You might also like
- Urology: Kidneys BladderDocument26 pagesUrology: Kidneys BladderChristineGonzalesNo ratings yet
- Surg 3.4 - LiverDocument8 pagesSurg 3.4 - LiveryayayanizaNo ratings yet
- Anatomy of PeritoneumDocument61 pagesAnatomy of PeritoneumFirdaus SeptiawanNo ratings yet
- Anatomy of Urinary SystemDocument43 pagesAnatomy of Urinary SystemIrfan Ali JunejoNo ratings yet
- Organ Anatomy Notes 1Document8 pagesOrgan Anatomy Notes 1ELIANA CARIS CABILDONo ratings yet
- Anatomy of Liver and Pancreas by Kazim AliDocument32 pagesAnatomy of Liver and Pancreas by Kazim AliAhmad KhanNo ratings yet
- Peritoneum: General FeaturesDocument92 pagesPeritoneum: General FeaturestuhinsinghNo ratings yet
- Laparoscopic Anatomy of The Abdominal CavityDocument14 pagesLaparoscopic Anatomy of The Abdominal CavityUffie-Isabela GheNo ratings yet
- Anatomy of The LiverDocument25 pagesAnatomy of The Liverapi-354184238100% (1)
- Molecular Pathology of Liver Diseases - S. Monga (Springer, 2011) WW PDFDocument956 pagesMolecular Pathology of Liver Diseases - S. Monga (Springer, 2011) WW PDFMoldovan Tiberiu100% (2)
- III - Digestive SystemDocument3 pagesIII - Digestive SystemGael QuingNo ratings yet
- Table e - Liver Anatomy Biliary SystemDocument11 pagesTable e - Liver Anatomy Biliary Systemapi-371971600No ratings yet
- Esophagus and StomachDocument33 pagesEsophagus and StomachIrfan Falah100% (1)
- Abdomen Engl PDFDocument51 pagesAbdomen Engl PDFShuler0071No ratings yet
- Anatomy MCQ - Abdomen - 2Document15 pagesAnatomy MCQ - Abdomen - 2ahsan gujjarNo ratings yet
- Liver Anatomy and ResectionDocument62 pagesLiver Anatomy and ResectionNurfa Mustamir100% (1)
- Powerpoint: Liver Surgical DiseasesDocument95 pagesPowerpoint: Liver Surgical Diseasesj.doe.hex_8792% (12)
- Thursday, April 09, 2009 4:45 PMDocument266 pagesThursday, April 09, 2009 4:45 PMkcs2012No ratings yet
- Liver CirrhosisDocument31 pagesLiver CirrhosisAsniah Hadjiadatu Abdullah100% (1)
- 8) Anatomy of Liver&spleennnjnjDocument25 pages8) Anatomy of Liver&spleennnjnjSumayyah AkbarNo ratings yet
- Peritonem A ND Peritonealcavity PDFDocument62 pagesPeritonem A ND Peritonealcavity PDFKarem MaaliNo ratings yet
- Abdomen #7: DR - Bushra Haseeb BDS, Rds Demonstrator in Dental Section Azra Naheed Medical CollegeDocument21 pagesAbdomen #7: DR - Bushra Haseeb BDS, Rds Demonstrator in Dental Section Azra Naheed Medical CollegeTanveer AhmadNo ratings yet
- 10 The LiverDocument54 pages10 The LiverAbdullah HaroonNo ratings yet
- Organ Anatomy Notes 2Document11 pagesOrgan Anatomy Notes 2ELIANA CARIS CABILDONo ratings yet
- Gross Anatomy LiverDocument51 pagesGross Anatomy LiverDeny ShajiniNo ratings yet
- Histology of The Esophagus and Stomach-1Document34 pagesHistology of The Esophagus and Stomach-1kuchipuchi12No ratings yet
- ANAT 221 - PeritoneumDocument22 pagesANAT 221 - PeritoneumWisdom IkechukwuNo ratings yet
- Kidney and Ureter For Paramedical StudentsDocument53 pagesKidney and Ureter For Paramedical Studentslakshmiraman1770No ratings yet
- Anatomy of The KidneyDocument16 pagesAnatomy of The Kidneycnk4qrjgb6No ratings yet
- Abdominal-Cavity TransDocument23 pagesAbdominal-Cavity TransMigz BolivarNo ratings yet
