You might also like
- ADSD Lab (BECL305) - 2022 Scheme 1st Cycle Experiments RSMDocument44 pagesADSD Lab (BECL305) - 2022 Scheme 1st Cycle Experiments RSMm1947asha100% (5)
- 2000 Paper 4 NovDocument8 pages2000 Paper 4 Novrajdeepghai5607No ratings yet
- Sachin - AA-Core ANSWERSDocument3 pagesSachin - AA-Core ANSWERSrajan shukla100% (2)
- Sandwich TechniqueDocument14 pagesSandwich TechniqueHarish KhundrakpamNo ratings yet
- [British Dental Journal 2014-may 23 vol. 216 iss. 10] Ngo, H._ Opsahl-Vital, S. - Minimal intervention dentistry II_ part 7. Minimal intervention in cariology_ the role of glass-ionomer cements in the preservat (201Document5 pages[British Dental Journal 2014-may 23 vol. 216 iss. 10] Ngo, H._ Opsahl-Vital, S. - Minimal intervention dentistry II_ part 7. Minimal intervention in cariology_ the role of glass-ionomer cements in the preservat (201كرم الباريNo ratings yet
- البحث الخامسDocument13 pagesالبحث الخامسMostafa Shaker El AasserNo ratings yet
- An In-Vitro Evaluation of MicroleakageDocument6 pagesAn In-Vitro Evaluation of MicroleakageDumitritaNo ratings yet
- 62 - The Open PDFDocument9 pages62 - The Open PDFSandeep Lal CherukaraNo ratings yet
- Porosity Formation and Microleakage of Composite Resins Using The Snowplow TechniqueDocument5 pagesPorosity Formation and Microleakage of Composite Resins Using The Snowplow TechniqueUnlikely QuestionsNo ratings yet
- Facial Slot Class II Restorations: A Conservative Technique RevisitedDocument5 pagesFacial Slot Class II Restorations: A Conservative Technique RevisitedAlyaa NabiilaNo ratings yet
- 2Document6 pages2Dey AzzNo ratings yet
- s40563 019 0118 7 PDFDocument13 pagess40563 019 0118 7 PDFXray PolyclinicNo ratings yet
- Rafter 2005Document7 pagesRafter 2005SindhuNo ratings yet
- Testing On Specimen - 6Document14 pagesTesting On Specimen - 6Dhruv ThakkarNo ratings yet
- Double Seal PDFDocument3 pagesDouble Seal PDFJitender Reddy100% (1)
- Effect of Conventional Adhesive Application or Co-Curing Technique On Dentin Bond StrengthDocument13 pagesEffect of Conventional Adhesive Application or Co-Curing Technique On Dentin Bond StrengthCarlos Andrés González RodríguezNo ratings yet
- JIntOralHealth94141-7129967 194819Document5 pagesJIntOralHealth94141-7129967 194819zaheerbdsNo ratings yet
- Microleakage in Class II Restorations: Open Vs Closed Centripetal Build-Up TechniqueDocument6 pagesMicroleakage in Class II Restorations: Open Vs Closed Centripetal Build-Up TechniquePutri MortezaNo ratings yet
- Sealers, Liners, and Bases: Contemporary IssuesDocument3 pagesSealers, Liners, and Bases: Contemporary IssuesD-F-093/Associate Professor/Dental Materials Dr. Shahreen ZahidNo ratings yet
- Comparative Evaluation of Microleakage in Class II Cavities Restored With Ceram X and Filtek P-90: An in Vitro StudyDocument6 pagesComparative Evaluation of Microleakage in Class II Cavities Restored With Ceram X and Filtek P-90: An in Vitro StudyRedhabAbbassNo ratings yet
- An Alkasite Restorative Material Effectively Remineralized Artificial Interproximal Enamel Caries in VitroDocument9 pagesAn Alkasite Restorative Material Effectively Remineralized Artificial Interproximal Enamel Caries in VitroJesus LugoNo ratings yet
- Wjoud 10 166Document4 pagesWjoud 10 166Bogdan HohaNo ratings yet
- Comparative Study of Resin Composite Class I RestoDocument9 pagesComparative Study of Resin Composite Class I RestoSholehudin Al AyubiNo ratings yet
- Cement, Nanohybrid Composite Resin Dan Resin BasedDocument1 pageCement, Nanohybrid Composite Resin Dan Resin BasedSherly PutriNo ratings yet
