Professional Documents
Culture Documents
QEMG
Uploaded by
Cindy nnnCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
QEMG
Uploaded by
Cindy nnnCopyright:
Available Formats
Critical Reviews™ in Biomedical Engineering, 38(5):467–485 (2010)
A Review of Clinical Quantitative Electromyography
Charles Farkas,1 Daniel W. Stashuk,1* Andrew Hamilton-Wright2, & Hossein Parsaei1
1
Department of Systems Design Engineering, University of Waterloo, Ontario, Canada; 2Department of Math and
Computer Science, Mount Allison University, New Brunswick, Canada
*Address all correspondence to Dr. Daniel W. Stashuk, Department of Systems Design Engineering, University of Waterloo, 200 University Avenue West, Waterloo,
Ontario, Canada, N2L 3G1. Tel.: 519-888-4567, ext. 32982; Fax: 519-746-4791; e-mail: stashuk@uwaterloo.ca.
ABSTRACT: Information regarding the morphology of motor unit potentials (MUPs) and motor unit firing pat-
terns can be used to help diagnose, treat, and manage neuromuscular disorders. In a conventional electromyographic
(EMG) examination, a clinician manually assesses the characteristics of needle-detected EMG signals across a
number of distinct needle positions and forms an overall impression of the condition of the muscle. Such a subjec-
tive assessment is highly dependent on the skills and level of experience of the clinician, and is prone to a high error
rate and operator bias. Quantitative methods have been developed to characterize MUP waveforms using statistical
and probabilistic techniques that allow for greater objectivity and reproducibility in supporting the diagnostic pro-
cess. In this review, quantitive EMG (QEMG) techniques ranging from simple reporting of numeric MUP values
to interpreted muscle characterizations are presented and reviewed in terms of their clinical potential to improve
status quo methods. QEMG techniques are also evaluated in terms of their suitability for use in a clinical decision
support system based on previously established criteria. Aspects of prototype clinical decision support systems are
then presented to illustrate some of the concepts of QEMG-based decision making.
KEY WORDS: EMG signal; motor unit potentials; motor unit potential trains; motor unit firing patterns; quan-
titative EMG; clinical decision support
I. CLINICAL QUANTITATIVE ELECTROMYOGRAPHY
Neuromuscular disorders change the morphology and activation patterns of the motor units of the af-
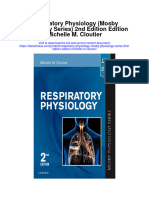
fected muscles. As depicted in Figure 1, myopathic disorders in general maintain the number of motor
units in a muscle but reduce the number of muscle fibers in motor units due to fiber necrosis, atrophying
some fibers while hypertrophying others and thus increasing the range of fiber diameters and densities
in the motor units. To compensate for fiber loss and diameter changes, more motor units are required to
be recruited and to fire more often in myopathic muscle than in healthy muscle to create a specific level
of contraction. In contrast, neurogenic disorders in general cause a loss of motoneurons and thus motor
units. However, denervated fibers are reinnervated by axonal sprouts of surviving motor units, resulting
in motor units with large territories and numbers of fibers, and uneven motor unit fiber densities. These
motor unit fiber changes are also depicted in Figure 1. As a result of motor unit loss and reinnervation,
fewer motor units are required to be recruited in neurogenic muscle than in healthy muscle to create a
specific level of contraction.
Characteristics of suitably detected electromyographic (EMG) signals can reflect the morphology
and activation patterns of the motor units of a muscle, and can therefore be used to infer the degree and
type of disorder that may have affected the muscle. Therefore, EMG signals suitably detected, processed,
ABBREVIATIONS
EMG, electromyographic; LDA, linear discriminant analysis; MUP, motor unit potential; MUPT, motor unit po-
tential train; QEMG, quantitative electromyography
0278-940X/10/$35.00 © 2010 by Begell House, Inc. 467
468 Farkas et al
FIGURE 1. Schematic representation of the effects of the various categories of neuromuscular disor-
ders (Reprinted with permission from Stalberg and Falck1). A, Normal muscle; B, neurogenic muscle,
and C, myopathic muscle.
and analyzed can be used to detect neuromuscular not provide enough discrimination between the
disorders. In this regard, the differences between motor unit potentials (MUPs) of near and distant
needle- and surface-detected EMG signals need motor units. One exception to this is the use of
to be considered. Although surface-detected EMG high-density selective surface EMG techniques
signals have many areas of application and have capable of resolving the spatial and temporal ar-
received much recent attention, in general, they do rangements of the MUPs of concurrently active
not provide the sensitivity needed for clinical use. motor units.2-4 In principle, such techniques could
Typical surface electrodes cannot be positioned be used clinically. However, their use is currently
sufficiently close to motor unit territories to reflect impeded by instrumentation complexities and their
subtle morphological changes, and the respective clinical utility is only beginning to be evaluated.
changes in the EMG signal characteristics become This review therefore focuses solely on the clinical
obscured and confounded. In addition, surface use of needle-detected EMG signals.
electrodes typically cannot be used to statistically Current clinical practice is to qualitatively
sample motor units throughout a muscle, and do interpret insertional, spontaneous, and voluntary
Critical Reviews™ in Biomedical Engineering
A Review of Clinical QEMG 469
needle-detected EMG activity to determine the makers to interpret and mentally compare numeric
degree and type of disorder that has affected a information without the necessary context or level
muscle under examination. Although such qualita- of explanation. Such shortcomings of quantified
tive assessments allow an experienced physician to data highlight a specific characteristic that deci-
infer a host of underlying conditions and diseases, sion support and QEMG methods must possess:
it is subjective and related to the skill and experi- transparency. Transparency is especially important
ence of the physician. Moreover, it is lacking the when dealing with complex data structures, such as
precision of quantitative analysis. multivariate distributions of MUP feature values
Quantitative EMG (QEMG) is the process of or other statistical parameters. A system that can
extracting quantitative information related to the explain its conclusions in a manner that is consis-
morphology and activation of motor units from tent with, and analogous to, the cognitive processes
EMG signals.1,5 Such information can be used for employed by a human decision maker can thus
exploration of the underlying structure and opera- improve upon the quality and accuracy of the in-
tion of the peripheral neuromuscular control system, ferences made. Therefore, the degree to which the
and for the clinical characterization of muscle tissue findings and supporting evidence can be presented
with respect to detection of disease or abnormality. and explained to support the decision-making pro-
Several QEMG techniques have been developed to cess is an important factor to consider when devel-
quantize important aspects of needle EMG exami- oping a clinical decision-support system. How the
nations, resulting in a more precise numerical and findings and supporting evidence are presented and
statistical representation of their results.5-10 These explained to support the decision-making process
techniques provide a wide range of outputs, from is also very important.
a simple reporting of numeric MUP values to in- QEMG techniques attempt to reproducibly
terpreted muscle characterizations. QEMG-based extract useful muscle information from sets of fea-
muscle characterizations, and quantitative methods ture values used to represent important EMG signal
in general, can have a significant impact by present- characteristics. Features can represent characteris-
ing quantitative information in a way that supports tics of a composite EMG signal (i.e., interference
the clinical decision-making process. QEMG tools pattern) or of individual MUP trains (MUPTs) ex-
have the advantage of higher accuracy and greater tracted from a composite EMG signal using either
precision, but must be tailored to a specific purpose simple triggering techniques or more sophisticated
and thus are not intended to replace current clini- decomposition techniques. With respect to the
cal examinations but to augment certain aspects by latter, time domain features related to MUP size,
improving their accuracy and consistency. shape, and stability or features of transformed or
QEMG techniques have been demonstrated to modeled MUP waveforms have been used. QEMG
be effective in a number of research studies using methods use rigorous statistical and/or probabilis-
human data.11-20 They have also been applied in vet- tic inference in which feature values from EMG
erinary practice, wherein QEMG-based techniques signals detected in the muscle under examination
were shown to be more effective than the analysis (i.e., test EMG signals) are compared with respect
of muscle enzyme activity for monitoring training to distributions of corresponding values obtained
adaptation in racehorses.21 Nonetheless, despite from exemplary EMG data. By describing the sta-
their potential for improving subjective analysis, tistical similarities or differences between test val-
QEMG techniques are not widely understood or ues and exemplary data, it is possible to character-
used by clinicians. One of the main impediments ize EMG signals or constituent MUP waveforms
to the widespread acceptance of QEMG tech- acquired from a muscle under examination. This
niques is the inherent difficulty of presenting vast allows a clinical decision maker to use to the fullest
amounts of quantified data in a way that can be the information present in the test EMG signals
easily interpreted. It is difficult for human decision and, in addition, to leverage information extracted
Volume 38, Number 5, 2010
470 Farkas et al
from previously acquired (exemplary) signals. Such then combined to arrive at an overall impression
exemplary data must be acquired and stratified by or characterization of the muscle. Finally, a rule or
an expert clinician. In addition, it must be specifi- heuristic is applied to categorize the muscle based
cally acquired for each muscle or groups of muscles on the characterization measures obtained.
studied, and should be stratified by age or any other
relevant stratification criteria (e.g., gender) and in- I.A. Needle EMG Examination
corporated into a repository (database).
