You might also like
- Evaluation of A Manual Identification System For Detection of Mycobacterium Tuberculosis in A Primary Tuberculosis Laboratory in ChinaDocument10 pagesEvaluation of A Manual Identification System For Detection of Mycobacterium Tuberculosis in A Primary Tuberculosis Laboratory in ChinaTonny YuliantoNo ratings yet
- Bactec Mgit 960 CultureDocument15 pagesBactec Mgit 960 CultureKanzlerin UrielNo ratings yet
- Validity of A CB NAAT Assay in Diagnosing Tube - 2020 - Journal of Clinical TubeDocument6 pagesValidity of A CB NAAT Assay in Diagnosing Tube - 2020 - Journal of Clinical TubeKarina ChristantoNo ratings yet
- The Manual MGIT System For The DetectionDocument5 pagesThe Manual MGIT System For The DetectionZhang NickNo ratings yet
- BactecDocument3 pagesBactecAjiNo ratings yet
- Improved Polyacrylamide-Based Artificial Sputum With Formalin-Fixed Tubercle Bacilli For Training of Tuberculosis MicroscopistsDocument6 pagesImproved Polyacrylamide-Based Artificial Sputum With Formalin-Fixed Tubercle Bacilli For Training of Tuberculosis MicroscopistsMuhammad Ricky RamadhianNo ratings yet
- The Veterinary Journal: Jun Zhang, Gui-Hong Zhang, Lin Yang, Ren Huang, Yu Zhang, Kun Jia, Wen Yuan, Shou-Jun LiDocument4 pagesThe Veterinary Journal: Jun Zhang, Gui-Hong Zhang, Lin Yang, Ren Huang, Yu Zhang, Kun Jia, Wen Yuan, Shou-Jun LiEdgar DíazNo ratings yet
- Automated antimicrobial susceptibility testingDocument2 pagesAutomated antimicrobial susceptibility testingJoshua TrinidadNo ratings yet
- Recent Advances in Tuberculosis Diagnostic Techniques: Review ArticleDocument6 pagesRecent Advances in Tuberculosis Diagnostic Techniques: Review ArticleMustaqeem DawarNo ratings yet
- DOC-20240208-WA0011.Document11 pagesDOC-20240208-WA0011.umayamajidNo ratings yet
- Issues Facing TB Control (5.1) Diagnostic Issues: Laboratory Diagnosis of Tuberculosis Present TechniquesDocument2 pagesIssues Facing TB Control (5.1) Diagnostic Issues: Laboratory Diagnosis of Tuberculosis Present TechniquesBest of shafiNo ratings yet
- Identification of TBC: Using MTP 64 Protein and Cord FormationDocument4 pagesIdentification of TBC: Using MTP 64 Protein and Cord FormationMarwa aljarahNo ratings yet
- Ingl in 2015Document4 pagesIngl in 2015EugeniaNo ratings yet
- Chromobacterium ViolaceumDocument6 pagesChromobacterium ViolaceumMelissa Giorgi OrtizNo ratings yet
- Diagnosis of TuberculosisDocument28 pagesDiagnosis of TuberculosisAnggi Apriansyah PNo ratings yet
- BBRC Vol 14 No 04 2021-20Document7 pagesBBRC Vol 14 No 04 2021-20Dr Sharique AliNo ratings yet
- BBRC Vol 14 No 04 2021-35Document7 pagesBBRC Vol 14 No 04 2021-35Dr Sharique AliNo ratings yet
- 1 s2.0 S0167701206000224 MainDocument9 pages1 s2.0 S0167701206000224 MainGirish Kishor PaiNo ratings yet
- Standard Operating Procedures Bacteriology 1steditionDocument160 pagesStandard Operating Procedures Bacteriology 1steditionfirewNo ratings yet
- 1-s2.0-S1684118223001512-mainDocument10 pages1-s2.0-S1684118223001512-maindiego sanchezNo ratings yet
- JM 002170Document4 pagesJM 002170carmen quispeNo ratings yet
- Mathematical Modeling of Capsular Polysaccharide PDocument8 pagesMathematical Modeling of Capsular Polysaccharide Pandreaosorio37No ratings yet
