You might also like
- The Prevention and Treatment of Disease with a Plant-Based Diet Volume 2: Evidence-based articles to guide the physicianFrom EverandThe Prevention and Treatment of Disease with a Plant-Based Diet Volume 2: Evidence-based articles to guide the physicianNo ratings yet
- Jurnal 1Document17 pagesJurnal 1Sabrina Firda FarahiyahNo ratings yet
- Variation in DKA Frequency at Type 1 Diabetes Diagnosis in Children WorldwideDocument17 pagesVariation in DKA Frequency at Type 1 Diabetes Diagnosis in Children WorldwideHilna ShalihaNo ratings yet
- Effect of Familial Diabetes Status and Age at Diagnosis On Type 2 Diabetes Risk: A Nation-Wide Register-Based Study From DenmarkDocument10 pagesEffect of Familial Diabetes Status and Age at Diagnosis On Type 2 Diabetes Risk: A Nation-Wide Register-Based Study From DenmarkrhmilazhariNo ratings yet
- Bmjopen 2011 000666Document6 pagesBmjopen 2011 000666Fabiola PortugalNo ratings yet
- Increased Risk of Severe DKA Among Ultra-Orthodox ChildrenDocument7 pagesIncreased Risk of Severe DKA Among Ultra-Orthodox Childrennoah87No ratings yet
- Dia Care-2014-Dall-3172-9Document8 pagesDia Care-2014-Dall-3172-9jcc3417No ratings yet
- Epidemiology - Diabetes and Kidney Disease PDFDocument12 pagesEpidemiology - Diabetes and Kidney Disease PDFSharyna EmyraNo ratings yet
- Evidence Links Oral Health to Heart Disease and DiabetesDocument10 pagesEvidence Links Oral Health to Heart Disease and DiabetesAristya Julianto SidhartaNo ratings yet
- The Economic Burden of Elevated Blood Glucose Levels in 2017: Diagnosed and Undiagnosed Diabetes, Gestational Diabetes, and PrediabetesDocument8 pagesThe Economic Burden of Elevated Blood Glucose Levels in 2017: Diagnosed and Undiagnosed Diabetes, Gestational Diabetes, and PrediabetesNersdilahNo ratings yet
- Predictive Factor of Ketoacidosis in Tyoe 1 Diabetes MelitusDocument6 pagesPredictive Factor of Ketoacidosis in Tyoe 1 Diabetes MelitusHilna ShalihaNo ratings yet
- OJEpi20120100001 48070885Document6 pagesOJEpi20120100001 48070885Riodian SaputraNo ratings yet
- Clinical Course of Diabetic Ketoacidosis in Hypertriglyceridemic Pancreatitis Pancreas 2015Document4 pagesClinical Course of Diabetic Ketoacidosis in Hypertriglyceridemic Pancreatitis Pancreas 2015América FloresNo ratings yet
- Prevalence of Depression and Associated Factors Among Adult Patients With Diabetes Mellitus Attending Diabetic Clinic at Kampala International University Teaching HospitalDocument11 pagesPrevalence of Depression and Associated Factors Among Adult Patients With Diabetes Mellitus Attending Diabetic Clinic at Kampala International University Teaching HospitalKIU PUBLICATION AND EXTENSIONNo ratings yet
- The Emergence of Non-Communicable Disease in Indonesia: Dyah PurnamasariDocument2 pagesThe Emergence of Non-Communicable Disease in Indonesia: Dyah Purnamasarinene_luciaNo ratings yet
- Incidence Trends of Type 1 and Type 2 Diabetes Among Youths, 2002-2012Document11 pagesIncidence Trends of Type 1 and Type 2 Diabetes Among Youths, 2002-2012Django BoyeeNo ratings yet
- Journal of Clinical & Translational Endocrinology: Original ResearchDocument11 pagesJournal of Clinical & Translational Endocrinology: Original ResearchAmparito SanchezNo ratings yet
- Gestational DiabetesDocument8 pagesGestational DiabetesNur WahyuningsihNo ratings yet
- Depression's Impact on Diabetes HealthcareDocument7 pagesDepression's Impact on Diabetes HealthcareLorand RusNo ratings yet
- Endoscopic Intervention and Cholecystectomy in Pregnant Women With Acute Biliary Pancreatitis Decreases Early ReadmissionsDocument19 pagesEndoscopic Intervention and Cholecystectomy in Pregnant Women With Acute Biliary Pancreatitis Decreases Early ReadmissionsCarlos Altez FernandezNo ratings yet
- Komplikasi DiabetesDocument4 pagesKomplikasi DiabetesFrans SaputraNo ratings yet