QEMG analysis has the advantage of provid- A recent review by Daube and Rubin22 describes
ing greater objectivity and consistency, and is use- in detail how to properly complete a clinical nee-
ful for equivocal cases to increase the certainty of dle EMG examination. Briefly, a needle electrode
a diagnosis.22 Furthermore, the precision obtained (monopolar or concentric) is inserted into the su-
with more sophisticated quantitative techniques perficial layers of a muscle and the resultant detect-
can provide continuous measures that also relate to ed EMG signals are assessed based on three types
the level of involvement of a disorder.23 Compared of detected activity: insertional, spontaneous, and
with qualitative methods, QEMG methods can be voluntary. In all cases, the electrode must be posi-
more robust and reproducible. They can provide tioned to sample several regions of the muscle to
analytic confidence (i.e., provide measures of un- obtain a sufficient statistical sampling of the mo-
certainty or error) and have the ability to generalize tor units. When assessing voluntary activity, EMG
across sets of EMG signals. signals are assessed at a low level of contraction,
The reproducibility and robustness of EMG with only a few active motor units contributing to
data assessment are two important criteria used to the signal. However, if decomposition techniques
evaluate QEMG methods. Being able to discuss are used, EMG signals with five to seven motor
the degree to which similar feature values can be unit contributions can be assessed.22 Either way, it
obtained from similar EMG signals, coupled with is important to position the needle to detect MUPs
discussions related to the sources and types of con- with a rapid rise time to ensure that the detection
founding errors present, makes it possible to consider surface is sufficiently close to the fibers of the ac-
the entire workflow of obtaining decision-making tive motor units. It is also important to ensure that
data from an EMG signal in terms of reproducibil- the level of each contraction is consistent, so that
ity, robustness, and the general quality of the out- abnormally large or small MUPs may be attrib-
come measures provided by EMG-based analysis. uted to morphological changes in the muscle and
Whether EMG data are used for the exploration thus representative of disease and not be related
of muscle structure and function or to detect and to different sizes of active motor units due to dif-
characterize disease, it is clear that metrics for the fering levels of muscle activation. QEMG tech-
quality of the data are invaluable, and by measur- niques have not as of yet been applied to study
ing and improving data quality, any inference made EMG signals related to insertional or spontaneous
based on this data will also be improved. muscle activity. Therefore, the following discussion
Regardless of whether a qualitative or quan- focuses on EMG signals detected during volun-
titative assessment is used, a similar hierarchical tary muscle activity.
process is followed. First, in order to account for
the large variability in motor unit size and MUP I.B. Qualitative Characterization
shape throughout a muscle, MUP or/and other sig-
nal features are assessed at several needle positions Traditionally, needle EMG signals detected dur-
within a muscle. The data from these various needle ing voluntary activation are qualitatively charac-
positions are then characterized based on whether terized based on visual and auditory assessment of
they possess attributes consistent with certain dis- the morphology, stability, and times of occurrence
ease processes. The characterized sampled data are of their MUPs. In addition, the intensity of com-
Critical Reviews™ in Biomedical Engineering
A Review of Clinical QEMG 471
posite EMG signals (i.e., interference patterns) are provide further references to standardized values
described using terms ranging from full to sparse for manual visual and auditory assessment.22,24
in an effort to assess motor unit activation. These
characterizations are usually manually quantized II. QUANTITATIVE CHARACTERIZATION
and charted. While such qualitative assessment is
prone to a high error rate, a skilled practitioner can This review focuses on QEMG techniques using
use it to detect not just the broad category of dis- features extracted from individual MUPTs. Quan-
ease, but also certain processes that are symptomatic titative characterization of extracted MUPTs can
of a specific disease or group of disease processes. be accomplished in several ways and with vary-
MUP analysis is useful in determining the type ing degrees of complexity. MUPTs can be isolated
of disorder (myopathic or neurogenic), as well as semi-automatically using level or window trigger-
the time course and severity of the disease. How- ing, or automatically using signal decomposition
ever, qualitative analysis is limited to the MUPs of methods. In principle, any of these isolation tech-
only a few active motor units at a time. Motor unit niques can be used as long as the MUPTs used to
morphology is inferred based on the assessment of train a system are isolated in the same way as those
the duration, amplitude, and number of phases of being characterized. Standardization across EMG
detected MUPs. During qualitative assessment, a clinics requires the use of consistent needle elec-
physician keeps track of abnormally small or large trodes, filter settings, and detection protocols. Fur-
MUPs and polyphasic MUPs and assigns rankings thermore, training data must be grouped based on
based on severity. the specific muscle, age, and possibly gender. Oth-
MUP stability refers to consistency of MUP erwise, even though numerical data are extracted,
morphology across the MUPs of a MUPT and can the final interpretation may be biased and have a
indicate impaired transmission across the neuro- large margin for error.
muscular junctions of a motor unit. Although MUP Properly performed, the most immediate ben-
instability is typically a sign of disease of the neuro- efit of quantitative characterization is the provision
muscular junctions, such as myasthenia gravis, any of more precise continuous values for features like
disorder associated with denervation/reinnervation duration, amplitude, and number of phases/turns.
may cause unstable MUPs. Continuous-value features make it possible to
Motor unit activation patterns are assessed derive relationships among features such as area,
in terms of the level of motor unit activation and thickness, and size index,25 as well as measures of ir-
recruitment. Low activation represents a central regularity, such as the “irregularity coefficient.”26,27
process such as a central nervous system disorder Decomposition-based quantitative analysis5,6,7
or manifestation of pain. Compromised motor has the advantage that EMG signals detected dur-
unit recruitment is found in neurogenic diseases, ing higher levels of contraction can be analyzed
and sometimes in end-stage myopathy, whereas (usually five to seven MUPs), and features related
early recruitment (i.e., increased activation) is typi- to MUP stability, such as jitter,28 and to motor
cally a sign of myopathy. According to Preston and unit activation patterns, such as the mean and
Shapiro,23 motor unit activation analysis is one of standard deviation of the inter-discharge intervals
the most difficult tasks for an electromyographer. of a MUPT, can be provided. The automation of
Qualitative motor unit activation analysis is limited decomposition methods also provides a consider-
to very low levels of contraction, in which only a able time-saving advantage, especially with the
small number of motor units are active; otherwise, recent availability of cost-effective computational
the interference pattern makes motor unit activa- resources.29-32
tion become qualitatively indiscernible. Daube and The first QEMG methods developed charac-
Shapiro describe the normal and abnormal varia- terize MUPs based on morphological features of
tions of motor unit activation characteristics, and the shape and size of a template or average MUP,
Volume 38, Number 5, 2010
472 Farkas et al
because this is similar to what is done qualitatively scatter to achieve an optimal decision function for
and it is easy to define and measure these features. each muscle category. Pino et al.14,40 evaluated the
Quantitative MUP characterizations based on performance of linear discriminant analysis deci-
transformations of the MUP template have also sion trees, and a standard naive Bayes classifier,39
been developed, but suffer from less transparency and found that MUP categorization performance
and greater complexity. Quantitative analogs for was comparable across these methods. The advan-
characterization based on measures of MUP sta- tage of conventional classifier techniques is that
bility and motor unit activation have not yet been their simplistic nature allows for some degree of
developed. While such measures have been quanti- transparency, provided that a clinician has a mod-
fied, their values are currently reported solely for erate statistical background, although their perfor-
qualitative interpretation. mance is subject to the data upholding certain as-
sumptions, such as obeying a Gaussian distribution
II.A. MUP Characterization and independence across features.
MUP characterization and classification was in- 2. Advanced Pattern Recognition Tech-
troduced by Pattichis et al. and further developed niques
by several groups of investigators.33-38 Based on a
training set of features extracted from exemplary When MUP categorization accuracy is considered
MUP templates, MUP characterization calculates as the evaluation criteria, conventional classification
a set of scores that indicate the likelihood that the techniques do not provide the best performance.
muscle from which a MUP template was calculat- Therefore, advanced pattern recognition techniques
ed is affected by a specific category of disease based have been used to improve performance. In these
on the characteristics of the MUP template. In a studies, the true categories of MUP templates were
two-category case, the likelihood of a muscle be- manually determined by an expert neurophysiolo-
ing normal or abnormal conditioned on the char- gist to create a database of MUP templates. In their
acteristics of the MUP template is estimated. In a early work, Pattichis et al.33,41 were the first to de-
three-category case, which is more common, the velop a decision-making strategy based on artificial
likelihood of a muscle being normal, myopathic, neural networks combined with Kohonen self-or-
or neurogenic conditioned on the characteristics ganizing feature maps and a learning vector quanti-
of the MUP template is estimated. Features of the zation technique to perform MUP characterization
MUP template used for training and testing can based on morphological MUP features. Katsis et
be morphological, extracted from a time domain al. 37 used artificial neural networks with radial ba-
representation, or spectral, related to a frequency sis functions and probabilistic neural networks in
domain representation. a two-stage classification approach. The first stage
used an artificial neural network or probabilistic
1. Conventional Classifiers neural network to discriminate between normal
and abnormal MUPs, and the second stage used
Several MUP characterization techniques based a C4.5 decision tree42 to determine whether the
on classifiers that use continuous valued features abnormality was myopathic or neurogenic. Several
have been proposed. Linear discriminant analysis39 techniques using alternate MUP representations
was used by Pfeiffer and Kunze, and later by Pino, have also been suggested. Pattichis and others have
Stashuk, and Podnar as a candidate for a muscle used autoregressive and cepstral analysis to rep-
characterization methodology.11,12,23 Linear dis- resent MUPs,35 as well as the wavelet transform
criminant analysis statistically transforms data in an method,34 while Katsis et al.36 used MUP time
attempt to minimize within-class scatter (variance) domain samples and a support vector machine to
while simultaneously maximizing between-class perform raw EMG-based classification of decom-
Critical Reviews™ in Biomedical Engineering
A Review of Clinical QEMG 473
posed MUPs. Although these advanced pattern While pattern discovery was been shown to
recognition-based MUP characterization tech- have accuracy comparable to other classification
niques are robust and accurate, several drawbacks techniques,13,40 it is not considered to be as robust
have been noted. For example, artificial neural net- as some of the other classification methods because
work methods have a tendency toward over-fitting, of the need for discretizing the continuous feature
which results in a difficulty of generalizing to new values. The number of intervals (“bins”) used for
data.33,41 In addition, while most of the advanced discretization must be carefully selected to manage
pattern recognition techniques, including artificial the trade-off between the level of granularity (and
neural networks, support vector machines and oth- accuracy) and the quality of evidence. For example,
ers offer greater sensitivity and specificity, they do if the number of intervals increases, more training
not provide good transparency. It is difficult to in- data are needed to determine if specific patterns are
tuitively appreciate how they make their decisions. significant. Decreasing the number of intervals re-
Poor transparency leads to poor acceptance of the sults in larger discretization ranges, which decreases
results and the techniques by clinicians. the precision of the MUP representation.
