You might also like
- Soltan2020 Article KnowledgeRiskPerceptionAndPrevDocument8 pagesSoltan2020 Article KnowledgeRiskPerceptionAndPrevزينب بنت لفإل مدّسرNo ratings yet
- Factors Influencing The Epidemiological Characteristics of Pandemic COVID 19: A TISM ApproachDocument11 pagesFactors Influencing The Epidemiological Characteristics of Pandemic COVID 19: A TISM ApproachDivine AguilarNo ratings yet
- Concepts in Disaster MedicineDocument8 pagesConcepts in Disaster MedicinedaniaNo ratings yet
- Knowledge, and Practice Towards Infection Control Measures For The Novel Corona Virus Among Nurses Working at Isolation DepartmentDocument49 pagesKnowledge, and Practice Towards Infection Control Measures For The Novel Corona Virus Among Nurses Working at Isolation DepartmentOmima MuhammedNo ratings yet
- The COVID-19 Pandemic: Implications For The Cytology LaboratoryDocument10 pagesThe COVID-19 Pandemic: Implications For The Cytology LaboratoryAndy SetiawanNo ratings yet
- Modelling Transmission and Control of The COVID-19 Pandemic in AustraliaDocument24 pagesModelling Transmission and Control of The COVID-19 Pandemic in AustraliafaithnicNo ratings yet
- Musa Et Al. (2021) - Assessing The Potential Impact of Immunity Waning On The Dynamics of COVID-19 An Endemic Model of COVID-19Document21 pagesMusa Et Al. (2021) - Assessing The Potential Impact of Immunity Waning On The Dynamics of COVID-19 An Endemic Model of COVID-19Cristian Fernando Sanabria BautistaNo ratings yet
- Group 3 PR2Document21 pagesGroup 3 PR2jaxxNo ratings yet
- Cellular and Molecular ImmunologyDocument21 pagesCellular and Molecular ImmunologyMUGDHA MITTALNo ratings yet
- Critical Issues in Public Health: Yarmouk UniversityDocument12 pagesCritical Issues in Public Health: Yarmouk UniversityTamara ShNo ratings yet
- PIIS0140673621015890Document2 pagesPIIS0140673621015890Anastasija LevcenkoNo ratings yet
- COVID-19 Update For Nurses: Greetings From The QA Team!!Document8 pagesCOVID-19 Update For Nurses: Greetings From The QA Team!!Mable CNo ratings yet
- 1 s2.0 S152169422100005X MainDocument10 pages1 s2.0 S152169422100005X MainnordonkNo ratings yet
- Vaccines and Routine Immunization Strategies During The COVID 19 PandemicDocument9 pagesVaccines and Routine Immunization Strategies During The COVID 19 PandemicMěđ SimoNo ratings yet
- The Impact of Covid-19 Towards The Development of A CountryDocument17 pagesThe Impact of Covid-19 Towards The Development of A CountryMUHAMMAD ARIFIN BIN SAPUANNo ratings yet
- Underestimation of The Number of Covid19 Cases An Epidemiological ThreatDocument2 pagesUnderestimation of The Number of Covid19 Cases An Epidemiological ThreatEliosNo ratings yet
- Visce NiagaDocument18 pagesVisce NiagaAbdul Adhim MustaqimNo ratings yet
- Haischer Et Al - Who Is Wearing A MaskDocument12 pagesHaischer Et Al - Who Is Wearing A MaskK L YEONo ratings yet
- When Will The COVID-19 Pandemic End?Document39 pagesWhen Will The COVID-19 Pandemic End?hvsbouaNo ratings yet
- Candida Auris Rapti 2023Document14 pagesCandida Auris Rapti 2023John HenryNo ratings yet
- Covid19 A Tale of Two Epidemics March 20 2020Document3 pagesCovid19 A Tale of Two Epidemics March 20 2020Tewfic SeidNo ratings yet
