You might also like
- Eye For An Eye: Ocular Prosthesis - A Case ReportDocument8 pagesEye For An Eye: Ocular Prosthesis - A Case ReportSkAliHassanNo ratings yet
- Fabrication of A Custom Ocular Prosthesis: Case ReportDocument4 pagesFabrication of A Custom Ocular Prosthesis: Case ReportIa HidaryaNo ratings yet
- IJPRDDEC2013EYEPROSTHESISDocument6 pagesIJPRDDEC2013EYEPROSTHESISSahana RangarajanNo ratings yet
- An Innovative Technique For Fabricating A CustomMade Ocular Prosthesis in A Pediatric Patient A Case ReportDocument4 pagesAn Innovative Technique For Fabricating A CustomMade Ocular Prosthesis in A Pediatric Patient A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Management of Phthisis Bulbi Patient with Scleral Cover Shell ProsthesisDocument4 pagesManagement of Phthisis Bulbi Patient with Scleral Cover Shell ProsthesisOliver GiroudNo ratings yet
- ManuscriptDocument3 pagesManuscriptAbhishek Kumar GuptaNo ratings yet
- Ocular ProsthesisDocument3 pagesOcular ProsthesisAmar BhochhibhoyaNo ratings yet
- Rehabilitation of Patient With Ocular Defects-Case ReportDocument4 pagesRehabilitation of Patient With Ocular Defects-Case ReportbhupendraNo ratings yet
- Sculpting The Eye Prosthetic Rehabilitation FollowDocument5 pagesSculpting The Eye Prosthetic Rehabilitation Followisichelichukwutem3No ratings yet
- Ocular Prosthesis BhavanDocument58 pagesOcular Prosthesis BhavanDrkvpratheep Pratheep100% (1)
- Technique for Fabricating Temporary Ocular ProsthesisDocument8 pagesTechnique for Fabricating Temporary Ocular ProsthesisDeepthi Rajesh100% (1)
- IJISRT20JAN543Document3 pagesIJISRT20JAN543International Journal of Innovative Science and Research TechnologyNo ratings yet
- 2011 Article 99Document4 pages2011 Article 99ali baridiNo ratings yet
- Dr. Kirti Kumsowar - 6Document2 pagesDr. Kirti Kumsowar - 6Zoya AfzalNo ratings yet
- Orbital ProsthesisDocument5 pagesOrbital ProsthesisdrsmritiNo ratings yet
- Nasal Prosthesis - A Case ReportDocument4 pagesNasal Prosthesis - A Case ReportInternational Organization of Scientific Research (IOSR)No ratings yet
- Dr. Kirti Kumsowar - 6Document6 pagesDr. Kirti Kumsowar - 6Manjeev GuragainNo ratings yet
- Customized Scale Aids Iris Orientation in Ocular ProsthesisDocument4 pagesCustomized Scale Aids Iris Orientation in Ocular ProsthesisRajsandeep SinghNo ratings yet
- Impression Techniques For Occular Prosthesis - ReviewDocument9 pagesImpression Techniques For Occular Prosthesis - ReviewIJAR JOURNALNo ratings yet
- Improved Edge Strength in A Facial Prosthesis by Incorporation of Tulle: A Clinical ReportDocument4 pagesImproved Edge Strength in A Facial Prosthesis by Incorporation of Tulle: A Clinical ReportmadalinaNo ratings yet
- Artificial Eye Seminar ReportDocument16 pagesArtificial Eye Seminar ReportKeerthan GowdaNo ratings yet
- The Ocular Prosthesis: A Novel Technique Using Digital PhotographyDocument7 pagesThe Ocular Prosthesis: A Novel Technique Using Digital Photographyhafidh akbarNo ratings yet
- 1st Article - Vikas AggarwalDocument4 pages1st Article - Vikas AggarwalSai VyshuNo ratings yet
- A New Clinical Approach in Fabrication of Closed Hollow Bulb Obturator: A Case ReportDocument4 pagesA New Clinical Approach in Fabrication of Closed Hollow Bulb Obturator: A Case ReportDr. Ravi Sagar Singh ShahiNo ratings yet