In other areas of medicine, fuzzy-logic-based
3. Transparent Rule-based Techniques inference systems offer an attractive alternative
to conventional characterization techniques. The
The issue of transparency can be addressed by em- general idea is to represent hard numeric values
ploying rule-based methods. The two-stage meth- by linguistic expressions, in which a membership
od developed by Katsis et al.37 is able to provide a function determines the degree to which a variable
level of transparency and interpretability by using falls within a particular decision boundary. The
a decision tree to discriminate between myopathic benefit of such a system is that it allows quanti-
and neurogenic categories. Pino14,40 used the pat- ties to be represented by linguistic qualifiers like
tern discovery technique developed by Wang and somewhat high, high, very high, and expressions such
Wong43 to characterize MUPs. Pattern discovery as hot, cold, warm. Hamilton-Wright38 proposed
quantizes all continuous feature values into dis- a fuzzy inference system that augmented pattern
crete events. In a training set, patterns of events discovery with fuzzy logic theory to yield a hybrid
across the features used to represent a MUP and system. Discretization error is greatly reduced be-
including a specific muscle category, which oc- cause values within a bin are assigned memberships
cur more often than expected under the assump- based on their continuous value. The “fuzziness” of
tion of independent features and categories, are membership values allows multiple rules with the
selected by pattern discovery as rules. The entire same feature value to be considered simultaneously,
set of discovered rules form a knowledge-based selecting the rule that yields the best discrimina-
system that can be used for the categorization of tion. Information presented in this way is also more
test MUPs. If a pattern of events created by the in line with the way humans interpret and reason
quantized feature values of a test MUP matches with data they are presented with, making it an ex-
a rule associated with a pattern discovered in the cellent candidate for use in decision support.
training data that occurred more often than ex-
pected, it is used as positive evidence and supports 4. Evaluation of MUP Characterization Tech-
the category contained in the rule. Alternatively, niques
if the matched rule is associated with a pattern
discovered in the training data that occurred less To be clinically useful, a classifier must meet cer-
often than expected, it is used as negative evidence tain requirements in addition to being accurate. A
and refutes the category contained in the rule. The more complete description of these requirements
degree of support or refutation is measured by the is presented in section III.A. One of the most im-
weight of evidence statistic.43 portant of these requirements is transparency (i.e.,
Volume 38, Number 5, 2010
474 Farkas et al
the ability for a clinician to understand the crite- and cannot be used in isolation for accurate diag-
ria used to make a specific classification decision). nosis. A more robust indicator can be achieved if
Conventional classifier methods are simplistic several MUP characterizations across a muscle are
enough that they may provide some level of trans- aggregated. During qualitative analysis, a clinician
parency to clinicians familiar with the concepts also aggregates, based on experience and training,
of differential diagnosis. However, these methods the information extracted from the MUPs and in-
have several drawbacks, such as unmet assumptions terference patterns examined to create an overall
regarding feature data distributions that can cause clinical impression of the muscle under examina-
the accuracy of these methods for MUP categori- tion. Unfortunately, the consistency and accuracy
zation to be quite poor. Advanced pattern recogni- of the clinical impression obtained is dependent on
tion techniques, such as artificial neural networks the experience of the clinician.
and support vector machines, are quite robust and
offer better performance. However, artificial neural 1. Statistical Muscle Characterization
networks are essentially “black-box” classifiers that
do not permit an explanation of their output. Even The most common method used to address the
if such an explanation were possible, it would not shortcomings of subjective qualitative interpre-
be in a form that is easily understood by a human tation is to use summary statistics of quantified
decision maker. Support vector machines also suf- MUP features. Statistical techniques go beyond
fer from complexity and require a deeper apprecia- simply summarizing quantitative data, and attempt
tion of their theoretical mechanisms. While pro- to characterize a muscle based on the distributions
viding accuracy comparable to other methods, the of their sampled MUP parameters. Such predictive
pattern discovery and fuzzy inference techniques analysis techniques form the basis of the early deci-
introduced by Pino and Hamilton-Wright offer a sion support techniques.13,14,18,19,44,45
completely transparent classification scheme. Pat- Common practice has been to calculate mean
tern discovery is unique in that it combines infor- values for morphological MUP features, such as
mation theoretic principles with linguistic inter- duration, amplitude, and number of phases across
pretation. At the heart of the method lies a robust sets of MUPs, and to compare them with normative
statistical and probabilistic analysis, but the rules standards reported in the literature to get a muscle-
derived from patterns in the data are in a form that level impression of the state of disease involve-
can be intuitively understood and easily displayed. ment. For example, the early works of Buchthal46
In addition, pattern discovery and fuzzy inference are still used as standards for formal quantization,
are capable of handling continuous and discrete and Podnar15-17,47-49 has published predictive values
feature values as well as missing data. Further, it is for limb, genioglossus, and anal sphincter muscles.
believed that the rule-based nature of pattern dis- Researchers have cited constraints on the mini-
covery allows it to generalize its conclusions to new mum number of motor units sampled in a muscle
data better than other classification techniques. (i.e., the preferred number of MUPs sampled for
robust diagnosis), and the general consensus is that
II.B. Muscle Characterization a minimum of 20 MUPs should be sampled.18,50
However, Podnar showed that sampling additional
Given the wide variability of MUPs detected in a MUPs can increase sensitivity and specificity.51
muscle dependent on the specific needle positions The major drawback with the statistical methods
during signal detection and the varying degrees to is that for each MUP feature, suitable threshold
which a disorder may affect specific motor units, values for defining normality/abnormality must be
individual MUP characterization scores are not established, as well as rules regarding the number
robust indicators of the actual category or state of of abnormal features required to declare a muscle
a muscle (i.e., myopathic, normal, or neurogenic) as abnormal.
Critical Reviews™ in Biomedical Engineering
A Review of Clinical QEMG 475
To implement a statistical method, a set of train- 2. Classifier-Based Muscle Characterization
ing data consisting of exemplary “normal” MUPs
is used to generate distributions for each feature. As an analog to MUP characterization, classifica-
Mean44 and/or outlier45 threshold values are then tion techniques have been applied to features that
defined, and feature values of a muscle under test are represent the entire muscle. For example, Xie et
classified based on their locations relative to these al.55 developed a multi-domain fusion strategy that
limits. For example, Stalberg used a mean norma- incorporates mean MUP morphological, frequen-
tive range of ±2 standard deviations and considered cy domain, and wavelet transform-based features.
three different outlier criteria: 95% confidence lim- Information from these domains is combined us-
its; 95% confidence limits for the third highest and ing fuzzy integral theory. Komur and Dobrowolski
third smallest values; and extreme upper and lower applied Fourier spectral analysis56,57 and classified
outlier limits. No appreciable difference was found wavelet coefficients from MUP scalograms.58 The
across these methods. A further strategy based on former has the advantage of providing a single diag-
this approach applies rules and heuristics13,19 to in- nostic parameter derived from the power spectrum
terpret the numbers of outliers and deviations from of the signal and does not require the onset and end
normal mean limits. Several works by Podnar52-54 locations of the MUPs to be accurately determined.
have performed comparisons of different outlier The latter method uses linear discriminant analysis
criteria and have established standardized norma- to reduce the number of wavelet based features to
tive limits for diagnostic criteria. two, transforming the decision space into a linear
The intention of QEMG analysis is to increase classification problem.
both sensitivity (number of correct positive deci-
sions) and specificity (number of correct negative 3. Probabilistic Muscle Characterization
decisions). For every decision, the objective is to
maximize sensitivity and specificity. However, sen- Statistical muscle characterizations have two main
sitivity and specificity cannot be simultaneously weaknesses: i) they are unable to provide a mea-
maximized. Therefore, with regard to the deci- sure of the quality of or confidence in a particular
sion-making process, whether it is better to be less inference, and ii) they use thresholds defined us-
specific in order to be more sensitive must first be ing averages and deviations across sets of MUPs
decided. Best practice is to determine the minimum (20 or more), making it difficult to investigate the
number of overall errors by balancing sensitivity and rationale for a particular result at the level of the
specificity unless the cost of poor sensitivity relative individual MUPs. Both of these weaknesses reduce
to specificity or vice versa can be determined. In this the transparency of decisions made. A probabilis-
regard, statistical muscle characterization methods tic approach addresses these weaknesses by pro-
have two main implementation issues. First, it is dif- viding information at the muscle level as well as
ficult to suitably define thresholds of normality/ab- the MUP level, thus allowing for the provision of
normality. Second, much confusion exists in deter- a detailed explanation of the underlying decision-
mining suitable categorization rules. For example, a making process. Recent work has applied pattern
rule might state that a minimum number of outliers recognition techniques to the probabilistic analysis
must be present to declare abnormality, but results of MUP features, and in some cases to features of
may vary depending on which features happen to composite EMG signals.11, 13,19,20,23,34-37,40,58,59 The
have outliers. On the other hand, a single feature term “characterization” in this sense takes on a more
might have sufficient evidence due to the number complex definition, but with the same end result as
of outlying MUPs. Such a feature may or may not described for statistical characterization. A proba-
fail the “mean” test depending on the distribution of bilistic characterization is one that assigns a score
its MUP feature values, but based on outlier criteria or likelihood measure to each muscle category un-
may clearly demonstrate abnormality. der consideration. Ideally, the score represents the
Volume 38, Number 5, 2010
476 Farkas et al
probability of the examined muscle being affected is uncertain of the outcome, this should be clearly
by a disease of a particular category conditioned by reflected in the characterization score, rather than by
the specific characteristics of the set of its sampled saturation in an incorrect category. The probabilistic
MUPs. A characterization is a set of n scores, where methodology has been compared to the statistical
n is number of muscle categories under consider- techniques of the previous section on several occa-
ation (typically 2 or 3). sions13,19,20,23 and has shown much promise.