- Anal PathologyDocument28 pagesAnal PathologyHaashveeni Jayan KumarNo ratings yet
- Gross Anatomy and Histolgy of UrinarysystemDocument81 pagesGross Anatomy and Histolgy of UrinarysystemIncredible DivineNo ratings yet
- KidneyDocument16 pagesKidneykhatheejahani12No ratings yet
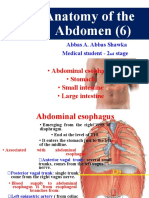
- Anatomy of The Abdomen (6) : - Abdominal Esophagus - Stomach - Small Intestine - Large IntestineDocument34 pagesAnatomy of The Abdomen (6) : - Abdominal Esophagus - Stomach - Small Intestine - Large IntestineBilal YimamNo ratings yet
- Abbas A. A. Shawka 2 Year Medical StudentDocument15 pagesAbbas A. A. Shawka 2 Year Medical StudentPlutokidNo ratings yet
- PANCREASDocument9 pagesPANCREASNitin KumarNo ratings yet
- 01-Anatomy of KidneyDocument19 pages01-Anatomy of KidneyGanapathyGaneshNo ratings yet
- 7) Anatomy of OMENTUMDocument22 pages7) Anatomy of OMENTUMGoodone OneNo ratings yet
- 01-Anatomy of KidneyDocument32 pages01-Anatomy of KidneyMRS DR NIDHI SHARMA VISHWAKARMANo ratings yet
- GasterDocument179 pagesGasterAraka Patriota100% (1)
- Anatomi Gaster Dan DuodenumDocument179 pagesAnatomi Gaster Dan DuodenumHaraka NabdaNo ratings yet
- Urinary Bladder, Rectum and Anal CanalDocument34 pagesUrinary Bladder, Rectum and Anal CanalIbe ClementNo ratings yet
- Urinary Kidney and HeartDocument9 pagesUrinary Kidney and HeartVillanueva, AbegailNo ratings yet
- Intro To Abdominal Cavity (Merrick)Document35 pagesIntro To Abdominal Cavity (Merrick)Sidiq AboobakerNo ratings yet
- Surgical Anatomy of PeritoneumDocument63 pagesSurgical Anatomy of PeritoneumSuvarna RajNo ratings yet
- Large Intestine PIMSR-Dr - Gosai 2022Document40 pagesLarge Intestine PIMSR-Dr - Gosai 2022Dr.B.B.GosaiNo ratings yet
- CHAPTER 9-Body CavitiesDocument3 pagesCHAPTER 9-Body CavitiespraiseginelcNo ratings yet
- Colon, Caecum & Appendix 2017Document67 pagesColon, Caecum & Appendix 2017yasrul izad0% (1)
- DiaphragmDocument18 pagesDiaphragmAuza Moses IbrahimNo ratings yet
- Development of GIT - IDocument69 pagesDevelopment of GIT - IAarushi JainNo ratings yet
- UGS - MaleDocument44 pagesUGS - MaleSʌɩĸʌt PʌʋɭNo ratings yet
- Transes - AbdomenDocument8 pagesTranses - AbdomencamatoviancaNo ratings yet
- 01-Anatomy of KidneyDocument19 pages01-Anatomy of KidneyDr.Shahana banuNo ratings yet
- Anatomy of The Abdomen: Samara University Biomedical Sciences DepartmentDocument142 pagesAnatomy of The Abdomen: Samara University Biomedical Sciences Departmentfentaw melkieNo ratings yet
- Liver & Gall Bladder: Presented by DR - Sujaya NairDocument102 pagesLiver & Gall Bladder: Presented by DR - Sujaya Nairjoy rajNo ratings yet
- General AnatomyDocument46 pagesGeneral AnatomyIhab IsmailNo ratings yet
- Anatomy of GIT For PCII Students..Document106 pagesAnatomy of GIT For PCII Students..AMANUEL HABTEWOLDNo ratings yet
- HA Notes Whole Term 2Document21 pagesHA Notes Whole Term 2kpv454yk7mNo ratings yet
- Abdominal CavityDocument78 pagesAbdominal Cavitytanishapatel1005No ratings yet
- Development of Alimentary System Part 1Document52 pagesDevelopment of Alimentary System Part 1Aarushi JainNo ratings yet
- Yusi - Anatomy of The Urinary Tract 2009 12-7Document129 pagesYusi - Anatomy of The Urinary Tract 2009 12-7abstabsNo ratings yet