- Editorial: Complications of Diabetes 2017Document5 pagesEditorial: Complications of Diabetes 2017landoo oooNo ratings yet
- My Publication 2ndDocument6 pagesMy Publication 2ndAnjum FahadNo ratings yet
- Analgesic Use Parents Clan and Coffee Intake Are Three Independent Risk Factors of Chronic Kidney Disease in Middle and Elderly Aged Population ADocument7 pagesAnalgesic Use Parents Clan and Coffee Intake Are Three Independent Risk Factors of Chronic Kidney Disease in Middle and Elderly Aged Population AJackson HakimNo ratings yet
- Psychiatric and Medical Conditions in Transition-Aged Individuals With ASDDocument13 pagesPsychiatric and Medical Conditions in Transition-Aged Individuals With ASDLAURA CAMILA CACERES DELGADONo ratings yet
- Comorbid Diabetes and Hypertension: Gender - DifferencesDocument13 pagesComorbid Diabetes and Hypertension: Gender - DifferencesvinuthaNo ratings yet
- Pediatric Obesity and Gallstone Disease.18Document6 pagesPediatric Obesity and Gallstone Disease.18Merari Lugo OcañaNo ratings yet
- Journal Pre-Proof: The Journal of PediatricsDocument33 pagesJournal Pre-Proof: The Journal of Pediatricslaura_d_2No ratings yet
- (20493614 - Endocrine Connections) Association of Obesity With Diabetic Retinopathy in US Adults With Diabetes in A National SurveyDocument6 pages(20493614 - Endocrine Connections) Association of Obesity With Diabetic Retinopathy in US Adults With Diabetes in A National SurveyJoe SoNo ratings yet
- Am J Kidney Dis 2014 Oct 64 (4) 510Document24 pagesAm J Kidney Dis 2014 Oct 64 (4) 510hrol31060No ratings yet
- Prevalence of Diabetes and Impaired Fasting Glucose in Adults in The U.S. PopulationDocument6 pagesPrevalence of Diabetes and Impaired Fasting Glucose in Adults in The U.S. PopulationAndi BintangNo ratings yet
- Emergency Department Utilization by Californians With Sickle Cell Disease, 2005-2014Document6 pagesEmergency Department Utilization by Californians With Sickle Cell Disease, 2005-2014MateoZuluagaGomezNo ratings yet
- Prevalence of Diabetic Retinopathy Among Sioux IndiansDocument3 pagesPrevalence of Diabetic Retinopathy Among Sioux IndiansTrx AntraxNo ratings yet
- 1 s2.0 S126236362200074X MainDocument22 pages1 s2.0 S126236362200074X Mainwahyu kusumaNo ratings yet
- Journal of Diabetes and Clinical PracticeDocument7 pagesJournal of Diabetes and Clinical Practicebich truongNo ratings yet
- Jurnal 2 InterDocument9 pagesJurnal 2 InterYuni Amelia Putri 142No ratings yet
- Jurnal Media Keperawatan: Politeknik Kesehatan Makassar Vol. 08. No.02. 2017 E-Issn: 2622-0148, P-Issn: 2087-0035Document9 pagesJurnal Media Keperawatan: Politeknik Kesehatan Makassar Vol. 08. No.02. 2017 E-Issn: 2622-0148, P-Issn: 2087-0035Towo RottenNo ratings yet
- Frequency, Clinical Characteristics and Predictors of KetoacidosisDocument9 pagesFrequency, Clinical Characteristics and Predictors of KetoacidosisYogiPrimaZulkifliNo ratings yet
- Prevalence of Diabetes Mellitus Amongst Antenatal Clinic Attendees at Booking in A Teaching Hospital in Rivers State, NigeriaDocument3 pagesPrevalence of Diabetes Mellitus Amongst Antenatal Clinic Attendees at Booking in A Teaching Hospital in Rivers State, NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Epidemiology of Type 1 Diabetes Incidence and PrevalenceDocument17 pagesEpidemiology of Type 1 Diabetes Incidence and PrevalenceenrionickolasNo ratings yet
- Anthropometry Assessment in Children With Disease Related MalnutritionDocument10 pagesAnthropometry Assessment in Children With Disease Related Malnutritionberlian29031992No ratings yet
- Providing Diabetes Education To Patients With Chronic Kidney Disease: A Survey of Diabetes Educators in Ontario, CanadaDocument10 pagesProviding Diabetes Education To Patients With Chronic Kidney Disease: A Survey of Diabetes Educators in Ontario, CanadaKritik KumarNo ratings yet