a. Aggregating MUP Characterizations b. Measures of Confidence and Involvement
Despite the fact that MUPs can be characterized A muscle characterization score should reflect the
with high accuracy, there is a high degree of vari- probability that the muscle from which the MUPs
ability across MUP characterizations, even for were detected is actually of the given category, condi-
MUPs detected in the same normal muscle, there- tioned on the evidence provided by the set of MUP
by limiting their diagnostic potential. However, characterizations. In this way, a muscle character-
a robust muscle characterization can be obtained ization measure can be thought of as the confidence
by aggregating information across a set of MUPs in making a particular categorization based on the
detected from a muscle under test. An overall available evidence. A well-calibrated muscle confi-
muscle characterization is achieved by aggregating dence score of 80% for a given category means that,
the characterizations from individual MUPs. Just out of all the muscles that are assigned that score,
as in the MUP case, a score is produced for each 80% are truly of that category. It is therefore useful
category under consideration. The muscle is then to calibrate muscle scores to reflect true conditional
categorized as being from the category that has probabilities. One such calibration technique13 uses
the highest conditional probability score. A muscle Monte Carlo sampling39 to generate many variations
conditional probability can also be thought of as of the training data. These instances are then used
the confidence in a particular characterization. to calculate the actual probabilities associated with
Pfeiffer and Kunze11,12 first introduced the idea each score value. Curves fitted to these points can
of probabilistic characterization by using Bayes’ rule be used to transform subsequent test muscle scores
for multiple pieces of evidence to aggregate MUPs into well-calibrated conditional probabilities.
that were characterized using Fisher’s linear dis- When the arithmetic mean is used to aggregate
criminant analysis. Hamilton-Wright and Stashuk, MUP conditional probabilities, the conditional
using MUP characterizations created by a pattern probabilities representing a muscle characterization
discovery-based method modified to include fuzzy correlate well with the level of involvement of a dis-
inference, aggregated MUP characterizations using ease. In particular, the arithmetic mean aggregation
a fuzzy logic-based centroid calculation weighted method had a correlation of 0.9 using the Spearman’s
by the confidence of each MUP characterization.38 rank test.23 Although correlation is high, much dif-
Pino14,19 considered several aggregation metrics, ficulty lies in predicting the level of involvement due
including arithmetic mean, Bayes’ rule, and the z- to the fact that at lower levels of disease involvement,
transform.60 These metrics were used to aggregate the confidence in making a correct characterization
scores from several classifier methods (naive Bayes, is also low, resulting in greater variability and lower
linear discriminant analysis, pattern discovery, deci- accuracy in the measurement.
sion trees). All methods seem to provide a high level
of accuracy, with Bayes’ rule-based muscle charac- II.C. Accuracy of Characterization Methods
terization performing best. The muscle character-
ization scores generated using Bayes’ rule tend to The metrics used to evaluate MUP or muscle char-
saturate to 0 or 1 as more evidence (higher number acterization performance are greatly dependent on
of diseased MUPs) is presented, which is desirable the specific objectives and desired outcome of the
in most circumstances. However, when the classifier techniques in question. This makes it difficult to
Critical Reviews™ in Biomedical Engineering
A Review of Clinical QEMG 477
consistently compare the individual techniques. For of muscle categorization when using probabilistic
example, Katsis has done a considerable amount methods is significantly better than the accuracy of
of work to reduce the error in detecting diseased competing strategies. For example, the probabilistic
MUPs, and achieved overall accuracy values of 86% method achieved accuracies of 80% to 95% com-
to 88% and a disease-specific sensitivity of 85% to pared with 76% to 86% using statistical methods.19
99%.36,37 However, the MUPs used in these stud- Other studies have demonstrated accuracies of 59%
ies were characterized and annotated by an expert, (37% improvement over conventional) using linear
thus focusing mainly on pattern recognition aspects discriminant analysis and Bayes’ rule aggregation,59
of the problem. and 95% to 98% using advanced pattern recogni-
In contrast to this approach, probabilistic tion techniques,33 while in one case only a slight
methods use the true label of the muscle that the improvement was observed (60% vs. 66%).13
MUPs were extracted from as the class label for Studies by Pino and others13,19,23,40 have shown
classifier training and performance evaluation. The that several commonly used classification tech-
difficulty of this approach is that there is a great niques perform comparably with regard to MUP
deal of ambiguity in the interpretation of MUPs categorization and do not impact the overall muscle
detected from a muscle, because MUPs represent- categorization outcome significantly. However, they
ing each of the clinical disease states (normal, do affect the conditional probability estimates that
myopathic, neurogenic) can be detected from any make up the muscle characterization vector. The low
muscle regardless of its condition.11 This ambiguity accuracies obtained are mainly a result of the over-
is due to several factors such as the variability of lap of MUP feature value distributions mentioned
needle position and muscle structure or composi- previously, rather than of poor classifier design or
tion. As such, single MUP categorization accuracy feature selection. By aggregating MUP character-
is rather poor by comparison and in the range of izations, an overall decision can be made by taking
60% to 70%40; therefore, discussing the accuracy of into account evidence that is representative of the
MUP categorization in this manner will produce entire muscle. Depending on the aggregation strat-
poor results compared with the methods men- egy used, such methods can either be conservative,
tioned above, but MUP categorization is not the focusing on the level of agreement between MUP
main goal. Rather, it is the distribution of MUPs categorizations, or extremist by weighting outlier
from each of the clinical states being studied that MUPs (MUPs with a high likelihood for a given
provides valuable information, in a probabilistic disease category) more heavily.
sense, about the likelihood of a disease, its level In either case, a decision based on multiple
of involvement, and the confidence in this assess- pieces of evidence is shown to be superior in terms
ment. Muscle characterization methods must con- of muscle characterization performance, despite
sider the confusion created by MUPs that have its low classifier performance at the MUP level.
a high likelihood of belonging to more than one Therefore, it is not so much the predicted category
disease state, and it is this information, in contrast (categorization) assigned to an MUP that is rel-
to highly confident MUP characterizations, that evant, but rather the MUP characterization vec-
makes it possible to properly categorize a muscle. tor that describes the probabilities of a particular
Evaluating the performance of muscle character- disease conditioned on the features of the detected
ization techniques must therefore be done at the MUP. The aggregation of several of these MUP
muscle level after combining the individual MUP characterizations provides a robust representation
characterizations, and their performance must be of the clinical state of the muscle. Furthermore,
compared against other techniques designed to the method of MUP aggregation used to obtain
achieve a similar goal (i.e., statistical muscle char- a muscle characterization, combined with a trans-
acterization, EMG signal characterization, etc.). parent MUP characterization technique, forms the
Numerous studies have shown that the accuracy basis for clinical decision support.
Volume 38, Number 5, 2010
478 Farkas et al
III. CLINICAL DECISION SUPPORT are able to interpret heterogeneous, fluctuating
data and are able to capture time-varying clinical
Numerous methods of analyzing and interpreting parameters as well as predict the course of disease
data to provide decision support have been report- progression. Revett et al.62 developed a system for
ed, particularly in the medical field, in which large breast cancer diagnosis by combining “rough sets”
amounts of disparate data are analyzed and amal- and neural networks, and Gevaert et al.63 developed
gamated to make critical and time-sensitive deci- a breast cancer prediction scheme based on Bayes-
sions. One of the most important aspects of a clini- ian networks that combines high-dimensional
cal decision support system is its ability to combine microarray data with clinical findings. In the field
two important (and sometimes conflicting) capa- of pulmonary diseases, Economou et al.64 initially
bilities: the ability to characterize consistently and used artificial neural networks in a decision support
accurately make a prediction and the ability to system and then developed a knowledge base mod-
explain that prediction in a manner that is easily eled after the methodology used by physicians for
understood by a decision maker. The statistical and clinical differential diagnosis to provide decision
probabilistic characterization techniques discussed support.65
in the previous section can be used in a decision
support framework to present the vast amounts of III.A. Requirements for Clinical Decision
information obtained from QEMG analysis in a Support
clinically useful and relevant fashion.
