You might also like
- 2020 Bidirectional Association Between Tuberculosis and SarcoidosisDocument8 pages2020 Bidirectional Association Between Tuberculosis and SarcoidosisLCCNo ratings yet
- Epidemiological Risk Factors For Adult Dengue in Singapore: An 8-Year Nested Test Negative Case Control StudyDocument9 pagesEpidemiological Risk Factors For Adult Dengue in Singapore: An 8-Year Nested Test Negative Case Control StudydouwesdNo ratings yet
- CAP - PrinaDocument12 pagesCAP - PrinaSalNo ratings yet
- NeumoniaDocument28 pagesNeumoniaresidentes isssteNo ratings yet
- Childhood Pneumonia Etiology and Treatment ReviewDocument32 pagesChildhood Pneumonia Etiology and Treatment ReviewlaurentiaNo ratings yet
- Pneumonia Severity Index in Viral Community Acquired Pneumonia in AdultsDocument12 pagesPneumonia Severity Index in Viral Community Acquired Pneumonia in Adultsmuhammad_ariefNo ratings yet
- 2021 - TorresDocument28 pages2021 - TorresCarlosNo ratings yet
- Epidemiology Characteristics of Streptococcus Pneumoniae From Children With Pneumonia in Shanghai: A Retrospective StudyDocument10 pagesEpidemiology Characteristics of Streptococcus Pneumoniae From Children With Pneumonia in Shanghai: A Retrospective StudyAna-Mihaela BalanuțaNo ratings yet
- Mortality Among Tuberculosis Patients in The Democratic Republic of CongoDocument7 pagesMortality Among Tuberculosis Patients in The Democratic Republic of CongoGary Rios DionicioNo ratings yet
- HCW Vs Adult Influenza IncidenceDocument9 pagesHCW Vs Adult Influenza Incidencereza_adrian_2No ratings yet
- Obesity Increases The Duration of Influenza A Virus Shedding in AdultsDocument5 pagesObesity Increases The Duration of Influenza A Virus Shedding in AdultsJuanze 41No ratings yet
- Epidemiology of Tuberculosis and HIV Coinfections in Singapore, 2000 2014Document6 pagesEpidemiology of Tuberculosis and HIV Coinfections in Singapore, 2000 2014jessicaNo ratings yet
- Childhood CAPDocument8 pagesChildhood CAPAlex Toman Fernando SaragihNo ratings yet
- Improving Survival With TBDocument8 pagesImproving Survival With TBdani catriaNo ratings yet
- Usia TBDocument9 pagesUsia TBViviNo ratings yet
- New MOC ResourcesDocument22 pagesNew MOC ResourcesYidnekachew Girma AssefaNo ratings yet
- IOSR JournalsDocument10 pagesIOSR JournalsInternational Organization of Scientific Research (IOSR)No ratings yet
- Serious Fungal Infections in The Philippines: Original ArticleDocument5 pagesSerious Fungal Infections in The Philippines: Original ArticleAilen LagulaNo ratings yet
- Effects of Vaccination and The New Neuraminidase Inhibitor, Laninamivir, On Influenza InfectionDocument6 pagesEffects of Vaccination and The New Neuraminidase Inhibitor, Laninamivir, On Influenza InfectionenggaingetNo ratings yet
- Apid 8 2 98735Document5 pagesApid 8 2 98735ko naythweNo ratings yet
- Fungalinfections in The Icu: Marya D. Zilberberg,, Andrew F. ShorrDocument18 pagesFungalinfections in The Icu: Marya D. Zilberberg,, Andrew F. ShorrGiselle BaiãoNo ratings yet
- A Comparative-Descriptive Analysis of Clinical Characteristics in 2019-Coronavirus-Infected Children and AdultsDocument28 pagesA Comparative-Descriptive Analysis of Clinical Characteristics in 2019-Coronavirus-Infected Children and AdultsPatrick NunsioNo ratings yet