- Gross Anatomy of The Kidney 2Document22 pagesGross Anatomy of The Kidney 2Precious JuliusNo ratings yet
- Anatomy of Lower Gastrointestinal TractDocument26 pagesAnatomy of Lower Gastrointestinal TractOmar Ali AyoubkhanNo ratings yet
- Small Intestine 2017Document78 pagesSmall Intestine 2017yasrul izadNo ratings yet
- Anatomy of BladderDocument10 pagesAnatomy of BladderKiran tyraNo ratings yet
- The AbdomenDocument67 pagesThe AbdomenOriade TaiwoNo ratings yet
- Helling2014 - Ton That Tung's LiversDocument8 pagesHelling2014 - Ton That Tung's Livershoangducnam100% (1)
- Gross Anatomy LiverDocument51 pagesGross Anatomy LiverDeny ShajiniNo ratings yet
- Liver Pancreas SpleenDocument88 pagesLiver Pancreas SpleenGabi NaeNo ratings yet
- Past Paper - 221208 - 003047Document96 pagesPast Paper - 221208 - 003047Ashraf ShalbiNo ratings yet
- Anatomy-1-HepatologyDocument16 pagesAnatomy-1-HepatologyPrashant SapkotaNo ratings yet
- Proliferative and Nonproliferative Lesions of The Rat and Mouse Hepatobiliary SystemDocument77 pagesProliferative and Nonproliferative Lesions of The Rat and Mouse Hepatobiliary SystemVlad TomaNo ratings yet
- Mcqs For The Abdomen and PosteriorDocument14 pagesMcqs For The Abdomen and PosteriorMohamed TawalbeNo ratings yet
- Liver Anatomy - Portal (And Suprahepatic) or Biliary Segmentation PDFDocument9 pagesLiver Anatomy - Portal (And Suprahepatic) or Biliary Segmentation PDFBîndar CristianNo ratings yet
- Anatomy 7 Digestive SystemDocument181 pagesAnatomy 7 Digestive SystemJeanette LynnNo ratings yet
- Aad Abdomen WorksheetDocument15 pagesAad Abdomen WorksheetAchNo ratings yet
- Human Body Minipedia - Nodrm-16-30Document15 pagesHuman Body Minipedia - Nodrm-16-30kailashNo ratings yet
- Zakim and Boyers Hepatology A Textbook of Liver Disease 7Th Edition Arun J Sanyal Ebook Full ChapterDocument51 pagesZakim and Boyers Hepatology A Textbook of Liver Disease 7Th Edition Arun J Sanyal Ebook Full Chapterwesley.sharon378100% (14)
- (Oncologysurgery) Graeme J Poston, Michael DAngelica, Rene ADAM - Surgical Management of Hepatobiliary and Pancreatic Di 1Document630 pages(Oncologysurgery) Graeme J Poston, Michael DAngelica, Rene ADAM - Surgical Management of Hepatobiliary and Pancreatic Di 1Marlene MartínezNo ratings yet
- Liver Function and AnatomyDocument2 pagesLiver Function and AnatomyKeanna Nicole CollantesNo ratings yet
- Obstructive JaundiceDocument34 pagesObstructive Jaundicemogesie1995No ratings yet
- Human Anatomy. Abdominal CavityDocument104 pagesHuman Anatomy. Abdominal Cavitynero20012No ratings yet
- Anatomi CT Scan AbdomenDocument17 pagesAnatomi CT Scan Abdomenwawan saifullahNo ratings yet
- Lesson Plan LiverDocument9 pagesLesson Plan LiverSAYMABANUNo ratings yet
- Liver - WikipediaDocument148 pagesLiver - WikipediaMuhammad HuzaifaNo ratings yet
- 2 Biliary Anatomy and EmbrDocument16 pages2 Biliary Anatomy and EmbrShawn GravesNo ratings yet
- Liver & Gall Bladder: Presented by DR - Sujaya NairDocument102 pagesLiver & Gall Bladder: Presented by DR - Sujaya Nairjoy rajNo ratings yet
- Refrensi Soal UAS Anatomi PraktikumDocument20 pagesRefrensi Soal UAS Anatomi Praktikumshendy aurelyaNo ratings yet
- Dokumen Tanpa JudulDocument11 pagesDokumen Tanpa JudulRabiatul adhwiyah DalimuntheNo ratings yet