- International Immunopharmacology: Hyun Jee Han, Chinekwu Nwagwu, Obumneme Anyim, Chinedu Ekweremadu, San KimDocument11 pagesInternational Immunopharmacology: Hyun Jee Han, Chinekwu Nwagwu, Obumneme Anyim, Chinedu Ekweremadu, San KimyoshefarieNo ratings yet
- 21 - Muhamad Ihsan Nuril Anwar - Covid19 - 18032020Document29 pages21 - Muhamad Ihsan Nuril Anwar - Covid19 - 18032020Muhamad Ihsan Nuril AnwarNo ratings yet
- Prospects For Sars-Cov-2 Diagnostics, Therapeutics and Vaccines in AfricaDocument15 pagesProspects For Sars-Cov-2 Diagnostics, Therapeutics and Vaccines in AfricaÃßD ÔûñîNo ratings yet
- Velavan Et Al-2020-Tropical Medicine International HealthDocument4 pagesVelavan Et Al-2020-Tropical Medicine International Healthjunior rodriguesNo ratings yet
- Review of COVID On CADocument14 pagesReview of COVID On CAvit1234No ratings yet
- Math Model On Covid Social Distancing EffectivenessDocument9 pagesMath Model On Covid Social Distancing EffectivenessNJUGUNA AUSTIN KIMUHUNo ratings yet
- Research Paper 2 ReviewDocument6 pagesResearch Paper 2 ReviewThe Code RunNo ratings yet
- Perceptions On Public Safety Towards Regulating The Rollout of COVID-19 Vaccination Among The Residents of BongaoDocument10 pagesPerceptions On Public Safety Towards Regulating The Rollout of COVID-19 Vaccination Among The Residents of BongaoPsychology and Education: A Multidisciplinary JournalNo ratings yet
- LEMBAR KERJA SISWA Virus Corona OKDocument18 pagesLEMBAR KERJA SISWA Virus Corona OKAbraham MaramisNo ratings yet
- Effectiveness of Covid 19 ResearchDocument9 pagesEffectiveness of Covid 19 ResearchAinah Faith LegaspiNo ratings yet
- Benefit of Covid-19 VaccineDocument9 pagesBenefit of Covid-19 VaccineKevo KarisNo ratings yet
- Running Head: Benefits of The Covid-19 Vaccine 1Document7 pagesRunning Head: Benefits of The Covid-19 Vaccine 1bonnieNo ratings yet
- Tang BiologyRPDocument5 pagesTang BiologyRPRyder TangNo ratings yet
- COVIDDocument17 pagesCOVIDnensih suryanensihNo ratings yet
- The Potential Impact of The COVID-19 Pandemic On Antimicrobial Resistance and Antibiotic StewardshipDocument8 pagesThe Potential Impact of The COVID-19 Pandemic On Antimicrobial Resistance and Antibiotic StewardshipAdil JDNo ratings yet
- Chaurasia, Pal - 2020 - Application of Machine Learning Time Series Analysis For Prediction COVID-19 Pandemic-AnnotatedDocument13 pagesChaurasia, Pal - 2020 - Application of Machine Learning Time Series Analysis For Prediction COVID-19 Pandemic-AnnotatedZipeng WuNo ratings yet
- The Use of The Health Belief Model To Assess Predictors of Intent To Receive The COVID 19 Vaccine and Willingness To PayDocument12 pagesThe Use of The Health Belief Model To Assess Predictors of Intent To Receive The COVID 19 Vaccine and Willingness To PayMuhammad ImranNo ratings yet
- Knowledge Attitude and Risk Perception of COVID 19 in Rural Ghana A ViewpointDocument6 pagesKnowledge Attitude and Risk Perception of COVID 19 in Rural Ghana A ViewpointAthenaeum Scientific PublishersNo ratings yet
- Accepted Manuscript: Preventing COVID-19 Collateral DamageDocument19 pagesAccepted Manuscript: Preventing COVID-19 Collateral Damagekayegi8666No ratings yet
- Vaccination Strategies Against COVID 19 and The Diffusion of Anti Vaccination ViewsDocument13 pagesVaccination Strategies Against COVID 19 and The Diffusion of Anti Vaccination ViewsShaila PrabhuNo ratings yet