- Iris Foto DigitalDocument5 pagesIris Foto DigitalAnonymous iXvm527dNo ratings yet
- A Simplified Method For The Fabrication of Obturator:a Case ReportDocument4 pagesA Simplified Method For The Fabrication of Obturator:a Case ReportinventionjournalsNo ratings yet
- Ajcr 4 47Document2 pagesAjcr 4 47paulpiensaNo ratings yet
- Customized Thermoplast Retentive Aid For Partial Auricular Prosthesis-A Case ReportDocument9 pagesCustomized Thermoplast Retentive Aid For Partial Auricular Prosthesis-A Case ReportIJAR JOURNALNo ratings yet
- Sulcus Implantation of A Single-Piece Foldable Acrylic Intraocular Lens After Posterior Capsular Rupture in Cataract SurgeryDocument6 pagesSulcus Implantation of A Single-Piece Foldable Acrylic Intraocular Lens After Posterior Capsular Rupture in Cataract SurgeryPrizilia SaimimaNo ratings yet
- Rehabilitation of A Complex Oro-Facial Defect by Modified Prosthetic ApproachDocument3 pagesRehabilitation of A Complex Oro-Facial Defect by Modified Prosthetic ApproachBharat KhemaniNo ratings yet
- Clinical excellence in aesthetic implant placementDocument2 pagesClinical excellence in aesthetic implant placementDrMarkHoganNo ratings yet
- Ocular ProsthesisDocument28 pagesOcular ProsthesisrajaniNo ratings yet
- Positioning Magnets On A Multiple/Sectional Maxillofacial ProsthesisDocument7 pagesPositioning Magnets On A Multiple/Sectional Maxillofacial Prosthesisڣـڕٱټـي آڵـھـۈئNo ratings yet
- Implant-Retained Auricular Prosthesis: A Case Report: January 2010 - Vol.4Document4 pagesImplant-Retained Auricular Prosthesis: A Case Report: January 2010 - Vol.4noranNo ratings yet
- Innovative Rehabilitation Approach Spectacle-Retained Orbital Prosthesis For Post-Mucormycosis Orbital DefectDocument5 pagesInnovative Rehabilitation Approach Spectacle-Retained Orbital Prosthesis For Post-Mucormycosis Orbital DefectInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Abstract Id enDocument1 pageAbstract Id ennurqumirfanNo ratings yet
- Immediate Denture: Sandeep Shukla, S Swarajya Bharathi, Chandana Nair, Alok KumarDocument4 pagesImmediate Denture: Sandeep Shukla, S Swarajya Bharathi, Chandana Nair, Alok Kumarnur aslindahNo ratings yet
- Management of Hyper-Mobile Tissue With A Modified Combine Technique of Zafrulla and HobkrikDocument5 pagesManagement of Hyper-Mobile Tissue With A Modified Combine Technique of Zafrulla and HobkrikIJAR JOURNALNo ratings yet
- Case Report Fibre Post & All Ceramic Crown-A Simple Approach To The Perfect SmileDocument3 pagesCase Report Fibre Post & All Ceramic Crown-A Simple Approach To The Perfect SmileAlamMinersNo ratings yet
- CSE Artificial Eye REPORTDocument18 pagesCSE Artificial Eye REPORTVaibhav TiwariNo ratings yet
- Teflon Tape TechniqueDocument6 pagesTeflon Tape TechniqueJuan K. J. Shin100% (1)
- Prosthetic Rehabilitation of Compromised Ridges Maxillary Flabby Ridge and Severely Resorbed Mandibular Ridge - A Case ReportDocument6 pagesProsthetic Rehabilitation of Compromised Ridges Maxillary Flabby Ridge and Severely Resorbed Mandibular Ridge - A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Ocular and Orbital ProsthesisDocument69 pagesOcular and Orbital ProsthesisAkshayaa BalajiNo ratings yet