The prevalence of clinical decision support Attempts have been made to formalize the re-
systems in medicine is growing exponentially, quirements of a clinical decision support system.
and systems have been proposed both in the field Such requirements are intended to guide the de-
of neuromuscular disease18,19,61 and in diagnostic velopment and evaluation of future systems. The
medicine in general.61-65 For example, the MUNIN works of Konokenko and Sprogar68,69 and a later
system66 uses Bayesian networks to infer a disease summary by Pino14 have generated a list of require-
based on findings from clinical tests, examinations, ments for clinical decision support systems to be
and patient reports. A major limitation of this clinically useful and safe. These are: i) transparency,
system is that human medical expertise is required ii) accuracy, iii) a measure of confidence in deci-
to “train” the system by defining conditional prob- sion support provided, iv) a numeric or continuous
ability tables. A machine that can “learn” without characterization value or measure, v) the ability to
a great deal of user intervention would be an asset. handle mixed-mode and multivariate feature data;
The KANDID system61 uses logical operators and vi) the ability to generalize to new data, and vii) the
known rules to build a knowledge base. The system ability to handle missing features or data. In addi-
is used by making queries that are answered using tion, it is desirable to have a reasoning strategy and
first-order logic. The statistical muscle characteriza- flow of information that, even in an abstract way, is
tion techniques presented earlier18 can be used in a analogous to the cognitive processes and data as-
decision support framework to indicate the pres- similation strategies employed by a human decision
ence or absence of disease. By incorporating a set maker. This helps to establish trust in the system,
of known rules, the disease category (neurogenic or and provides a “consultative” approach rather than
myopathic) can also be specified. a simple statement of the facts.
In most clinical decision support systems, data
from multiple sources, such as clinical evaluations, III.B. Suitable Methods for QEMG-Based
imaging, and other medical tests, are used to achieve Clinical Decision Support
a more robust inference. For example, miniTUBA67
is a medical inference system based on dynamic The evaluation by Pino showed that the statisti-
Bayesian networks. Dynamic Bayesian networks cal methods (i.e., the means and outlier analysis of
Critical Reviews™ in Biomedical Engineering
A Review of Clinical QEMG 479
Stewart and Stalberg19,44,45) perform as well as the III.C. Examples of Clinical Decision Support
classifier-based and probabilistic methods.13,18 The
statistical methods are also quite intuitive in terms One advantage of the probabilistic muscle charac-
of explaining the decision support provided, mak- terization frameworks proposed by Pinot14 is the
ing them useful for presentation purposes. How- ability to appreciate how each MUP template con-
ever, the statistical methods are not well suited for tributes to a muscle characterization and to explore
clinical decision support. They are not tractable to the rationale for this contribution. These methods
larger feature sets and are not able to provide a con- allow a decision maker to “drill down” from high
tinuous measure of confidence or degree of involve- levels of abstraction to detailed explanations.
ment. Similar arguments can also be made against Figure 2 is a visualization displaying MUP
most of the continuous classifier methods as well. characterizations obtained using a combined pat-
They may be quite robust, but they lack the needed tern discovery/fuzzy inference methodology38
transparency. In contrast, the probabilistic methods having several decision support components. At
meet the requirements for clinical decision support the top left of the display is the suggested muscle
presented above, particularly when implemented categorization (myopathic), and the confidence in
using pattern discovery and/or the fuzzy inference and conflict with this suggestion are presented at
frameworks. the top right. Below this are the individual MUP
Regardless of the specific inference techniques characterizations calculated from the EMG sig-
used, a fundamental component of decision sup- nals detected in the muscle under study. Each
port systems is the knowledge base or repository. component of each MUP characterization is plot-
The quality of inference made by the system greatly ted (point with tail) in a 2D plot representing the
depends on the nature of the data being defined assertion and confidence of the MUP character-
as exemplary. Therefore, exemplary data must first ization for its muscle category (myopathic, normal,
be acquired and stratified by an expert clinician. and neurogenic). Points with multiple tails repre-
Specifically, it must be acquired for each muscle or sent multiple MUP characterization components
groups of muscles studied, and should be stratified with the same assertion and confidence values. The
by age or any other relevant stratification criteria muscle characterization scores are calculated using
(e.g., gender). The physical architecture of a deci- a centroid calculation of MUP assertions weighted
sion support system with respect to its knowledge by their confidence measures, and are shown as a
base can take on several forms. For example, a colored circle in each respective muscle category
stand-alone system with its own repository of plot. The suggested muscle category corresponds
knowledge can provide a self-consistent defini- to the largest muscle characterization score. In
tion of clinical disease states based on acquisition the bottom-left corner, the MUP template and its
protocols and studies performed at a particular respective features of a selected MUP character-
clinic. In this case, the knowledge base would be ization are presented. Next to this, the assertion
built up by the users in that particular clinic, and and confidence of the selected MUP characteriza-
its use would be confined to that particular area tion are presented, along with the main patterns of
of expertise. Conversely, client-server architecture feature events used for their calculation. By select-
could be used to centralize the knowledge base ing different MUP characterizations, a decision
and promote consistency of gold standard data, but maker is able to “drill down” into the details of the
also to accommodate different detection protocols presented muscle characterizations. In addition,
from laboratory to laboratory. This type of frame- due to the fact that all of the MUP characteriza-
work would support collaboration of experts across tions are available, it is possible to show how the
clinics, would be useful for training students and data associated with each MUPT relate to all of
researchers, and could even support the diagnosis the other MUPTs sampled from the muscle be-
of patients in remote areas. ing examined. The collective display of the set of
Volume 38, Number 5, 2010
480 Farkas et al
FIGURE 2. Fuzzy inference-based muscle characterization.
MUP characterizations helps a decision maker to ues that occurred together as an nth-order pattern.
visualize the resultant muscle characterizations Patterns for or against each category are displayed
as well as its component MUP characterizations. with their x-position reflecting the level of asser-
This in turn allows a decision maker to appreciate tion or refutation provided by the respective rule.
the basis of, and confidence in, a suggested muscle The solid red bars represent the combined asser-
categorization. tion across all rules for a category. In this case, the
Figures 3 and 4 provide visualizations related evidence suggests that the muscle from which the
to MUP characterizations obtained using pattern MUPT was detected is likely myopathic, but also
discovery-based estimates of conditional probabil- possesses normal and neurogenic characteristics.
ity. Figure 3 presents individual MUP character- This confusion is driven by the presence of rules
izations as small pie charts, each of which is shown that provide evidence both for and against the
to contribute to the overall muscle characterization myopathic and neurogenic categories. Generally,
and level of involvement shown on the right. The higher order patterns provide a higher weight of
muscle characterization scores and involvement evidence and thus form the basis of the decision, in
percentages (using Bayes’ rule and autoregressive, this case showing strong support for the myopathic
respectively) for each category are represented by category and strong refutation of the neurogenic
large pie charts. Figure 4 shows the feature events category. A second-order rule is also present in
that underlie a single MUP characterization. The both the myopathic and neurogenic cases, provid-
plots on the bottom left provide a visual interpre- ing contrary evidence to the higher-order rule, but
tation of the rules generated by pattern discovery. to a much lesser degree. The amount of evidence
Each shape represents a discrete feature value, low is less convincing for the normal category (shown
(L), medium (M) or high (H), and shapes stacked by lower assertion values), but the presence of two
along the same vertical line represent feature val- separate rules bring the overall assertion farther to
Critical Reviews™ in Biomedical Engineering
A Review of Clinical QEMG 481
FIGURE 3. Probabilistic muscle characterization. The small pie charts on the left represent individual
MUP characterizations, the large pie chart at the top right represents muscle characterization, and the
large pie chart at the bottom right represents the estimated level of involvement.
the left. The overall characterization is still myo- characterization complete with a measure of con-
pathic, but not with a very high level of confidence fidence and the ability to see the distribution of
given the conflicting evidence. In Figure 4, in the MUP characterizations, as well as the ability to
right column are plots of the distributions of the “drill down” into the details of the individual MUP
values for each feature. The three bins used for characterizations. These examples demonstrate the
quantization (L, M, H) are demarcated, and green advantages of using transparent decision support
and red bars represent the normal and abnormal systems for QEMG.
ranges for each feature value. The white bar and
plot represent the feature value and distribu- IV. SUMMARY
tion of feature values for the MUP template and
MUP template set, respectively. Figures 3 and 4 The concepts and methods applied to quantitatively
again demonstrate the ability of the probabilistic use clinically detected needle EMG signals to pro-
methods to provide a quantitative overall muscle vide decision support related to the diagnosis, treat-
Volume 38, Number 5, 2010
482 Farkas et al
FIGURE 4. Probabilistic muscle characterization. Details of a specific MUP characterization with support
for the myopathic category are shown.
ment, and management of neuromuscular disorders development of more clinically useful methods of
have been reviewed. The fundamental basis for the quantitative analysis of needle EMG signals.
clinically relevant information present in needle In summary, QEMG assessment in general
EMG signals has been described. Methods for the provides several benefits in terms of analytical
quantitative analysis (characterization) of individu- strength and reproducibility. Many of the benefits
al MUPs with the objective of providing evidence of QEMG methods stem from the underlying fact
regarding the clinical state of the muscle under that once a reproducible system of measurement is
examination have been described and compared. constructed, integration of new data into that sys-
Methods for aggregating information from a set of tem is straightforward.
MUPs detected in the muscle under examination QEMG methods provide a starting point for
to obtain a characterization of the clinical state of a discussion of which features individually may be
the muscle have also been described and compared. used to identify and characterize EMG signals, as
Finally, the requirements of a clinical decision sup- well as the utility of feature combinations.
port system have been presented and the suitability The variety of tools available to support infer-
of the various muscle characterization methods for ence based on QEMG data is large and growing.
clinical decision support has been compared and The subtlety of inference that QEMG analysis cur-
examples of decision support methods shown. This rently supports is already quite impressive, and can
review demonstrates the progress made toward the be expected to improve in the future.