- Assessment of Knowledge, Attitudes, and Perception of Health Care Workers Regarding COVID-19Document10 pagesAssessment of Knowledge, Attitudes, and Perception of Health Care Workers Regarding COVID-19andris mejia alvarezNo ratings yet
- Lks Virus Corona (Covid-19) Xii Ips-3 Dikdik SunanjarDocument15 pagesLks Virus Corona (Covid-19) Xii Ips-3 Dikdik SunanjarAlika 52No ratings yet
- Lks Virus Corona (Covid-19) Xii Ips-3 Dikdik SunanjarDocument15 pagesLks Virus Corona (Covid-19) Xii Ips-3 Dikdik SunanjarAlika 52No ratings yet
- Pharmaceuticals 13 00143 v2Document14 pagesPharmaceuticals 13 00143 v2Sundas EjazNo ratings yet
- Vaksin 2Document9 pagesVaksin 2Arumm88No ratings yet
- LEMBAR KERJA SISWA Virus Corona OKDocument28 pagesLEMBAR KERJA SISWA Virus Corona OKSaep SudarjoNo ratings yet
- Summary of Guidance For Minimizing The Impact of COVID-19 On Individual Persons, Communities, and Health Care Systems - United States, August 2022Document8 pagesSummary of Guidance For Minimizing The Impact of COVID-19 On Individual Persons, Communities, and Health Care Systems - United States, August 2022PANAMA GREEN BUILDING COUNCILNo ratings yet
- Lembar Kerja SiswaDocument25 pagesLembar Kerja SiswaMuhammad HaikalNo ratings yet
- LKS Virus CoronaDocument21 pagesLKS Virus CoronaOshNo ratings yet
- Hygiene Hypothesis CovidDocument9 pagesHygiene Hypothesis Covidmicro sdcNo ratings yet
- Preprint Modelling of COVID-19 Vaccination Strategies and Herd Immunity, in Scenarios of Limited and Full Vaccine SupplyDocument29 pagesPreprint Modelling of COVID-19 Vaccination Strategies and Herd Immunity, in Scenarios of Limited and Full Vaccine SupplyArifin SiregarNo ratings yet
- Coronavirus Disease 2019 (COVID-19) : Because Learning Changes EverythingDocument29 pagesCoronavirus Disease 2019 (COVID-19) : Because Learning Changes EverythingDennis MuthusiNo ratings yet
- Sahwa Aisya SafitriDocument21 pagesSahwa Aisya SafitriSahwa Aisyah safitriNo ratings yet
- Rifqi Julyana Firdaus Lembar Kerja Siswa (LKS) Virus CoronaDocument22 pagesRifqi Julyana Firdaus Lembar Kerja Siswa (LKS) Virus CoronaRifqi Julyana FirdausNo ratings yet
- Rethinking Lockdowns Joffe COMMENTARY FWebDocument12 pagesRethinking Lockdowns Joffe COMMENTARY FWebGllauber Marlon RibeiroNo ratings yet
- Virus Corona FixDocument14 pagesVirus Corona FixEka FadlilaNo ratings yet
- Covid 19Document3 pagesCovid 19Manpinder SinghNo ratings yet
- 2021 PSL CovidDocument10 pages2021 PSL CovidRalph Gerard SangalangNo ratings yet
- Guidelines: For (COVID-19) Prevention in The Work LocationDocument9 pagesGuidelines: For (COVID-19) Prevention in The Work LocationGhazanfar GulNo ratings yet
- The New Pregnancy and Lactation Labeling RuleDocument3 pagesThe New Pregnancy and Lactation Labeling RuleVijendra RNo ratings yet
- Servillance and Out BreakDocument79 pagesServillance and Out BreakruthNo ratings yet
- Clinical Features of DiarrhoeaDocument4 pagesClinical Features of DiarrhoeaKhogen MairembamNo ratings yet
- CertificateDocument1 pageCertificateRanjana RanjanaNo ratings yet
- Meher Assessment 2014 (1) NONFoodDocument90 pagesMeher Assessment 2014 (1) NONFoodMERHAWIT NEGATUNo ratings yet
- A Rational Approach To Septic Tank Design: March 2012Document12 pagesA Rational Approach To Septic Tank Design: March 2012Jannatun NaimNo ratings yet
- Thesis PresentationDocument114 pagesThesis PresentationFgNo ratings yet