- Straumann Pro Arch DR EskanDocument3 pagesStraumann Pro Arch DR EskanShyam BhatNo ratings yet
- Implant Supported OverdentureDocument5 pagesImplant Supported OverdentureFadil ObiNo ratings yet
- Restoration of A Large Class IV Fracture Using Direct Composite Resin: A Clinical ReportDocument5 pagesRestoration of A Large Class IV Fracture Using Direct Composite Resin: A Clinical ReportYasmine SalsabilaNo ratings yet
- Single-Tooth Implants: A Procedure To Make A Precise, Flexible Gingival Contour On The Master Cast COELHO 1997Document2 pagesSingle-Tooth Implants: A Procedure To Make A Precise, Flexible Gingival Contour On The Master Cast COELHO 1997Douglas KrugNo ratings yet
- Five Year PROSE Treatment For Aniridic KojimaOct2016PAPDocument5 pagesFive Year PROSE Treatment For Aniridic KojimaOct2016PAP小島隆司No ratings yet
- Screenshot 2023-10-09 at 10.05.37Document7 pagesScreenshot 2023-10-09 at 10.05.37DevanyNataniaNo ratings yet
- Full Mouth Rehabilitation Restores Vertical DimensionDocument5 pagesFull Mouth Rehabilitation Restores Vertical DimensionammarkochiNo ratings yet
- Ocular Prosthesis PDFDocument2 pagesOcular Prosthesis PDFBrianNo ratings yet
- Crid2014 658790Document6 pagesCrid2014 658790paula catanaNo ratings yet
- Cold-Welded Healing Cap A Unique Implant Complication and Its ManagementDocument5 pagesCold-Welded Healing Cap A Unique Implant Complication and Its ManagementdeepthiNo ratings yet
- Clinical Report Rehabilitation of Maxillary Surgical Defect With A Cast Partial Denture ObturatorDocument4 pagesClinical Report Rehabilitation of Maxillary Surgical Defect With A Cast Partial Denture ObturatorSahana RangarajanNo ratings yet
- Rehabilitation of Maxillary Defects in Partial and Complete Edentulous Arches With Definitive Obturators-A Case SeriesDocument10 pagesRehabilitation of Maxillary Defects in Partial and Complete Edentulous Arches With Definitive Obturators-A Case SeriesIJAR JOURNALNo ratings yet
- 'The Mettle'' - Recent Advancement in Maxillofacial ProstheticsDocument4 pages'The Mettle'' - Recent Advancement in Maxillofacial ProstheticsAmaliNo ratings yet
- Rotational Stability of Toric Intraocular - 2022 - Medical Journal Armed ForcesDocument6 pagesRotational Stability of Toric Intraocular - 2022 - Medical Journal Armed ForcesAnisha RanaNo ratings yet
- Glued IOL Scaffold Technique for Soemmerring Ring RemovalDocument6 pagesGlued IOL Scaffold Technique for Soemmerring Ring RemovalAryananda Kondre AndikaNo ratings yet
- OCULOPATHY - Disproves the orthodox and theoretical bases upon which glasses are so freely prescribed, and puts forward natural remedial methods of treatment for what are sometimes termed incurable visual defectsFrom EverandOCULOPATHY - Disproves the orthodox and theoretical bases upon which glasses are so freely prescribed, and puts forward natural remedial methods of treatment for what are sometimes termed incurable visual defectsNo ratings yet
- Diane Derzis Motion To Dismiss Complaint by The Alabama State Board of Health To Stop Her From Operating An Abortion Clinic Closed by The State.Document8 pagesDiane Derzis Motion To Dismiss Complaint by The Alabama State Board of Health To Stop Her From Operating An Abortion Clinic Closed by The State.Tom CiesielkaNo ratings yet