Critical Reviews™ in Biomedical Engineering
A Review of Clinical QEMG 483
REFERENCES 12. Pfeiffer G. The diagnostic power of motor unit
potential analysis: An objective Bayesian ap-
1. Stalberg EV, Falck B. The role of electromyog- proach. Muscle Nerve. 1999;22(5):584–91.
raphy in neurology. Electroencephalogr Clin 13. Pino L, Stashuk D, Podnar S. Bayesian char-
Neurophysiol. 1997;103(6):579–98. acterization of external anal sphincter mus-
2. Gazzoni M, Farina D, Merletti R. A new cles using quantitative electromyography. Clin
method for the extraction and classification Neurophysiol. 2008;119(10):2266–73.
of single motor unit action potentials from 14. Pino L. Neuromuscular clinical decision sup-
surface EMG signals. J Neurosci Methods. port using motor unit potentials characterized
2004;136(2):165–77. by ‘pattern discovery’ [dissertation]. Waterloo,
3. Merletti R, Farina D. Analysis of intramuscu- Ontario, Canada: University of Waterloo; 2009.
lar electromyogram signals. Philos Transact A 15. Podnar S. Predictive values of motor unit po-
Math Phys Eng Sci. 2009;367(1887):357–68. tential analysis in limb muscles. Clin Neuro-
4. Holobar A, Minetto MA, Botter A, Negro F, physiol. 2009;120(5):937–40.
Farina D. Experimental analysis of accuracy 16. Podnar S, Mrkaić M. Predictive power of mo-
in the identification of motor unit spike trains tor unit potential parameters in anal sphincter
from high-density surface EMG. IEEE Trans electromyography. Muscle Nerve. 2002;26(3):
Neural Syst Rehabil Eng. 2010;18(3):221–9. 389–94.
5. Stashuk D, Brown W. Quantitative electro- 17. Podnar S. Predictive values of the anal sphinc-
myography. In: Brown WF, Bolteon C, Ami- ter electromyography. Neurourol Urodyn.
noff M, editors. Neuromuscular function and 2009;28(8):1034–5.
disease: basic, clinical, and electrodiagnostic 18. Stålberg E, Bischoff C, Falck B. Outliers, a way
aspects. Philadelphia: WB Saunders; 2002. p. to detect abnormality in quantitative EMG.
311–48. Muscle Nerve. 1994;17(4):392–9.
6. Stashuk DW. Decomposition and quantitative 19. Pino L, Stashuk D, Boe S, Doherty T. Proba-
analysis of clinical electromyographic signals. bilistic muscle characterization using QEMG:
Med Eng Phys. 1999; 21(6-7):389–404. Application to neuropathic muscle. Muscle
7. Stashuk D. EMG signal decomposition: how Nerve. 2010;41(1):18–31.
can it be accomplished and used? J Electro- 20. Hamilton-Wright A, McLean L, Stashuk DW,
myogr Kinesiol. 2001;11(3):151–73. Calder KM. Bayesian aggregation versus major-
8. Doherty TJ, Stashuk DW. Decomposition- ity vote in the characterization of non-specific
based quantitative electromyography: Meth- arm pain based on quantitative needle electro-
ods and initial normative data in five muscles. myography. J Neuroeng Rehabil. 2010;7:8.
Muscle Nerve. 2003;28(2):204–11. 21. Wijnberg ID, van Dam KG, Graaf-Roelfsema
9. McGill KC, Lau K, Dorfman LJ. A compari- E, Keizer HA, van Ginneken MM, Barneveld
son of turns analysis and motor unit analysis A, Breda E, van der Kolk JH. (Over)training
in electromyography. Electroencephalogr Clin effects on quantitative electromyography and
Neurophysiol. 1991;81(1):8–17. muscle enzyme activities in standardbred hors-
10. McGill KC, Lateva ZC, Marateb HR. es. J Appl Physiol. 2008;105(6):1746–53.
EMGLAB: An interactive EMG decom- 22. Daube JR, Rubin DI. Needle electromyogra-
position program. J Neurosci Methods phy. Muscle Nerve. 2009;39(2):244–70.
2005;149(2):121–33. 23. Pino LJ, Stashuk DW. Using motor unit po-
11. Pfeiffer G, Kunze K. Discriminant classifi- tential characterizations to estimate neuro-
cation of motor unit potentials (MUPs) suc- muscular disorder level of involvement. Conf
cessfully separates neurogenic and myopathic Proc IEEE Eng Med Biol Soc. 2008;2008:
conditions. A comparison of multi- and uni- 4138–41.
variate diagnostical algorithms for MUP anal- 24. Preston D, Shapiro B. Needle electromyogra-
ysis. Electroencephalogr Clin Neurophysiol. phy fundamentals, normal and abnormal pat-
1995; 97(5):191–207. terns. Neurol Clin. 2002;20:361–96.
Volume 38, Number 5, 2010
484 Farkas et al
25. Sonoo M. New attempts to quantify concen- method for MUAP classification based on
tric needle electromyography. Muscle Nerve. EMG decomposition. Comput Biol Med.
2002;25(S11):S98–102. 2007;37(9):1232–40.
26. Zalewska E, Hausmanowa-Petrusewicz I. 38. Hamilton-Wright A, Stashuk D. Clinical Char-
The SIIR index--a non-linear combination of acterization of Electromyographic Data Using
waveform size and irregularity parameters for Computational Tools. Conf. Proc. IEEE Com-
classification of motor unit potentials. Clin putational Intelligence and Bioinformatics and
Neurophysiol. 2005;116(4):957–64. Computational Biology (CIBCB 2006); 2006;
27. Zalewska E, Hausmanowa-Petrusewicz I, 2006:1–7.
Stålberg E. Modeling studies on irregular 39. Duda RO, Hart PE, Stork DG. Pattern classi-
motor unit potentials. Clin Neurophysiol. fication. 2nd ed. New York: Wiley-Interscience;
2004;115(3):543–56. 2000.
28. Stålberg E, Trontelj JV. The study of normal 40. Pino L, Stashuk D, Boe S, Doherty T. Motor
and abnormal neuromuscular transmission unit potential characterization using “pattern
with single fibre electromyography. J Neurosci discovery”. Med. Eng Phys. 2008;30(5):563–73.
Methods. 1997;74(2):145–54. 41. Schizas CN, Middleton LT, Pattichis CS. Neu-
29. Parsaei H, Stashuk D W, Rasheed S, Farkas ral network models in EMG diagnosis. IEEE
C, Hamilton-Wright A. Intramuscular EMG Trans Biomed Eng. 1990;42(5):486–96.
signal decomposition. Crit Rev Biomed Eng. 42. Quinlan JR. C4.5: Programs for machine learn-
2010;435–65. ing. 1st ed. San Francisco: Morgan Kaufmann;
30. Parsaei H, Nezhad FJ, Stashuk D, Hamilton- 1992.
Wright. Development of an SVM classifier for 43. Wong AKC, Wang Y. High-order pattern dis-
detecting merged motor unit potential trains. covery from discrete-valued data. IEEE Trans.
Proceedings of the XVII th Congress of ISEK, Knowl. Data Eng. 1997;9(6):877-893.
June 18 – 21, Niagara Falls, Canada; 2008. 44. Stewart CR, Nandedkar SD, Massey JM, Gil-
31. Parsaei H, Nezhad F, Stashuk D, Hamilton- christ JM, Barkhaus PE, Sanders DB. Evalua-
Wright A. Validation of motor unit potential tion of an automatic method of measuring fea-
trains using motor unit firing pattern infor- tures of motor unit action potentials. Muscle
mation. Conf Proc IEEE Eng Med Biol Soc. Nerve. 1989;12(2):141–8.
2009;2009:974–7. 45. Stålberg E, Stålberg S, Melander M, Arimura
32. Parsaei H, Stashuk D. MUP shape-based vali- K. A personal computer based system used in
dation of a motor unit potential train. Conf Proc electromyography for interpretation and re-
IEEE Eng Med Biol Soc. 2009;2009:2551–4. porting. Comput Methods Programs Biomed.
33. Christodoulou C, Pattichis C. Unsupervised 1991;34(2-3):219–27.
pattern recognition for the classification of 46. Buchthal F, Pinell P, Rosenfalck P. Action po-
EMG signals. IEEE Trans Biomed Eng. tential parameters in normal human muscle
1999;46(2):169–78. and their physiological determinants. Acta
34. Pattichis CS, Pattichis MS. Time-scale analy- Physiol Scand. 1954;32(2–3):219–29.
sis of motor unit action potentials. IEEE Trans 47. Podnar S, Vodusek DB. Standardisation of
Biomed Eng. 1999;46(11):1320–9. anal sphincter EMG: high and low threshold
35. Pattichis CS, Elia AG. Autoregressive and motor units. Clin Neurophysiol. 1999;110(8):
cepstral analyses of motor unit action poten- 1488–91.
tials. Med Eng Phys. 1999;21(6–7):405–19. 48. Podnar S, Vodusek DB. Standardization of anal
36. Katsis C, Goletsis Y, Likas A, Fotiadis D, Sar- sphincter electromyography: uniformity of the
mas I. A novel method for automated EMG de- muscle. Muscle Nerve. 2000;23(1):122–5.
composition and MUAP classification. Artificial 49. Podnar S, Vodusek DB. Standardization of
Intelligence in Medicine. 2006;37(1):55–64. anal sphincter electromyography: utility of mo-
37. Katsis CD, Exarchos TP, Papaloukas C, Go- tor unit potential parameters. Muscle Nerve.
letsis Y, Fotiadis DI, Sarmas I. A two-stage 2001;24(7):946–51.