- Conventional and Adhesive Luting Cements PDFDocument8 pagesConventional and Adhesive Luting Cements PDFZahraa HamedNo ratings yet
- 1 PB PDFDocument5 pages1 PB PDFhanna asshabirinaNo ratings yet
- Alex - Direct Pulp Capping 2018Document7 pagesAlex - Direct Pulp Capping 2018Egidya Friezca ShafiraNo ratings yet
- Indirect Resin CompositesDocument12 pagesIndirect Resin CompositesJavier Istúriz Sijot100% (1)
- Evaluation of Two Different Materials For Pre-Endodontic Restoration of Badly Destructed TeethDocument7 pagesEvaluation of Two Different Materials For Pre-Endodontic Restoration of Badly Destructed TeethsrinandanNo ratings yet
- Improving Polymethyl Methacrylate Resin Using A Novel Titanium Dioxide CoatingDocument7 pagesImproving Polymethyl Methacrylate Resin Using A Novel Titanium Dioxide Coatingsilencer recnelisNo ratings yet
- Microleakage in Different Primary Tooth RestoratioDocument7 pagesMicroleakage in Different Primary Tooth RestoratioErtemNo ratings yet
- Comparison of The Sealing Ability of Bioceramic Sealer Against Epoxy ResinDocument8 pagesComparison of The Sealing Ability of Bioceramic Sealer Against Epoxy ResinViC JasonNo ratings yet
- The Influence of Different Composite Placement Techniques On Microleakage in Preparations With High C-FactorDocument5 pagesThe Influence of Different Composite Placement Techniques On Microleakage in Preparations With High C-FactordaconetubeNo ratings yet
- Review of Microleakage Evaluation ToolsDocument5 pagesReview of Microleakage Evaluation ToolsnisaNo ratings yet
- 18-Recycling of Fly Ash For Development of Value Added ProductsDocument9 pages18-Recycling of Fly Ash For Development of Value Added ProductsAli SherNo ratings yet
- Self-Healing of Concrete Cracks by Use of Bacteria-Containing Low Alkali Cementitious MaterialDocument14 pagesSelf-Healing of Concrete Cracks by Use of Bacteria-Containing Low Alkali Cementitious MaterialShaik HussainNo ratings yet
- Microleakage of Restorative Materials: An in Vitro Study: M P., D S., S ADocument4 pagesMicroleakage of Restorative Materials: An in Vitro Study: M P., D S., S Apreethi.badamNo ratings yet
- Effect of Microwave Disinfection On Dimensional Stability of Polymethyl Methacrylate and Polyamide Denture Base MaterialDocument5 pagesEffect of Microwave Disinfection On Dimensional Stability of Polymethyl Methacrylate and Polyamide Denture Base MaterialInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Espitia2013 ZnODocument10 pagesEspitia2013 ZnOParvinder KaurNo ratings yet
- A Comparative Study of Microleakage Between GiomerDocument5 pagesA Comparative Study of Microleakage Between GiomerJody ThiaNo ratings yet
- Pizza Technique in Site 1 Restoration in Lower Second Molar Tooth: A Case ReportDocument4 pagesPizza Technique in Site 1 Restoration in Lower Second Molar Tooth: A Case ReportKarissa NavitaNo ratings yet
- Closing Open Contacts Adjacent To An Implant-SuppoDocument3 pagesClosing Open Contacts Adjacent To An Implant-SuppoSeptimiu TiplicaNo ratings yet
- Investigation of Biodentine As Dentine Replacement MaterialDocument11 pagesInvestigation of Biodentine As Dentine Replacement MaterialOB RayinNo ratings yet
- 4 Articol Engleza CarioDocument7 pages4 Articol Engleza CarioAlexandraIoanaRășcanuNo ratings yet
- Wang 2014Document14 pagesWang 2014Coco Gonzales TorresNo ratings yet
- 2Document8 pages2Hamba AllahNo ratings yet
- Peel Bond Strength of Soft Lining Materials With Antifungal To A Denture Base Acrylic ResinDocument10 pagesPeel Bond Strength of Soft Lining Materials With Antifungal To A Denture Base Acrylic Resin165 - MUTHIA DEWINo ratings yet