- CAP Guidelines SA 2020Document22 pagesCAP Guidelines SA 2020kudzaimuregidubeNo ratings yet
- 90532100Document5 pages90532100Devi PuspasariNo ratings yet
- Articulo MicroDocument8 pagesArticulo Microliliana ospinaNo ratings yet
- Pertussis Detection in Children With Cough of Any Duration: Researcharticle Open AccessDocument9 pagesPertussis Detection in Children With Cough of Any Duration: Researcharticle Open AccessLee제노No ratings yet
- Typhoid Fever in Children Aged Less Than 5 Years: The Lancet August 1999Document5 pagesTyphoid Fever in Children Aged Less Than 5 Years: The Lancet August 1999Marian SplashNo ratings yet
- Meningitis Bacteriana Aguda en El AdultoDocument12 pagesMeningitis Bacteriana Aguda en El AdultoJulian AlbarracínNo ratings yet
- Jurnal TBC Inter 1Document5 pagesJurnal TBC Inter 1sekti lindaNo ratings yet
- Journal of Infectious Diseases and Epidemiology Jide 6 166Document6 pagesJournal of Infectious Diseases and Epidemiology Jide 6 166Stephanie AndersonNo ratings yet
- DiagnosisofpulmonaryTB in ChildrenDocument8 pagesDiagnosisofpulmonaryTB in ChildrenSumit MitraNo ratings yet
- Prevalence and Determinants of Human Immunodeficiency Virus and Tuberculosis Co-Infection at Kampala International University Teaching HospitalDocument6 pagesPrevalence and Determinants of Human Immunodeficiency Virus and Tuberculosis Co-Infection at Kampala International University Teaching HospitalKIU PUBLICATION AND EXTENSIONNo ratings yet
- 19 Ninan EtalDocument6 pages19 Ninan EtaleditorijmrhsNo ratings yet
- 1 s2.0 S0929664621003892 MainDocument8 pages1 s2.0 S0929664621003892 Mainrheynamaulidar rumoninNo ratings yet
- Irv 12867Document10 pagesIrv 12867Ihsan fahrojiNo ratings yet
- CBD 1 - Iqbal MuhammadDocument8 pagesCBD 1 - Iqbal MuhammadAnonymous D8BO57g3No ratings yet
- The Epidemiological Landscape of The National Influenza Sentinel Surveillance System From 2016 To 2019, TanzaniaDocument10 pagesThe Epidemiological Landscape of The National Influenza Sentinel Surveillance System From 2016 To 2019, TanzaniaInternational Journal of Innovative Science and Research Technology100% (1)
- Towards Personalized Medicine in Bronchiolitis: Word Count: 972Document7 pagesTowards Personalized Medicine in Bronchiolitis: Word Count: 972Pediatría grupoNo ratings yet
- Community-Acquired Pneumonia in Children: Myths and FactsDocument4 pagesCommunity-Acquired Pneumonia in Children: Myths and FactsFranciscoDelgadoNo ratings yet
- Du 2019Document11 pagesDu 2019Briliant GhaustinNo ratings yet
- Jurnal 1Document8 pagesJurnal 1aziskarnNo ratings yet
- Mendeley 03Document5 pagesMendeley 03faraNo ratings yet
- 1 s2.0 S2213007117303866 Main PDFDocument5 pages1 s2.0 S2213007117303866 Main PDFSasqia Rakhmi LeonyNo ratings yet
- Immunogenicity of Fractional-Dose Vaccine During A Yellow Fever Outbreak - Preliminary ReportDocument9 pagesImmunogenicity of Fractional-Dose Vaccine During A Yellow Fever Outbreak - Preliminary Reportrizki agusmaiNo ratings yet
- Ofx 137Document7 pagesOfx 137Sheila Alcalde RNo ratings yet
- IJTLDeditorial Protecting HCworkers Form TBDocument2 pagesIJTLDeditorial Protecting HCworkers Form TBRoma ParyaniNo ratings yet