Critical Reviews™ in Biomedical Engineering
A Review of Clinical QEMG 485
50. Podnar S, Mrkaić M. Size of motor unit po- A, Rønager J, Petrera J, Stigsby B, Willison RG,
tential sample. Muscle Nerve. 2003;27(2): et al. KANDID an EMG decision support sys-
196–201. tem evaluated in a European multicenter trial.
51. Podnar S. Usefulness of an increase in size of Muscle Nerve. 1993;16(5):520–9.
motor unit potential sample. Clin Neurophysi- 62. Revett K, Gorunescu F, Gorunescu M, El-
ol. 2004;115(7):1683–8. Darzi E, Ene M. A hybrid breast cancer di-
52. Podnar S. Criteria for neuropathic abnormality agnosis system: a combined approach using
in quantitative anal sphincter electromyogra- rough sets and probabilistic neural networks.
phy. Muscle Nerve. 2004;30(5):596–601. Conf. Proc. IEEE Int. Conf. on “Computer as
53. Podnar S. Comparison of different outlier crite- a tool”-Eurocon 2005, Belgrade, Serbia, 2005;
ria in quantitative anal sphincter electromyogra- 2005: 1124- 1127.
phy. Clin Neurophysiol. 2005;116(8):1840–5. 63. Gevaert O, De Smet F, Timmerman D,
54. Podnar S. Comparison of parametric and non- Moreau Y, De Moor B. Predicting the prog-
parametric reference data in motor unit poten- nosis of breast cancer by integrating clinical
tial analysis. Muscle Nerve. 2008;38(5):1412–9. and microarray data with Bayesian networks.
55. Xie H, Huang H, Wang Z. Multiple feature Bioinformatics. 2006;22(14):e184–90.
domains information fusion for computer-aid- 64. Economou GP, Lymberopoulos D, Karavatsel-
ed clinical electromyography. In: Gagalowicz ou E, Chassomeris C. A new concept toward
A, Philips W, editors. Computer analysis of im- computer-aided medical diagnosis--a proto-
ages and patterns. Berlin/Heidelberg: Springer; type implementation addressing pulmonary
2005. p. 304–12. diseases. IEEE Trans Inf Technol Biomed.
56. Dobrowolski A, Tomczykiewicz K, Komur P. 2001;5(1):55-66.
Spectral analysis of motor unit action poten- 65. Economou G, Goumas P, Spiropoulos K. A
tials. IEEE Trans Biomed Eng. 2007;54(12): novel medical decision support system. J Com-
2300–2. put Control Eng. 1996;7(4):177–83.
57. Komur P, Dobrowolski AP, Dabrowski T, Tom- 66. Suojanen M, Andreassen S, Olesen KG.
czykiewicz K. Automated diagnostic method A method for diagnosing multiple diseas-
supporting EMG examination. Conf Proc es in MUNIN. IEEE Trans Biomed Eng.
IEEE Eng Med Biol Soc. 2008;2008:1116–9. 2001;48(5):522–32.
58. Dobrowolski AP, Jakubowski J, Tomczykiewicz 67. Xiang Z, Minter RM, Bi X, Woolf PJ, He Y.
K. Linear discriminant analysis of MUAP sca- miniTUBA: medical inference by network in-
lograms. Conf Proc IEEE Eng Med Biol Soc. tegration of temporal data using Bayesian anal-
2008;2008:1100–3. ysis. Bioinformatics. 2007;23(18):2423–32.
59. Pfeiffer G. The diagnostic power of motor unit 68. Kononenko I. Machine learning for medical
potential analysis: an objective bayesian ap- diagnosis: history, state of the art and perspec-
proach. Muscle Nerve. 1999;22(5):584–91. tive. Artif Intell Med. 2001;23(1):89–109.
60. Whitlock MC. Combining probability from 69. Šprogar M, Lenič M, Alayon S. Evolu-
independent tests: the weighted Z-method tion in medical decision making. J Med Syst.
is superior to Fisher’s approach. J Evol Biol. 2002;26(5):479–89.
2005;18(5):1368–73.
61. Fuglsang-Frederiksen A, Johnsen B, Vingtoft
S, Rønager J. Vingtoft S, Fuglsang-Frederiksen
Volume 38, Number 5, 2010
You might also like
- SDG Business Reporting Analysis 2022Document559 pagesSDG Business Reporting Analysis 2022ComunicarSe-ArchivoNo ratings yet
- Animal Protection Reiki PDFDocument6 pagesAnimal Protection Reiki PDForlatan100% (1)
- Chiropractic & Osteopathy: On The Reliability and Validity of Manual Muscle Testing: A Literature ReviewDocument23 pagesChiropractic & Osteopathy: On The Reliability and Validity of Manual Muscle Testing: A Literature ReviewEdgardo BivimasNo ratings yet
- Emergency Nursing: By: Keverne Jhay P. ColasDocument61 pagesEmergency Nursing: By: Keverne Jhay P. ColasGaras AnnaBerniceNo ratings yet
- LamaDocument3 pagesLamarockyNo ratings yet
- Quantitative MRI of the Spinal CordFrom EverandQuantitative MRI of the Spinal CordJulien Cohen-AdadNo ratings yet
- Patient Registration Form 29Document8 pagesPatient Registration Form 29Cahayastore CahayastoreNo ratings yet
- Hydra Facial Machine PDFDocument11 pagesHydra Facial Machine PDFAarifNo ratings yet
- Dysrhythmia Advance Content Outline A1 - 2020.1.2Document3 pagesDysrhythmia Advance Content Outline A1 - 2020.1.2Kimberly Whiteside50% (2)
- Unique Point Japanese AcupunctureDocument12 pagesUnique Point Japanese Acupuncturepustinikki100% (4)
- The Use of Surface EMG in Biomechanics PDFDocument38 pagesThe Use of Surface EMG in Biomechanics PDFMarshall BananaNo ratings yet
- Muscle and Nerve - 2013 - Abdelmaseeh - Feature Selection For Motor Unit Potential Train CharacterizationDocument11 pagesMuscle and Nerve - 2013 - Abdelmaseeh - Feature Selection For Motor Unit Potential Train CharacterizationChengyiNo ratings yet
- Medical Decision Support System For DiagDocument29 pagesMedical Decision Support System For DiagIuri SampaioNo ratings yet
- SV2021112102Document12 pagesSV2021112102pashaNo ratings yet
- Single Channel EMG Classification With Ensemble Empirical Mode Decomposition Based ICA For Diagnosing Neuromuscular DisordersDocument10 pagesSingle Channel EMG Classification With Ensemble Empirical Mode Decomposition Based ICA For Diagnosing Neuromuscular DisordersRama BayuNo ratings yet
- NormativeDocument9 pagesNormativeEdher PliegoNo ratings yet
- 191 ModifiedDocument4 pages191 Modifiedqudrat zohirovNo ratings yet
- Applied Kinesiology Research Articles I Ak Research Compendium DR Scott Cuthbert 10-08-11 LatestDocument218 pagesApplied Kinesiology Research Articles I Ak Research Compendium DR Scott Cuthbert 10-08-11 LatestMOTION ARGENTINANo ratings yet
- Cerebal PalsyDocument10 pagesCerebal PalsySoffie FitriyahNo ratings yet
- Train - Sensorimotor System Measurement TechniquesDocument14 pagesTrain - Sensorimotor System Measurement TechniquesEdher Pliego100% (1)
- Lower Limb Analysis of The Biomechanical Gait Cycle at Various Phases in Real TimeDocument12 pagesLower Limb Analysis of The Biomechanical Gait Cycle at Various Phases in Real Timeمدرس مساعد هدى فاروق جميلNo ratings yet
- Muscle Force Estimation From Lower Limb EMG Signals Using Novel Optimised Machine Learning TechniquesDocument17 pagesMuscle Force Estimation From Lower Limb EMG Signals Using Novel Optimised Machine Learning Techniquesu5600291No ratings yet
- A Guide For Use and Interpretation of Kinesiologic Electromyographic Data PDFDocument13 pagesA Guide For Use and Interpretation of Kinesiologic Electromyographic Data PDFIgor Eduardo S. SouzaNo ratings yet
- Artificial Neural Network Learns Clinical Assessment of Spasticity in Modified Ashworth ScaleDocument9 pagesArtificial Neural Network Learns Clinical Assessment of Spasticity in Modified Ashworth ScalePrasasti 19No ratings yet
- Content: 2. Literature Survey 3. Problem Definition 4. Objective 5. Methodology 6. ReferencesDocument10 pagesContent: 2. Literature Survey 3. Problem Definition 4. Objective 5. Methodology 6. ReferencesImran ShaikhNo ratings yet
- Sensors 14 12598Document25 pagesSensors 14 12598Afrizal SuhariNo ratings yet
- Alberts Et Al. - 2015 - Using Accelerometer and Gyroscopic Measures To QuaDocument11 pagesAlberts Et Al. - 2015 - Using Accelerometer and Gyroscopic Measures To QuaYouriDuchêneNo ratings yet
- Surface Electromyography Based Muscle Fatigue Detection Using High-Resolution Time-Frequency Methods and Machine Learning AlgorithmsDocument12 pagesSurface Electromyography Based Muscle Fatigue Detection Using High-Resolution Time-Frequency Methods and Machine Learning AlgorithmsCindy nnnNo ratings yet
- Assessment Muscle Fatigueusing Statistical Study AReviewDocument7 pagesAssessment Muscle Fatigueusing Statistical Study AReviewWeCareNo ratings yet