- Recent Trends and Modifications in Glass Fibre Composites - A ReviewDocument7 pagesRecent Trends and Modifications in Glass Fibre Composites - A ReviewhiuNo ratings yet
- Jurnal Direct and Indirect Pulp CappingDocument9 pagesJurnal Direct and Indirect Pulp Cappingninis anisaNo ratings yet
- Direct and Indirect Pulp Capping: A Brief History, Material Innovations, and Clinical Case ReportDocument9 pagesDirect and Indirect Pulp Capping: A Brief History, Material Innovations, and Clinical Case ReportNaeimaNo ratings yet
- ContentServer Asp-2Document10 pagesContentServer Asp-2Lex Puma IdmeNo ratings yet
- Milani 2017Document4 pagesMilani 2017akshayNo ratings yet
- Bonding of Contemporary Glass Ionomer Cements To Different Tooth Substrates Microshear Bond Strength and Scanning Electron Microscope StudyDocument7 pagesBonding of Contemporary Glass Ionomer Cements To Different Tooth Substrates Microshear Bond Strength and Scanning Electron Microscope StudyAini Dwi HandiniNo ratings yet
- Articulo 2Document9 pagesArticulo 2SofiaNo ratings yet
- Testing On Specimen - 7Document17 pagesTesting On Specimen - 7Dhruv ThakkarNo ratings yet
- Bioceramics As Sealers in EndodonticsDocument6 pagesBioceramics As Sealers in EndodonticsShazeena QaiserNo ratings yet
- Pengaruh Aplikasi Liner Self Adhering Flowable Composite Terhadap Kebocoran Mikro Restorasi Resin Komposit Klas II (In Vitro)Document6 pagesPengaruh Aplikasi Liner Self Adhering Flowable Composite Terhadap Kebocoran Mikro Restorasi Resin Komposit Klas II (In Vitro)Andi ThatiaNo ratings yet
- Indirect Composite Inlay Restoration A Case ReportDocument6 pagesIndirect Composite Inlay Restoration A Case ReportgsgugsNo ratings yet
- Global Challenges - 2022 - Dinesh - Citric Acid Crosslinked Highly Porous Cellulose Nanofiber Foam Prepared by AnDocument10 pagesGlobal Challenges - 2022 - Dinesh - Citric Acid Crosslinked Highly Porous Cellulose Nanofiber Foam Prepared by AnLulu Aprilia DamayantiNo ratings yet
- 10 1002@pen 25078Document14 pages10 1002@pen 25078chemistpl420No ratings yet
- Comparison of Physical and Mechanical PropertiesDocument8 pagesComparison of Physical and Mechanical PropertiesSorour 2No ratings yet
- Nanobiomaterials in Clinical DentistryFrom EverandNanobiomaterials in Clinical DentistryKarthikeyan SubramaniRating: 5 out of 5 stars5/5 (1)
- Creating Super Dentin Using Flowable Composites As Luting Agents To Help Prevent Secondary CariesDocument10 pagesCreating Super Dentin Using Flowable Composites As Luting Agents To Help Prevent Secondary CariesGifix GifunNo ratings yet
- Colour Improvement and Stability of White Spot Lesions Following Infiltration, Microabrasion, or Fluoride Treatments in VitroDocument8 pagesColour Improvement and Stability of White Spot Lesions Following Infiltration, Microabrasion, or Fluoride Treatments in VitroGifix GifunNo ratings yet
- Guidance On Posterior Resin Composites Academy of Operative DentistryDocument7 pagesGuidance On Posterior Resin Composites Academy of Operative DentistryGifix GifunNo ratings yet
- Buonocore 1963 Retenção Adesiva e Materiais AdesivosDocument10 pagesBuonocore 1963 Retenção Adesiva e Materiais AdesivosGifix GifunNo ratings yet
- Rde 47 E15Document18 pagesRde 47 E15Gifix GifunNo ratings yet
- Claudius Ptolemy (Greece, 90-168) .CDocument4 pagesClaudius Ptolemy (Greece, 90-168) .CCandice Aberin Mag-alasinNo ratings yet
- Dissolution of Active Ingredient From Dosage FormDocument32 pagesDissolution of Active Ingredient From Dosage FormWira Wahyudi NandayasaNo ratings yet