- 465 886 1 SMDocument8 pages465 886 1 SM17Annisa Muthmainnah067No ratings yet
- Wrap Book A4Document27 pagesWrap Book A4doscribe100% (1)
- Vitality Book (1606456525)Document57 pagesVitality Book (1606456525)Ritu ShewaniNo ratings yet
- Wolf Gone Wild - Juliette CrossDocument312 pagesWolf Gone Wild - Juliette CrossAbdelhediNo ratings yet
- Entrepreneurs That Changed The Face of IndiaDocument4 pagesEntrepreneurs That Changed The Face of Indiamarykavitha_6No ratings yet
- Vrs PresentationDocument24 pagesVrs PresentationshrutipalkarNo ratings yet
- WP Stratasys TopFiveReasonsDocument7 pagesWP Stratasys TopFiveReasonscititorulturmentatNo ratings yet
- Diseases That Cause HypoproteinemiaDocument12 pagesDiseases That Cause HypoproteinemiaRachel Marie M. GaniaNo ratings yet
- Caffeine Natural Coffee BeanDocument1 pageCaffeine Natural Coffee BeanMayang TariNo ratings yet
- ARTIKEL 44 Famuntamah 391-399Document9 pagesARTIKEL 44 Famuntamah 391-399Dandi Aksan MasjudNo ratings yet
- Alkaline Phosphatase TestDocument6 pagesAlkaline Phosphatase TestShameema shami100% (1)
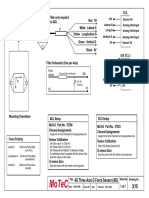
- Filter and wiring schematic for 3-axis ADL G-force sensorDocument1 pageFilter and wiring schematic for 3-axis ADL G-force sensorJuan Ramón Pérez LorenzoNo ratings yet
- Arthur Kleinman The Illness Narratives Suffering Healing and The Human ConditionDocument46 pagesArthur Kleinman The Illness Narratives Suffering Healing and The Human Conditionperdidalma62% (13)
- Chapter 8-Mental Health and Well-Being in Middle and LateDocument15 pagesChapter 8-Mental Health and Well-Being in Middle and LateCathleen Beth100% (2)
- BInggrisDocument19 pagesBInggrisanwar318No ratings yet
- 1-Well Completion I PDFDocument20 pages1-Well Completion I PDFHomam MohammadNo ratings yet
- Constance Carroll Cosmetics) Final.1Document4 pagesConstance Carroll Cosmetics) Final.1api-26027438100% (1)
- 1619928348861forensic Science UNIT - VII 1 PDFDocument159 pages1619928348861forensic Science UNIT - VII 1 PDFVyshnav RNo ratings yet
- Life Wealth Mastery EnglishDocument12 pagesLife Wealth Mastery EnglishD.j. Ralmm100% (1)
- 3 - 2017 - Superia X 5 StarDocument26 pages3 - 2017 - Superia X 5 Starsomnath serviceNo ratings yet
- DCM601A51 - Technical DataDocument405 pagesDCM601A51 - Technical Datathanhthuan100% (1)
- Animal Names in English and Telugu - 20170912 - 182216545Document17 pagesAnimal Names in English and Telugu - 20170912 - 182216545karimulla goraNo ratings yet
- Structural Notes and Specifications for ConcreteDocument1 pageStructural Notes and Specifications for Concreteroger100% (2)
- Community-Based Forest ManagementDocument7 pagesCommunity-Based Forest ManagementZiazel ThereseNo ratings yet
- 4 ReactorsDocument58 pages4 ReactorsKiran ShresthaNo ratings yet
- Quality Assurance in The Manufacture of Light Unmanned Aircraft SystemDocument4 pagesQuality Assurance in The Manufacture of Light Unmanned Aircraft SystemAhmad Zubair RasulyNo ratings yet
- Silver Rain Svetlana Perevalova PDFDocument9 pagesSilver Rain Svetlana Perevalova PDFAndrea Koumarian100% (1)
- Ibsen in PracticeDocument17 pagesIbsen in PracticevictorkalkaNo ratings yet
- Chapter III Pharmacokinetics: Durge Raj GhalanDocument64 pagesChapter III Pharmacokinetics: Durge Raj GhalanDurge Raj Ghalan100% (3)