- Isolation and Identification of Bacteria ThesisDocument7 pagesIsolation and Identification of Bacteria Thesisafbtbegxe100% (2)
- Growth of Mycobacteria in Urine Determined by Isothermal Microcalor - 2012 - UroDocument4 pagesGrowth of Mycobacteria in Urine Determined by Isothermal Microcalor - 2012 - UroJerusalen BetancourtNo ratings yet
- Use of Hydrogen Peroxide Vapor For Deactivation ofDocument7 pagesUse of Hydrogen Peroxide Vapor For Deactivation ofMd. Saddam HossainNo ratings yet
- BAM CronobacterDocument15 pagesBAM CronobacterLACEN - Divisao de ProdutosNo ratings yet
- Micro LabDocument117 pagesMicro Labعبدالعزيز المحياNo ratings yet
- CTS QDs Staphylococus PDFDocument7 pagesCTS QDs Staphylococus PDFLicuriciMarcelaNo ratings yet
- Rapid Detection ESBLDocument7 pagesRapid Detection ESBLVenny PatriciaNo ratings yet
- Performance Survey and Comparison BetweeDocument9 pagesPerformance Survey and Comparison Betweemeredes gomezNo ratings yet
- SpoligotypingDocument17 pagesSpoligotypingmuchlis syahnuddinNo ratings yet
- Hayat cp3Document5 pagesHayat cp3hayatkuwaityNo ratings yet
- Metallo-Beta-Lactamase Producing Gram-Negative Bacterial IsolatesDocument6 pagesMetallo-Beta-Lactamase Producing Gram-Negative Bacterial IsolatesShyam MishraNo ratings yet
- Utility of Mycobacterium Tuberculosis PCR in Rul - 2020 - Journal of Clinical TuDocument5 pagesUtility of Mycobacterium Tuberculosis PCR in Rul - 2020 - Journal of Clinical TuKarina ChristantoNo ratings yet
- BMS Iddt 2020 41Document8 pagesBMS Iddt 2020 41Guneyden GuneydenNo ratings yet
- Molecular Analysis of Bacterial Contamination On Stethoscopes in An Intensive Care UnitDocument7 pagesMolecular Analysis of Bacterial Contamination On Stethoscopes in An Intensive Care UnitletuslearnNo ratings yet
- Lactobacillus Plantarium en Kombucha PDFDocument42 pagesLactobacillus Plantarium en Kombucha PDFPAULA ANDREA GUTIERREZ ALVAREZNo ratings yet
- Bioburden Recovery Method Using Swabbing TechniqueDocument8 pagesBioburden Recovery Method Using Swabbing TechniquePiruzi MaghlakelidzeNo ratings yet
- Use of Hydrogen Peroxide Vapor For Deactivation ofDocument6 pagesUse of Hydrogen Peroxide Vapor For Deactivation ofMd. Saddam HossainNo ratings yet
- Cutaneous Microabscesses by Mycobacterium Chelonae: Case Reports From A Tertiary Care Centre, TripuraDocument4 pagesCutaneous Microabscesses by Mycobacterium Chelonae: Case Reports From A Tertiary Care Centre, TripuraIJAR JOURNALNo ratings yet
- MycoDot PIDocument4 pagesMycoDot PITanveer100% (1)
- Microbial Culture CollectionDocument10 pagesMicrobial Culture CollectionNurul Apsari AjiNo ratings yet
- tmp8D22 TMPDocument3 pagestmp8D22 TMPFrontiersNo ratings yet
- Ecobios Paper .........Document5 pagesEcobios Paper .........hrishikesh08No ratings yet
- TBC y PCRDocument5 pagesTBC y PCRMayra Castillo CórdovaNo ratings yet
- S Aureus AssessmentDocument7 pagesS Aureus AssessmentmotibaNo ratings yet
- Fluoresent Monoclonal Neisseria GonorrheaDocument4 pagesFluoresent Monoclonal Neisseria GonorrheaGumbo PolonaNo ratings yet
- Sensitivity and Spec of PCR For TBDocument8 pagesSensitivity and Spec of PCR For TBGabriel KlemensNo ratings yet
