratings yet
- Friere Reviewed - Sue Jackson 2007Document17 pagesFriere Reviewed - Sue Jackson 2007YenThiLeNo ratings yet
- Free Play With Froebel - Use and Abuse of Progressive Pedagogy in London's Infant SchoolsDocument26 pagesFree Play With Froebel - Use and Abuse of Progressive Pedagogy in London's Infant SchoolsYenThiLeNo ratings yet
- Some Conceptual Problems of Critical PedagogyDocument26 pagesSome Conceptual Problems of Critical PedagogyYenThiLeNo ratings yet
- Sample Points of DefenceDocument1 pageSample Points of DefenceYenThiLeNo ratings yet
- Problematizing Critical Pedagogy: by Mary BreuingDocument22 pagesProblematizing Critical Pedagogy: by Mary BreuingAbdelalim TahaNo ratings yet
- What Are Some Examples of Philosophers of Education and Their Contributions - QuoraDocument4 pagesWhat Are Some Examples of Philosophers of Education and Their Contributions - QuoraYenThiLeNo ratings yet
- Progressivism Schools and Schools of EdDocument14 pagesProgressivism Schools and Schools of EdMonicaNo ratings yet
- 3 Dewey Freire and Foucault and An Ever-Evolving PhilosophyDocument10 pages3 Dewey Freire and Foucault and An Ever-Evolving PhilosophyМария РыжковаNo ratings yet
- Philosophies of Education - 2 Types of Teacher-CenteredDocument3 pagesPhilosophies of Education - 2 Types of Teacher-CenteredМария РыжковаNo ratings yet
- The Aim of Progressive EducationDocument7 pagesThe Aim of Progressive EducationYenThiLeNo ratings yet
- Pragmatism in Education: Sakshi Sharma Rajesh Devi Jyoti KumariDocument6 pagesPragmatism in Education: Sakshi Sharma Rajesh Devi Jyoti KumariJohn Mark Fernandez DanlagNo ratings yet
- Progressive Education Emphasis on Hands-On LearningDocument13 pagesProgressive Education Emphasis on Hands-On LearningYenThiLeNo ratings yet
- Pragmatism and Progressivism - Editable Venn Diagram Template On CreatelyDocument6 pagesPragmatism and Progressivism - Editable Venn Diagram Template On CreatelyYenThiLeNo ratings yet
- Paper 1 PDFDocument153 pagesPaper 1 PDFCriselAlamagNo ratings yet
- John Locke's Pioneering Views on EducationDocument12 pagesJohn Locke's Pioneering Views on EducationYenThiLeNo ratings yet
- 4 Major Educational PerspectiveDocument2 pages4 Major Educational PerspectiveJimson CorpuzNo ratings yet
- The Impact of Block Scheduling On Student MotivatiDocument19 pagesThe Impact of Block Scheduling On Student MotivatiYenThiLeNo ratings yet
- Philosophies of Education - 3 Types of Student-Centered Philosophies - The EdvocateDocument3 pagesPhilosophies of Education - 3 Types of Student-Centered Philosophies - The EdvocateYenThiLeNo ratings yet
- Modern Educational PhilosophiesDocument1 pageModern Educational PhilosophiesYenThiLeNo ratings yet
- Essentialism in Education - Online Essentialism in EducationDocument1 pageEssentialism in Education - Online Essentialism in EducationYenThiLeNo ratings yet
- Comparison of Education PhilosophyDocument5 pagesComparison of Education PhilosophyMarc Fernand Roberts100% (3)
- Education PhilosophiesDocument15 pagesEducation PhilosophiesElfera Adriana100% (1)
- Sustainability 11 03750Document20 pagesSustainability 11 03750silminaNo ratings yet
- EFA Global Report 2020Document14 pagesEFA Global Report 2020YenThiLeNo ratings yet
- Essentialism in Philosophy, Psychology, Education, Social and Scientific ScopesDocument12 pagesEssentialism in Philosophy, Psychology, Education, Social and Scientific ScopesAnatasia LeticiaNo ratings yet
- Canada - A Historical Overview of Education in CanadaDocument36 pagesCanada - A Historical Overview of Education in CanadaYenThiLeNo ratings yet