- Jurnal Internasional Priscilla 2020Document13 pagesJurnal Internasional Priscilla 2020Nita S. NingsihNo ratings yet
- Literature Review On Typhoid FeverDocument4 pagesLiterature Review On Typhoid Feverc5h4drzjNo ratings yet
- Jurnal Seasonal Influenza Vaccination Among Older Adults in Jordan Prevalence Knowledge and AttitudesDocument6 pagesJurnal Seasonal Influenza Vaccination Among Older Adults in Jordan Prevalence Knowledge and AttitudesMusdaliva Tri Riskiani AlminNo ratings yet
- Respiratory Tract Virus Infections in The Elderly With PneumoniaDocument11 pagesRespiratory Tract Virus Infections in The Elderly With PneumoniatanyasisNo ratings yet
- Introduction to Community Acquired Pneumonia in ChildrenDocument7 pagesIntroduction to Community Acquired Pneumonia in ChildrenindahNo ratings yet
- Research ArticleDocument17 pagesResearch ArticleNatanael KindangenNo ratings yet
- Transmission of Nipah Virus - 14 Years of Investigations in BangladeshDocument11 pagesTransmission of Nipah Virus - 14 Years of Investigations in BangladeshRica Pauline LeogoNo ratings yet
- Tuberculosis Treatment Delay and Nosocomial Exposure Remain Important Risks For Patients Undergoing Regular HemodialysisDocument9 pagesTuberculosis Treatment Delay and Nosocomial Exposure Remain Important Risks For Patients Undergoing Regular HemodialysisRayCassidyNo ratings yet
- Copd 14 2219Document9 pagesCopd 14 2219Ruby FirdausNo ratings yet
- New England Journal Medicine: The ofDocument11 pagesNew England Journal Medicine: The ofFransisca PekertiNo ratings yet
- Abstract PneumoniaDocument2 pagesAbstract PneumoniaAlissa MaghopoyNo ratings yet
- Diagnosis & Treatment of Tuberculosis in HIV Co-Infected PatientsDocument16 pagesDiagnosis & Treatment of Tuberculosis in HIV Co-Infected PatientsdevisilalahiNo ratings yet
- Living on the Frontline of COVID-19 in MCO And CMCOFrom EverandLiving on the Frontline of COVID-19 in MCO And CMCONo ratings yet
- Living on the Frontline of COVID-19 in MCO And CMCO: Clinical Updates in COVID-19From EverandLiving on the Frontline of COVID-19 in MCO And CMCO: Clinical Updates in COVID-19No ratings yet
- Desain KwantitatifDocument14 pagesDesain KwantitatifGrimmboyYTNo ratings yet
- ANALISA JURNAL Sindrom Koroner Akut (SKA)Document22 pagesANALISA JURNAL Sindrom Koroner Akut (SKA)GrimmboyYTNo ratings yet
- Perencanaan Asuhan Keperawatan Pasien Hipertensi 2Document7 pagesPerencanaan Asuhan Keperawatan Pasien Hipertensi 2GrimmboyYTNo ratings yet
- Laporan Pendahuluan - Asfiksia - NeonatorumDocument14 pagesLaporan Pendahuluan - Asfiksia - NeonatorumGrimmboyYTNo ratings yet
- Perencanaan Asuhan Keperawatan Pasien HipertensiDocument17 pagesPerencanaan Asuhan Keperawatan Pasien HipertensiGrimmboyYTNo ratings yet
- JURNAL PERNAFASAN Smoking, Alcohol, and Nutritional Status in Relation To One-Year Mortality inDocument5 pagesJURNAL PERNAFASAN Smoking, Alcohol, and Nutritional Status in Relation To One-Year Mortality inGrimmboyYTNo ratings yet
- Asuhan Keperawatan Pada Bayi S Dengan Asfeksia BeratDocument5 pagesAsuhan Keperawatan Pada Bayi S Dengan Asfeksia BeratGrimmboyYTNo ratings yet