- First Law of ThermodynamicsDocument205 pagesFirst Law of ThermodynamicsRaj Komol100% (1)
- Nehalem Intel PTU GuideDocument33 pagesNehalem Intel PTU GuideHiuenTsangNo ratings yet
- 19 Car Safety FeaturesDocument19 pages19 Car Safety FeaturesMohamed Siyad HassanNo ratings yet
- GeneralCatalogue ENGLISH (201105R11)Document28 pagesGeneralCatalogue ENGLISH (201105R11)Stuparu VictorNo ratings yet
- Bagas Ari Nugroho Skema Jaringan Warnet Dan ModemDocument18 pagesBagas Ari Nugroho Skema Jaringan Warnet Dan ModemAgung Agil SaputraNo ratings yet
- Chapter 6-State ManagementDocument79 pagesChapter 6-State ManagementHeng PhinNo ratings yet
- 3G4 Distillation CalculationsDocument22 pages3G4 Distillation Calculationsrkm_rkmNo ratings yet
- UniDac Update MultiDocument10 pagesUniDac Update Multianon_660430481No ratings yet
- Common Applications Utilizing A Spherical Roller BearingsDocument12 pagesCommon Applications Utilizing A Spherical Roller BearingsdynamicbearingNo ratings yet
- Mathematics Stage 4 Sample Paper 1 Mark Scheme - tcm142-594990Document14 pagesMathematics Stage 4 Sample Paper 1 Mark Scheme - tcm142-594990Danquah KumiNo ratings yet
- Buoyancy Shoe: (S.H.O.E)Document15 pagesBuoyancy Shoe: (S.H.O.E)Syed Izzat Hussain AlHussaini100% (1)
- Lecture 4 PDFDocument9 pagesLecture 4 PDFVarun SinghalNo ratings yet
- Project Documentation: File: Examen - Project Date: 16/06/2021 Profile: Codesys V3.5 Sp17Document9 pagesProject Documentation: File: Examen - Project Date: 16/06/2021 Profile: Codesys V3.5 Sp17Luis SalasNo ratings yet
- Chisel Dac 2012 CorrectedDocument10 pagesChisel Dac 2012 Correctedgoxomi7969No ratings yet
- Lumwana Mining CompanyDocument6 pagesLumwana Mining CompanyMabvuto Banda the son of the Consuming fireNo ratings yet
- Volatile Matter (Including Water) of Vinyl Chloride Resins: Standard Test Method ForDocument3 pagesVolatile Matter (Including Water) of Vinyl Chloride Resins: Standard Test Method ForNabeel H. Al-SaighNo ratings yet
- IQM - Lecture GuideDocument12 pagesIQM - Lecture GuideKiran KumarNo ratings yet
- Loop Powered Microprocessor Controlled Positioner: Worcester Control ValvesDocument4 pagesLoop Powered Microprocessor Controlled Positioner: Worcester Control Valveskarim karimNo ratings yet
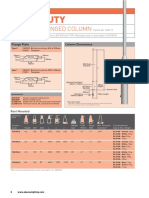
- Light Duty: 4-8M Base Hinged ColumnDocument3 pagesLight Duty: 4-8M Base Hinged ColumnAbrar AhmadNo ratings yet
- SP6 - 1 - Steel Section Details PDFDocument209 pagesSP6 - 1 - Steel Section Details PDFAnkur JainNo ratings yet
- Galvanic Corrosion of Zinc Anode and Copper Cathode Cell PDFDocument6 pagesGalvanic Corrosion of Zinc Anode and Copper Cathode Cell PDFsoekarnoNo ratings yet
- Mathematics For Economics (ECON 104)Document46 pagesMathematics For Economics (ECON 104)Experimental BeXNo ratings yet
- Astm A532 PDFDocument4 pagesAstm A532 PDFJuan Leon100% (1)
- 06 Introduction To Investment ABM BF12 IVm N 25Document32 pages06 Introduction To Investment ABM BF12 IVm N 25jcxes Del rosario100% (2)
- Dell-Opnmang-Plug-In-V2.0-For-Oracle-Entrps-Mangr-12c - Release Notes - En-UsDocument5 pagesDell-Opnmang-Plug-In-V2.0-For-Oracle-Entrps-Mangr-12c - Release Notes - En-UsBelu IonNo ratings yet




![[British Dental Journal 2014-may 23 vol. 216 iss. 10] Ngo, H._ Opsahl-Vital, S. - Minimal intervention dentistry II_ part 7. Minimal intervention in cariology_ the role of glass-ionomer cements in the preservat (201](https://imgv2-2-f.scribdassets.com/img/document/649305346/149x198/7311994bf1/1710571811?v=1)