- 217 - 219 Sensitivity of AedesDocument4 pages217 - 219 Sensitivity of Aedesfelipe andreNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument6 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Towards Detection of SARS-CoV-2 RNADocument8 pagesTowards Detection of SARS-CoV-2 RNARuben MonroyNo ratings yet
- Stepanovi Et Al 2007 ApmisDocument9 pagesStepanovi Et Al 2007 ApmisNicolás Matias Ruiz ValenzuelaNo ratings yet
- Device Independent, Real TimeidentificationofbacterialDocument6 pagesDevice Independent, Real TimeidentificationofbacterialHenny_OordNo ratings yet
- Ceotto, 2009Document8 pagesCeotto, 2009olindacabralNo ratings yet
- 108820lateral Move Molecular Assay For Horse StranglesDocument3 pages108820lateral Move Molecular Assay For Horse StranglesneriktjpcoNo ratings yet
- A Simplified Method of Three Dimensional Technique For The Detection of AmpC Beta-LactamasesDocument7 pagesA Simplified Method of Three Dimensional Technique For The Detection of AmpC Beta-LactamasesInternational Medical PublisherNo ratings yet
- Identification of Clinical Microbiology PathogensDocument2 pagesIdentification of Clinical Microbiology PathogensOrhan AsdfghjklNo ratings yet
- Microbios Que Permanecen en EstetoscopioDocument7 pagesMicrobios Que Permanecen en EstetoscopiojoaosabinoNo ratings yet
- A Method For The Detection of Cronobacter StrainsDocument7 pagesA Method For The Detection of Cronobacter StrainsLACEN - Divisao de ProdutosNo ratings yet
- The Chemistry of Milk v2Document1 pageThe Chemistry of Milk v2Florentina BarbălatăNo ratings yet
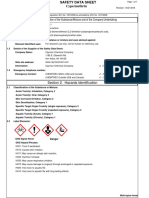
- Alphaplus® C24-28: Safety Data SheetDocument12 pagesAlphaplus® C24-28: Safety Data SheetlyesNo ratings yet
- Economy of Scale and Scope in Healthcare OperationsDocument22 pagesEconomy of Scale and Scope in Healthcare OperationsRavia SharmaNo ratings yet
- Public Workshop #1 PresentationDocument28 pagesPublic Workshop #1 PresentationEllyn SantiagoNo ratings yet
- Week10 Eth LMDocument8 pagesWeek10 Eth LMRenievave Torculas100% (2)
- Chapter I-V (Final)Document62 pagesChapter I-V (Final)Rhyll Dan ZanoNo ratings yet
- Rasika DietitianDocument3 pagesRasika DietitianChrill DsilvaNo ratings yet
- GATEWAY DRUGSDocument2 pagesGATEWAY DRUGSRegina ManlangitNo ratings yet
- 2020 Monitoring Drug TherapyDocument7 pages2020 Monitoring Drug Therapydolemite4No ratings yet
- Shine-On 22Document3 pagesShine-On 22I Gusti PradanaNo ratings yet
- Agesta Sacred Codes ListDocument22 pagesAgesta Sacred Codes Listmimigogo92% (12)
- Material Safety Data Sheet Cypermethrin PDFDocument7 pagesMaterial Safety Data Sheet Cypermethrin PDFSaid Muchsin AlkaffNo ratings yet
- 2023 ST HELENA BAY Course DatesDocument2 pages2023 ST HELENA BAY Course DatesNelson TolosseNo ratings yet
- Dental Clinic Safety Report Details ProgramsDocument2 pagesDental Clinic Safety Report Details ProgramsFay DeleCenNo ratings yet
- Forensic Psychologyin PracticeDocument17 pagesForensic Psychologyin PracticeDeepika L.No ratings yet
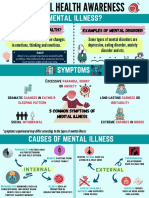
- Mental Health AwarenessDocument2 pagesMental Health Awarenessfarhatulhanimzulkifl100% (2)
