You might also like
- Coughing, A Simple Guide to The Condition, Treatment and Related ConditionsFrom EverandCoughing, A Simple Guide to The Condition, Treatment and Related ConditionsNo ratings yet
- What Is Tuberculosis?: Tuberculosis. It Usually Affects The Lung, But ItDocument1 pageWhat Is Tuberculosis?: Tuberculosis. It Usually Affects The Lung, But ItMaria Lourdes Cutipa MoranNo ratings yet
- Group Case Study - Pulmonary TBDocument8 pagesGroup Case Study - Pulmonary TBCj NiñalNo ratings yet
- What Is TBDocument2 pagesWhat Is TBAlyssa Mae EscalonaNo ratings yet
- TBDocument19 pagesTBJohn Kevin De VeraNo ratings yet
- Teaching Plan For TBDocument5 pagesTeaching Plan For TBChi Tuazon75% (4)
- By Hemant Sharma Tuberculosis: Latent TB. in This Condition, You Have A TB Infection, But The Bacteria RemainDocument8 pagesBy Hemant Sharma Tuberculosis: Latent TB. in This Condition, You Have A TB Infection, But The Bacteria RemainHemant SharmaNo ratings yet
- TUBERCULOSISDocument4 pagesTUBERCULOSISamirNo ratings yet
- TB - OutlineDocument11 pagesTB - Outlinekent yeeNo ratings yet
- What Is TuberculosisDocument6 pagesWhat Is Tuberculosissachin002kypNo ratings yet
- MTB 2 (1) .Docx23.docx23Document9 pagesMTB 2 (1) .Docx23.docx23nurnamekNo ratings yet
- TuberculosisDocument22 pagesTuberculosisIrumvamwizerwa OnesmeNo ratings yet
- TuberculosisDocument8 pagesTuberculosisArathi KarshNo ratings yet
- TuberculosisDocument15 pagesTuberculosisNovy Sylvia WardanaNo ratings yet
- Tetanus NoteDocument4 pagesTetanus NoteTaufik KhanNo ratings yet
- TUBERCULOSISDocument19 pagesTUBERCULOSISSaranya DeviNo ratings yet
- TUBERCULOSISDocument6 pagesTUBERCULOSISByzid ByzidNo ratings yet
- Cours tuberculosediabetEBOAHIVDocument18 pagesCours tuberculosediabetEBOAHIVhamedpourlesmeufsNo ratings yet
- Assignment No 1 DDocument4 pagesAssignment No 1 Ddanishbiggest124No ratings yet
- 2 MDW 204 Target Disease Vaccines & Cold ChainDocument34 pages2 MDW 204 Target Disease Vaccines & Cold ChainMaria Lejani TerencioNo ratings yet
- Health EducationDocument10 pagesHealth Educationrjay pascualNo ratings yet
- Tuberculosis by AkuDocument40 pagesTuberculosis by Akudevita oktaviani salsabilla kiranaNo ratings yet
- Mantoux test-TSTDocument13 pagesMantoux test-TSTNektarios TsakalosNo ratings yet
- Medicated Hand KerchiefsDocument31 pagesMedicated Hand Kerchiefsscribd_lostandfoundNo ratings yet
- Tory O: NameDocument17 pagesTory O: Namejana champakNo ratings yet
- Dengue FeverDocument4 pagesDengue FeverDez TabiosNo ratings yet
- FRSTDocument12 pagesFRSTGuezil Joy DelfinNo ratings yet
- TUBERCULOSISDocument9 pagesTUBERCULOSISRahma WatiNo ratings yet
- Penyuluhan Pelatihan Kader TBDocument16 pagesPenyuluhan Pelatihan Kader TBPutri SijunjungNo ratings yet
- Tuberculosis: Medical DictionaryDocument5 pagesTuberculosis: Medical DictionarydennisgdagoocNo ratings yet
- Tuberculosis (T.B) : What Is TB?Document16 pagesTuberculosis (T.B) : What Is TB?Usman MirzaNo ratings yet
- Hard BoundDocument369 pagesHard BoundClang SantiagoNo ratings yet
- Prevention & Treatment TBDocument14 pagesPrevention & Treatment TBFathiah66No ratings yet
- Diseases and VaccinesDocument37 pagesDiseases and Vaccinesraghu ramNo ratings yet
- Disseminated Tuberculosis: Lymph System Tuberculosis - PulmonaryDocument5 pagesDisseminated Tuberculosis: Lymph System Tuberculosis - PulmonaryJeanette C. LimNo ratings yet
- TuberculosisDocument4 pagesTuberculosisMjel Kezhia BarrietaNo ratings yet