- Dietary Knowledge Among Adults With Type 2 Diabetes-Kingdom of Saudi ArabiaDocument8 pagesDietary Knowledge Among Adults With Type 2 Diabetes-Kingdom of Saudi ArabiaMahmoud HakimNo ratings yet
- Characteristics of Patients With Type 2 Diabetes Mellitus at Surabaya Haji General HospitalDocument8 pagesCharacteristics of Patients With Type 2 Diabetes Mellitus at Surabaya Haji General Hospitaltiara cesariaNo ratings yet
- Economic and Survival Burden of Dysphagia Among Inpatients in The United StatesDocument7 pagesEconomic and Survival Burden of Dysphagia Among Inpatients in The United StatesClaudia Lorena MedinaNo ratings yet
- Diabetes, Pancreatogenic Diabetes, and Pancreatic CancerDocument8 pagesDiabetes, Pancreatogenic Diabetes, and Pancreatic CancerTeodoraManNo ratings yet
- ResearchDocument10 pagesResearchspadini putriNo ratings yet
- 10 1111@odi 13236Document10 pages10 1111@odi 13236vero alvarezNo ratings yet
- CKD Ska2Document14 pagesCKD Ska2Maya RustamNo ratings yet
- Wright2016 PDFDocument28 pagesWright2016 PDFMarco Alejandro RojasNo ratings yet
- jld150005 PDFDocument3 pagesjld150005 PDFAnonymous q9k297TG7HNo ratings yet
- Thiazolidinediones and Cardiovascular Outcomes in Older Patients With DiabetesDocument10 pagesThiazolidinediones and Cardiovascular Outcomes in Older Patients With Diabetesivel1506No ratings yet
- ADA Consenssus DM Eldery 2012Document15 pagesADA Consenssus DM Eldery 2012Jason CarterNo ratings yet
- Epidemiology Paper Final DraftDocument8 pagesEpidemiology Paper Final Draftapi-583311992No ratings yet
- Clinical Characteristics of Hyperglycemic Crises in Patients Without A History of DiabetesDocument6 pagesClinical Characteristics of Hyperglycemic Crises in Patients Without A History of DiabetesDewanggaWahyuPrajaNo ratings yet
- E20151662 FullDocument11 pagesE20151662 FullMichael OlaleyeNo ratings yet
- Richardson2021 Article L-typeCalciumChannelBlockerUseDocument9 pagesRichardson2021 Article L-typeCalciumChannelBlockerUsetrikusumaNo ratings yet
- Final Case - Ckd-To-DmnDocument56 pagesFinal Case - Ckd-To-DmnLovely Grace PoreNo ratings yet
- Association Between Health LiteraDocument8 pagesAssociation Between Health LiteraberthaNo ratings yet
- Consanguinity As A Significant Risk Factor For Diabetes Mellitus: A Systematic ReviewDocument8 pagesConsanguinity As A Significant Risk Factor For Diabetes Mellitus: A Systematic ReviewIJAR JOURNALNo ratings yet
- Cyanotic Congenital Heart Defects:: Practical Approach For PediatricianDocument25 pagesCyanotic Congenital Heart Defects:: Practical Approach For PediatricianYogiPrimaZulkifliNo ratings yet
- Hyperleukositosis: Bidasari Lubis-Olga Rasiyanti SiregarDocument26 pagesHyperleukositosis: Bidasari Lubis-Olga Rasiyanti SiregarYogiPrimaZulkifliNo ratings yet
- ABSENSI TAMPILAN Ilmiah 16 FEBRUARI 2022Document5 pagesABSENSI TAMPILAN Ilmiah 16 FEBRUARI 2022YogiPrimaZulkifliNo ratings yet
- DCIF EnglishDocument4 pagesDCIF EnglishKavsha GabaniNo ratings yet
- Antimicrobial Agen FixDocument3 pagesAntimicrobial Agen FixYogiPrimaZulkifliNo ratings yet
- Anaphylaxis: A 2020 Recommendation: Dr. Mahrani Lubis, M.Ked (Ped), Sp.A (K)Document19 pagesAnaphylaxis: A 2020 Recommendation: Dr. Mahrani Lubis, M.Ked (Ped), Sp.A (K)YogiPrimaZulkifliNo ratings yet
- 1 EARLY WARNING SYSTEM HOW TO RECOGNIZE THE CRITICALLY ILL PATIENTS-dr George PDFDocument43 pages1 EARLY WARNING SYSTEM HOW TO RECOGNIZE THE CRITICALLY ILL PATIENTS-dr George PDFYogiPrimaZulkifli100% (1)
- (Medical Masterclass) Coll.-Infectious Diseases and DermatologyDocument333 pages(Medical Masterclass) Coll.-Infectious Diseases and DermatologyVijay Mg100% (2)
- SalmonellaDocument27 pagesSalmonellaDayana PrasanthNo ratings yet
- Palpable Lymph Nodes Axillary: Signs and Symptoms of The Following Cancers: 1. Breast Cancer KidneyDocument4 pagesPalpable Lymph Nodes Axillary: Signs and Symptoms of The Following Cancers: 1. Breast Cancer KidneyJayNo ratings yet