- Understanding Hospital Emergency CodesDocument60 pagesUnderstanding Hospital Emergency CodesRemi0% (1)
- Tulajabahvani StotrDocument2 pagesTulajabahvani StotrHema DhaneNo ratings yet
- KPI Study on Middle Management PerceptionsDocument5 pagesKPI Study on Middle Management Perceptionsjigisha234100% (1)
- Healing Through LandscapeDocument28 pagesHealing Through LandscapeShinsha SaleemNo ratings yet
- Panel Outcome Letter Patient Eligible For CHC MGDocument2 pagesPanel Outcome Letter Patient Eligible For CHC MGDivine Mercy Apostolate UKNo ratings yet
- NUR 309 Informatics 2016-2017 Final ExamDocument10 pagesNUR 309 Informatics 2016-2017 Final ExamEmily ChiaravallotiNo ratings yet
- The Number of Grade 10 Serenity Students of School Year 2022-2023 at San Pedro National High School Affected by Verbal Abuse - Irritability, Stress, and Self-Harm - Anxiety - Research ProposalDocument5 pagesThe Number of Grade 10 Serenity Students of School Year 2022-2023 at San Pedro National High School Affected by Verbal Abuse - Irritability, Stress, and Self-Harm - Anxiety - Research ProposalMa Lourdez BayanNo ratings yet
- Nursing Rounds/case Methods/reports Nursing EducationDocument47 pagesNursing Rounds/case Methods/reports Nursing Educationrosana james100% (16)
- YDEW3004-Case Study-316103481Document15 pagesYDEW3004-Case Study-316103481Jenelle Lee ColeNo ratings yet
- Crisis Assessment Intervention and Prevention 2nd Edition Cherry Test BankDocument22 pagesCrisis Assessment Intervention and Prevention 2nd Edition Cherry Test Bankdolium.technic.1i5d67100% (30)
- CounterclaimsDocument3 pagesCounterclaimsRuthie PatootieNo ratings yet
- Martinez Gwu 0075A 13576Document152 pagesMartinez Gwu 0075A 13576امجد هليل السابلNo ratings yet
- Products You Can Cannot Mix 20Document2 pagesProducts You Can Cannot Mix 20RiaCasidsidNo ratings yet
- Cirugía de Colon Abierta Con "Fast Track" o Recuperación AceleradaDocument10 pagesCirugía de Colon Abierta Con "Fast Track" o Recuperación AceleradaManuelEduardoSanchezSotoNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (16)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- CBT Strategies: CBT Strategies for Overcoming Panic, Fear, Depression, Anxiety, Worry, and AngerFrom EverandCBT Strategies: CBT Strategies for Overcoming Panic, Fear, Depression, Anxiety, Worry, and AngerNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- How To Understand Your Anger For Better Mental Health: How To Control Emotions And Eliminate Stress In Your LifeFrom EverandHow To Understand Your Anger For Better Mental Health: How To Control Emotions And Eliminate Stress In Your LifeNo ratings yet
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Inmersion Into The Shadown Effective Method Of Dark Psychology: How To Use The Best Persuasion Techniques To Achieve Your Best Goals And How To Protect Yourself From Being ManipulatedFrom EverandInmersion Into The Shadown Effective Method Of Dark Psychology: How To Use The Best Persuasion Techniques To Achieve Your Best Goals And How To Protect Yourself From Being ManipulatedRating: 4 out of 5 stars4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)