- Huang V Tesla State of Calif 20190430Document20 pagesHuang V Tesla State of Calif 20190430jonathan_skillings100% (1)
- Introduction To Financial Planning Unit 1Document57 pagesIntroduction To Financial Planning Unit 1Joshua GeddamNo ratings yet
- bk978 1 6817 4068 3ch1Document28 pagesbk978 1 6817 4068 3ch1fysmaNo ratings yet
- Science MELCsDocument42 pagesScience MELCsRanjell Allain TorresNo ratings yet
- The Mysteries of Plato: Lunar NotebookDocument2 pagesThe Mysteries of Plato: Lunar NotebookDavor BatesNo ratings yet
- Cubic Spline Tutorial v3Document6 pagesCubic Spline Tutorial v3Praveen SrivastavaNo ratings yet
- Search Engine Marketing Course Material 2t4d9Document165 pagesSearch Engine Marketing Course Material 2t4d9Yoga Guru100% (2)
- Power System Analysis and Design, SI EditionDocument5 pagesPower System Analysis and Design, SI EditionAkimeNo ratings yet
- 01 A Brief Introduction To Cloud ComputingDocument25 pages01 A Brief Introduction To Cloud ComputingfirasibraheemNo ratings yet
- Teaching Vocabulary Through TPR Method ToDocument41 pagesTeaching Vocabulary Through TPR Method ToAan Safwandi100% (3)
- 3343 - C-Data-EPON-OLT-FD1108S-CLI-User-Manual-V1-3Document82 pages3343 - C-Data-EPON-OLT-FD1108S-CLI-User-Manual-V1-3Roar ZoneNo ratings yet
- RIBA Outline Plan of Work ExplainedDocument20 pagesRIBA Outline Plan of Work ExplainedkenNo ratings yet
- Password ManagementDocument7 pagesPassword ManagementNeerav KrishnaNo ratings yet
- FMAI - Ch04 - Stock MarketDocument105 pagesFMAI - Ch04 - Stock Marketngoc duongNo ratings yet
- The Joint Force Commander's Guide To Cyberspace Operations: by Brett T. WilliamsDocument8 pagesThe Joint Force Commander's Guide To Cyberspace Operations: by Brett T. Williamsأريزا لويسNo ratings yet
- Public OpinionDocument7 pagesPublic OpinionSona Grewal100% (1)
- CBK Test QuestionsDocument2 pagesCBK Test QuestionsMehul GuptaNo ratings yet
- Reprocessing Guide: Shaver Handpiece TrayDocument198 pagesReprocessing Guide: Shaver Handpiece TrayAnne Stephany ZambranoNo ratings yet
- Cheat Codes SkyrimDocument13 pagesCheat Codes SkyrimDerry RahmaNo ratings yet
- LESSON 9 Steam Generators 2Document12 pagesLESSON 9 Steam Generators 2Salt PapiNo ratings yet
- 01 - PV - RESCO 1d Workshop - S1 PDFDocument61 pages01 - PV - RESCO 1d Workshop - S1 PDFDeasy KurniawatiNo ratings yet
- Construction Materials and Testing: "WOOD"Document31 pagesConstruction Materials and Testing: "WOOD"Aira Joy AnyayahanNo ratings yet
- Introduction to Globalization ExplainedDocument27 pagesIntroduction to Globalization ExplainedMichael Ron DimaanoNo ratings yet
- Textbook of Heat Transfer Sukhatme S PDocument122 pagesTextbook of Heat Transfer Sukhatme S PSamer HouzaynNo ratings yet
- Tiresocks CatalogDocument19 pagesTiresocks CatalogAshBossNo ratings yet
- Inner Unit EstimateDocument35 pagesInner Unit EstimateMir MoNo ratings yet
- ArchimedesDocument22 pagesArchimedessharfexNo ratings yet
- DaburDocument3 pagesDaburchiru94No ratings yet
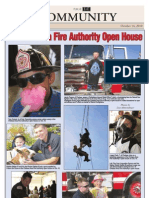
- CAFA Open House HighlightsDocument1 pageCAFA Open House HighlightsDaniel LaiNo ratings yet
- S 1804 2019 (E) - 0Document9 pagesS 1804 2019 (E) - 0Juan Agustin CuadraNo ratings yet