- Fluid and Electrolyte TherapyDocument4 pagesFluid and Electrolyte TherapyKhirren RaoNo ratings yet
- MRSA Training For Student, Families and School Staff PPTDocument30 pagesMRSA Training For Student, Families and School Staff PPTSam TullyNo ratings yet
- JR 1 PutriiiDocument14 pagesJR 1 Putriiirahmat feryadiNo ratings yet
- ConditionalsDocument7 pagesConditionalsquynhnnp234101eNo ratings yet
- The Effect of Healthy Heart Gymnastics on Blood PressureDocument15 pagesThe Effect of Healthy Heart Gymnastics on Blood PressureAlisantoniNo ratings yet
- MANAJEMEN PENGENDALIAN PENYAKIT DEGENERATIF DI KELUARGADocument67 pagesMANAJEMEN PENGENDALIAN PENYAKIT DEGENERATIF DI KELUARGAHasriana TepuNo ratings yet
- PSYC 1111-01 Written Assignment Unit 7Document4 pagesPSYC 1111-01 Written Assignment Unit 7Muftaudeen Yusuf BabatundeNo ratings yet
- Annals of Medicine - HPV VaccineDocument12 pagesAnnals of Medicine - HPV VaccineJudicial Watch, Inc.100% (3)
- PAD Walking Impairment Questionnaire OverviewDocument4 pagesPAD Walking Impairment Questionnaire OverviewIoana Margineanu0% (1)
- 6 - FTT & FAS - MergedDocument25 pages6 - FTT & FAS - Mergedrenie3245No ratings yet
- HIRSCHSPRUNGDocument1 pageHIRSCHSPRUNGAezyreal Anne MirallesNo ratings yet
- Breast Duct Excision ML38861Document5 pagesBreast Duct Excision ML38861DrFeelgood WolfslandNo ratings yet
- Priority Nursing Diagnosis Rationale: PrioritizationDocument3 pagesPriority Nursing Diagnosis Rationale: PrioritizationJan Lianne BernalesNo ratings yet
- Vaccination Trends and Herd ImmunityDocument2 pagesVaccination Trends and Herd ImmunityYoshi NNo ratings yet
- Recommendations For Managing The Manifestations of Severe and Lifethreatening Mixed Cryoglobulinemia SyndromeDocument8 pagesRecommendations For Managing The Manifestations of Severe and Lifethreatening Mixed Cryoglobulinemia SyndromeNaty Barrios LaraNo ratings yet
- A Study To Assess The Prevalence of TattDocument5 pagesA Study To Assess The Prevalence of Tatt高權梁No ratings yet
- Nursing-Management A Respriotry Syncytial Bronchiolitis PDFDocument7 pagesNursing-Management A Respriotry Syncytial Bronchiolitis PDFAdarsh MuniNo ratings yet
- Nursing Care Plan HemorroidsDocument2 pagesNursing Care Plan Hemorroidsderic77% (22)
- Revised Thesis Proposal ASF Stricken Swine RaisersDocument24 pagesRevised Thesis Proposal ASF Stricken Swine RaisersPinky VirtudazoNo ratings yet
- Neck PainDocument2 pagesNeck PainMuhammed ElgasimNo ratings yet
- Croup, Bronchiolitis and Pneumonia Diagnosis and ManagementDocument43 pagesCroup, Bronchiolitis and Pneumonia Diagnosis and ManagementHaider Nadhem AL-rubaiNo ratings yet
- Complexity of Malaria Eradication in IndonesiaDocument9 pagesComplexity of Malaria Eradication in Indonesiairfanul_chakimNo ratings yet
- RNTCP - Wikipedia, The Free EncyclopediaDocument5 pagesRNTCP - Wikipedia, The Free EncyclopediaakurilNo ratings yet
- On The Job Form: Form 001/FRM/RISINT-CRI/I/2021Document2 pagesOn The Job Form: Form 001/FRM/RISINT-CRI/I/2021andeskum fcNo ratings yet
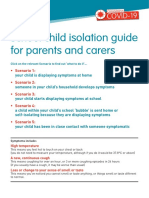
- Coronavirus school isolation guide for parentsDocument6 pagesCoronavirus school isolation guide for parentsMohammad TaNo ratings yet
- Laboratory Investigations in RheumatologyDocument43 pagesLaboratory Investigations in RheumatologyBahaa Shaaban100% (1)
- Epidemiology WholeDocument141 pagesEpidemiology WholeSonali SehrawatNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Recovering from Emotionally Immature Parents: Practical Tools to Establish Boundaries and Reclaim Your Emotional AutonomyFrom EverandRecovering from Emotionally Immature Parents: Practical Tools to Establish Boundaries and Reclaim Your Emotional AutonomyRating: 4.5 out of 5 stars4.5/5 (201)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)