- Effect of Mirror Therapy Combined With Somatosensory Stimulation On Motor Recovery and Daily Function in Stroke Patients: A Pilot StudyDocument7 pagesEffect of Mirror Therapy Combined With Somatosensory Stimulation On Motor Recovery and Daily Function in Stroke Patients: A Pilot Studywanda argeNo ratings yet
- Journal of Electromyography and Kinesiology: Yumna Albertus-Kajee, Ross Tucker, Wayne Derman, Michael LambertDocument8 pagesJournal of Electromyography and Kinesiology: Yumna Albertus-Kajee, Ross Tucker, Wayne Derman, Michael LambertJuniorMartinsNo ratings yet
- Associating Functional Neural Connectivity and SpecificDocument14 pagesAssociating Functional Neural Connectivity and SpecificAarya RaghavanNo ratings yet
- La Aplicación Isocinética en La Prueba y Rehabilitación Del Complejo Del Hombro.Document13 pagesLa Aplicación Isocinética en La Prueba y Rehabilitación Del Complejo Del Hombro.Edher PliegoNo ratings yet
- Naeem 2019Document13 pagesNaeem 2019mariasol63No ratings yet
- Nerve Conduction Velocity StudiesDocument12 pagesNerve Conduction Velocity StudiessridharNo ratings yet
- A Systematic ReviewDocument17 pagesA Systematic Reviewjorgequintero927470No ratings yet
- Computer EmgDocument3 pagesComputer Emgemilio9fernandez9gatNo ratings yet
- SensorsDocument30 pagesSensorsJuan sebastian lopez escobarNo ratings yet
- Nazmi 2015Document6 pagesNazmi 2015u5600291No ratings yet
- Muscle Motor Point Identification Is Essential For Optimizing Neuromuscular Electrical Stimulation UseDocument6 pagesMuscle Motor Point Identification Is Essential For Optimizing Neuromuscular Electrical Stimulation UsestefanoNo ratings yet
- A Wavelet-Based Method To Predict Muscle Forces From Surface Electromyography Signals in WeightliftingDocument11 pagesA Wavelet-Based Method To Predict Muscle Forces From Surface Electromyography Signals in WeightliftingRommel AndresNo ratings yet
- Journal Pre-Proof: Clinical BiomechanicsDocument34 pagesJournal Pre-Proof: Clinical BiomechanicsZouhour MiladiNo ratings yet
- D.J. 2022 Msot and Peripheral NervesDocument29 pagesD.J. 2022 Msot and Peripheral NervesChadiIbrahimNo ratings yet
- Efects of Robot-Assited Therapy On Upper Limb Recovery After StrokeDocument17 pagesEfects of Robot-Assited Therapy On Upper Limb Recovery After StrokeLorena CabreraNo ratings yet
- BMC Musculoskeletal DisordersDocument9 pagesBMC Musculoskeletal DisordersRakheeNo ratings yet
- Sensors 20 02354Document16 pagesSensors 20 02354Anh HuyNo ratings yet
- Background: Baseline Pearson Correlation P-ValueDocument1 pageBackground: Baseline Pearson Correlation P-ValueRed Menni de Daño CerebralNo ratings yet
- Healthcare 10 00704 v3Document12 pagesHealthcare 10 00704 v3Nakarit SangsirinawinNo ratings yet
- Applsci 10 08662 v2Document21 pagesApplsci 10 08662 v2Voruganti PranayNo ratings yet
- Musculoskeletal Impairment RatingDocument4 pagesMusculoskeletal Impairment RatingRavikiran NandirajuNo ratings yet
- Smudging of The Motor Cortex Is Related To The Severity of Low Back PainDocument18 pagesSmudging of The Motor Cortex Is Related To The Severity of Low Back PainAugusto Felipe Benavides MejiasNo ratings yet
- Methodology of Surface Electromyography in Gait Analysis: Review of The LiteratureDocument8 pagesMethodology of Surface Electromyography in Gait Analysis: Review of The LiteraturemaketoNo ratings yet
- A Multiclassifier Approach of Emg Signal Classification For Diagnosis of Neuromuscular Disorders 2155 9538 1000S3 003Document6 pagesA Multiclassifier Approach of Emg Signal Classification For Diagnosis of Neuromuscular Disorders 2155 9538 1000S3 003Isma IbaNo ratings yet
- Electromyography (EMG) Based Classification of Neuromuscular Disorders Using Multi-Layer PerceptronDocument6 pagesElectromyography (EMG) Based Classification of Neuromuscular Disorders Using Multi-Layer PerceptronIsma IbaNo ratings yet
- AWJune19wholemag 39Document1 pageAWJune19wholemag 39BwizerNo ratings yet
- Medical Engineering & Physics: Jie LiuDocument5 pagesMedical Engineering & Physics: Jie LiuD4wFl1NNo ratings yet
- Observational Pilot Study of Patients With Carpal Tunnel Syndrome Treated With Nucleo CMP ForteDocument8 pagesObservational Pilot Study of Patients With Carpal Tunnel Syndrome Treated With Nucleo CMP ForteRicardo BarcoNo ratings yet
- EMG SignalDocument9 pagesEMG Signalbvkarthik2711No ratings yet
- Ak Research Doc723062011105245Document19 pagesAk Research Doc723062011105245Alberto BeskowNo ratings yet
- Identification Method of Human Movement Intention Based On The Fusion Feature of EEG and EMGDocument5 pagesIdentification Method of Human Movement Intention Based On The Fusion Feature of EEG and EMGjimmie_yagerNo ratings yet
- Assig 1Document4 pagesAssig 1aabilaNo ratings yet
- Velasco 2008Document9 pagesVelasco 2008moiNo ratings yet
- Bolgla 2007Document10 pagesBolgla 2007Cindy nnnNo ratings yet
- Kann Us 1994Document8 pagesKann Us 1994hs rezaeeNo ratings yet
- Dosagem Otima Musculo PDFDocument10 pagesDosagem Otima Musculo PDFJanaina PanizzaNo ratings yet
- MCQ AnswersDocument2 pagesMCQ AnswersJeyarajasekar TtrNo ratings yet
- An Upper-Limb Rehabilitation Exoskeleton System Controlled by MI Recognition Model With Deep Emphasized Informative FeaDocument12 pagesAn Upper-Limb Rehabilitation Exoskeleton System Controlled by MI Recognition Model With Deep Emphasized Informative Fea911205josephNo ratings yet
- Premio 20 DTDocument35 pagesPremio 20 DThyakueNo ratings yet
- Vensim Model IndexDocument4 pagesVensim Model Indexkaren dejoNo ratings yet
- Respiratory Physiology Mosby Physiology Series 2Nd Edition Edition Michelle M Cloutier All ChapterDocument67 pagesRespiratory Physiology Mosby Physiology Series 2Nd Edition Edition Michelle M Cloutier All Chaptervincent.pathak166100% (9)
- Asperger SyndromeDocument4 pagesAsperger SyndromeJonald AlvaranNo ratings yet
- Educational Commentary - Basic Vaginal Wet PrepDocument6 pagesEducational Commentary - Basic Vaginal Wet PrepAhmed MostafaNo ratings yet
- Database TCMDocument131 pagesDatabase TCMKartika Lee GunawanNo ratings yet
- Makabuhay IpDocument7 pagesMakabuhay IpButterflyCalmNo ratings yet
- Suppositories Phardose LectureDocument41 pagesSuppositories Phardose LecturePeter Paul RecaboNo ratings yet
- Figo Misoprostol IufdDocument0 pagesFigo Misoprostol IufdAntoni KurniawanNo ratings yet
- Understanding Cancer Treatment and OutcomesDocument5 pagesUnderstanding Cancer Treatment and OutcomesMr. questionNo ratings yet
- 11 - Management Post Operative Low Cardiac Output SyndromeDocument46 pages11 - Management Post Operative Low Cardiac Output SyndromeNat SNo ratings yet
- Opalescence Boost Whitening PDFDocument2 pagesOpalescence Boost Whitening PDFVikas AggarwalNo ratings yet
- BourkeDocument8 pagesBourkeMilan BursacNo ratings yet
- Minamata Mercury Diseases (Presentation)Document34 pagesMinamata Mercury Diseases (Presentation)thanes_kumar100% (4)
- OMFC Application RequirementsDocument1 pageOMFC Application RequirementshakimNo ratings yet
- 3 Pocket Size-CriminalisticsDocument77 pages3 Pocket Size-CriminalisticsCriminology Criminology CriminologyNo ratings yet
- Bladder IrrigationDocument19 pagesBladder IrrigationDwight Kristian CruzNo ratings yet
- Microbiology With Diseases by Taxonomy 6Th Edition Full ChapterDocument37 pagesMicrobiology With Diseases by Taxonomy 6Th Edition Full Chapterjoelle.yochum318100% (25)
- ZENICADocument72 pagesZENICAVedadNo ratings yet
- Individual Performance Commitment and Review (Ipcr) : Name of Employee: Approved By: Date Date FiledDocument12 pagesIndividual Performance Commitment and Review (Ipcr) : Name of Employee: Approved By: Date Date FiledTiffanny Diane Agbayani RuedasNo ratings yet
- Prof. Eman Rushdy Sulphonylurea A Golden Therapy For DiabetesDocument51 pagesProf. Eman Rushdy Sulphonylurea A Golden Therapy For Diabetestorr123No ratings yet
- Schizophrenia and Offending: Area of Residence and The Impact of Social Disorganisation and UrbanicityDocument17 pagesSchizophrenia and Offending: Area of Residence and The Impact of Social Disorganisation and UrbanicityMustafa ŠuvalijaNo ratings yet