- Presentation: The Mor-Sand Filter in The Niger DeltaDocument19 pagesPresentation: The Mor-Sand Filter in The Niger DeltarawdpNo ratings yet
- Health Promotion and Primary Health Care PDFDocument34 pagesHealth Promotion and Primary Health Care PDFKavya S Mohan100% (2)
- Nipah Virus PDFDocument2 pagesNipah Virus PDFRakesh SahuNo ratings yet
- Asymptomatic Bacteriuria in Adults - UpToDateDocument20 pagesAsymptomatic Bacteriuria in Adults - UpToDatefilipiNo ratings yet
- Акушерство Фукс англ 2019Document875 pagesАкушерство Фукс англ 2019ȜLaa AsHrafNo ratings yet
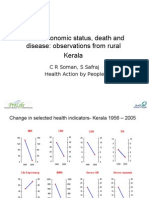
- Socio Economic Status and Health in KeralaDocument17 pagesSocio Economic Status and Health in Keralasafraj5003No ratings yet
- DPR UNNAO CityfinalDocument216 pagesDPR UNNAO CityfinalNikhil GNo ratings yet
- The Grand MultiparaDocument5 pagesThe Grand MultiparaIndhumathiNo ratings yet
- Coast Guard Public School, Daman: (Type Here)Document13 pagesCoast Guard Public School, Daman: (Type Here)Rajeev SinghNo ratings yet
- EU/EEA Digital COVID Certificate EU/EØS Digitalt KoronasertifikatDocument3 pagesEU/EEA Digital COVID Certificate EU/EØS Digitalt KoronasertifikatVegardNo ratings yet
- Sample of MRCOG Assessment 2021 - Saeed HasanDocument28 pagesSample of MRCOG Assessment 2021 - Saeed HasanIslam AwniNo ratings yet
- Guideline Regimen TB Ro 2019 PDFDocument61 pagesGuideline Regimen TB Ro 2019 PDFrima melliaNo ratings yet
- Vaccination Myths - A. G. PhillipsDocument11 pagesVaccination Myths - A. G. PhillipsBrendan D. MurphyNo ratings yet
- Hawiyah Gas Plant Expansion: Basic Safety Instructions For All Employees Working atDocument10 pagesHawiyah Gas Plant Expansion: Basic Safety Instructions For All Employees Working atmalik jahanNo ratings yet
- Vaccines For Children & Child Vaccination Schedule at Rainbow HospitalsDocument4 pagesVaccines For Children & Child Vaccination Schedule at Rainbow Hospitalsmuralikrishna221No ratings yet
- Guideline URTI in South Africa 2008Document9 pagesGuideline URTI in South Africa 2008Febbe Nadia Okky LucianaNo ratings yet
- Guidelines For Preventive Activities in General PracticeDocument382 pagesGuidelines For Preventive Activities in General PracticeDr. Serin KuriakoseNo ratings yet
- Afsana Afroz, Khurshid Alam, Mohammed J Alramadan, MD Nassif Hossain, Hasina Akhter Chowdhury, Liaquat Ali, Dianna J Magliano, Baki BillahDocument7 pagesAfsana Afroz, Khurshid Alam, Mohammed J Alramadan, MD Nassif Hossain, Hasina Akhter Chowdhury, Liaquat Ali, Dianna J Magliano, Baki BillahS1 FARMASI STIKESNAS ANGKATAN 2 2017No ratings yet
- Prevent Cross Contamination and Mix UpDocument2 pagesPrevent Cross Contamination and Mix UpPrince Moni100% (1)
- Research Proposal BDU Institute of TechnologyDocument22 pagesResearch Proposal BDU Institute of Technologysolomon demissew100% (3)
- Evaluasi Program Early Warning Alert and Surveilans KLB Kota Salatiga Provinsi Jawa TengahDocument9 pagesEvaluasi Program Early Warning Alert and Surveilans KLB Kota Salatiga Provinsi Jawa TengahIinAstikaNo ratings yet
- Cumulative Analysis of Post-Authorization Adverse Event Reports of PF-07302048 (BNT162B2) Received Through 28-Feb-2021Document38 pagesCumulative Analysis of Post-Authorization Adverse Event Reports of PF-07302048 (BNT162B2) Received Through 28-Feb-2021adan_infowars96% (49)