- Addiction - Substance AbuseDocument30 pagesAddiction - Substance AbusemidoNo ratings yet
- Decoding An Epidemic: Getting Beyond Conventional WisdomDocument39 pagesDecoding An Epidemic: Getting Beyond Conventional WisdomNational Press FoundationNo ratings yet
- Unintentional Nutmeg Autointoxication: J.E. Roeters Van Lennep, S.C.E. Schuit, R.L. Van Bruchem-Visser, B. ÖzcanDocument3 pagesUnintentional Nutmeg Autointoxication: J.E. Roeters Van Lennep, S.C.E. Schuit, R.L. Van Bruchem-Visser, B. Özcanarie ZogsNo ratings yet
- Local AnesthesiaDocument40 pagesLocal AnesthesiaKY HoNo ratings yet
- What Is Crystal Methamphetamine?Document2 pagesWhat Is Crystal Methamphetamine?losangelesNo ratings yet
- The World Drug Report - Executive Summary Chapter 1: Trends in World Drug Markets EvolutionDocument21 pagesThe World Drug Report - Executive Summary Chapter 1: Trends in World Drug Markets EvolutionlosangelesNo ratings yet
- Sympathomimetics and SympatholyticsDocument3 pagesSympathomimetics and Sympatholyticsbunso padillaNo ratings yet
- KlinikDocument165 pagesKlinikDwi Eka Suci WulandariNo ratings yet
- Opioid Dose Equivalence: Calculation of Oral Morphine Equivalent Daily Dose (oMEDD)Document3 pagesOpioid Dose Equivalence: Calculation of Oral Morphine Equivalent Daily Dose (oMEDD)Franz Josef TariganNo ratings yet
- Anti-Epileptic Drugs: - Classification of SeizuresDocument31 pagesAnti-Epileptic Drugs: - Classification of SeizuresgopscharanNo ratings yet
- Rapport DrogueDocument61 pagesRapport DrogueDefimediaNo ratings yet
- Chapter 5 DRUG EDUCDocument38 pagesChapter 5 DRUG EDUCRiza Roxanne ManongdoNo ratings yet
- CitalopramDocument3 pagesCitalopramunkown userNo ratings yet
- Pricelist Pharmasolindo 2018Document11 pagesPricelist Pharmasolindo 2018Niken Claudya Ecfrencylie0% (1)
- Mushroom Drug - Google SearchDocument1 pageMushroom Drug - Google SearchAishaNo ratings yet
- 30 CidDocument6 pages30 CidMa. Tiffany T. CabigonNo ratings yet
- Over 40 Medicines and Medical Supplies InventoryDocument7 pagesOver 40 Medicines and Medical Supplies InventoryTin Causaren-GertosNo ratings yet
- List Besaran Diskon Maksimal Per Produk: NO Kode Produk Komposisi Kemasan HNADocument4 pagesList Besaran Diskon Maksimal Per Produk: NO Kode Produk Komposisi Kemasan HNAapotekerNo ratings yet
- STOK RUANGAN OKDocument3 pagesSTOK RUANGAN OKok sayyidahNo ratings yet
- Nevid CH08 TBDocument94 pagesNevid CH08 TBAngela MarisNo ratings yet
- Book 2Document18 pagesBook 2fatha_87No ratings yet
- Price List Pt. Berkah Restu 24 Agustus 2022Document12 pagesPrice List Pt. Berkah Restu 24 Agustus 2022Klinik MuthmainnahNo ratings yet
- Azilect Uses, Dosage, Side Effects & InteractionsDocument6 pagesAzilect Uses, Dosage, Side Effects & InteractionspatgarettNo ratings yet
- Muscle RelaxantDocument33 pagesMuscle RelaxantLivia Nathania KosasihNo ratings yet
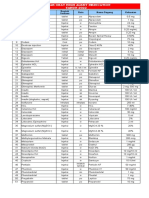
- High Alert Medications 2022Document4 pagesHigh Alert Medications 2022Abu Hisyam Al KhendaryNo ratings yet
- RespiratoryDocument1 pageRespiratoryMikaela LaoNo ratings yet
- Harm Reduction ZineDocument11 pagesHarm Reduction ZineAnonymous eWnP9dDu9100% (5)
- Fentanyl Fact Sheet 508c 1Document2 pagesFentanyl Fact Sheet 508c 1api-160935984No ratings yet
- WHO Analgesic Ladder: A Simple Guide for Pain ReliefDocument5 pagesWHO Analgesic Ladder: A Simple Guide for Pain ReliefKessi VikaneswariNo ratings yet
- Inventario Mensual Febrero 2023 - SMP 3 Codigo CAT Articulo LAB Total Entero Total FraccDocument58 pagesInventario Mensual Febrero 2023 - SMP 3 Codigo CAT Articulo LAB Total Entero Total Fraccsmp3similares similaresNo ratings yet