- What Are The Symptoms of TB?Document5 pagesWhat Are The Symptoms of TB?Reden Calubayan OblenaNo ratings yet
- MedSurg 063510Document10 pagesMedSurg 063510Saviana TiekuNo ratings yet
- Tugas Bahasa InggrisDocument2 pagesTugas Bahasa InggrisAnggita NovantiNo ratings yet
- Infectious DiseaseDocument33 pagesInfectious DiseaseVeer RamloghunNo ratings yet
- Tetanus.89898989 (Autosaved)Document15 pagesTetanus.89898989 (Autosaved)Abdulla AbasNo ratings yet
- Urinary Tract InfectionDocument20 pagesUrinary Tract InfectionFaraz SiddiquiNo ratings yet
- Microbial Disease of Respiratory SystemDocument2 pagesMicrobial Disease of Respiratory SystemJanah AbucayNo ratings yet
- 19: 05 24 Sept 2011 Tetanus: SymtompsDocument5 pages19: 05 24 Sept 2011 Tetanus: SymtompsVania ParamithaNo ratings yet
- FB3 - 13-Sudeep Koirala-TuberculosisDocument29 pagesFB3 - 13-Sudeep Koirala-Tuberculosisvaskar_karkiNo ratings yet
- Lopez, Marian Manuson, Ludy Melu, Anna Victoria Modina, Jayson Montenegro, Matilde Krisha 4dpharmacyDocument19 pagesLopez, Marian Manuson, Ludy Melu, Anna Victoria Modina, Jayson Montenegro, Matilde Krisha 4dpharmacyRyan100% (1)
- Tuberculosis (The Disease)Document24 pagesTuberculosis (The Disease)DiLahNo ratings yet
- Human Diseases Including Communicable and Non - Communicable Diseases - Prevention and Remedies - 1st - ChapterDocument22 pagesHuman Diseases Including Communicable and Non - Communicable Diseases - Prevention and Remedies - 1st - ChapterVijaya Kumar SNo ratings yet
- TuberculosisDocument4 pagesTuberculosisKate SantosNo ratings yet
- Tuberculosis (TB) : by Maryam and AyeshaDocument9 pagesTuberculosis (TB) : by Maryam and AyeshaAyesha GulzarNo ratings yet
- SAPNA TRIYANINGSIH - NUTRITION AND DIET HEALTH EDUCATION PLAN TUBERCULOSIS - Id.enDocument3 pagesSAPNA TRIYANINGSIH - NUTRITION AND DIET HEALTH EDUCATION PLAN TUBERCULOSIS - Id.enSapna TriyanNo ratings yet
- Group IDocument3 pagesGroup IyapyapvinxNo ratings yet
- 7 Reading INTDocument50 pages7 Reading INTfiorella lombardiNo ratings yet
- Tuberculosis TBDocument5 pagesTuberculosis TBHusna AmaliaNo ratings yet
- 1.8 Million: What Is Tuberculosis?Document9 pages1.8 Million: What Is Tuberculosis?rahayusri yayuNo ratings yet
- 13 QN ANSWRS Why Do We Fall IllDocument3 pages13 QN ANSWRS Why Do We Fall IllceoNo ratings yet
- BAHASA - INGGRIS ArtikelDocument4 pagesBAHASA - INGGRIS Artikelindah abdullahNo ratings yet
- Gram + DiseasesDocument30 pagesGram + DiseasesveerdedajiNo ratings yet
- Health and DiseaseDocument3 pagesHealth and DiseaseMehbub LaskarNo ratings yet
- TOPIC 8 - DOH Programs Related To Family HealthDocument35 pagesTOPIC 8 - DOH Programs Related To Family HealthRichmon SantosNo ratings yet
- Safety Bulletin 35 HOT WORKDocument3 pagesSafety Bulletin 35 HOT WORKTrebor SantosNo ratings yet
- Safe Working With Flammable SubstancesDocument5 pagesSafe Working With Flammable SubstancesTrebor SantosNo ratings yet
- 11 Things That Make Up A Perfect Fire Evacuation DrillDocument2 pages11 Things That Make Up A Perfect Fire Evacuation DrillTrebor SantosNo ratings yet
- SB 033 Welding and CuttungDocument2 pagesSB 033 Welding and CuttungAl DubNo ratings yet
- Safety Bulletin 7 PORTABLE ELECTRICAL EQUIPMENT SAFETYDocument1 pageSafety Bulletin 7 PORTABLE ELECTRICAL EQUIPMENT SAFETYTrebor SantosNo ratings yet
- Christmas Decor Safety CertificateDocument2 pagesChristmas Decor Safety CertificateTrebor SantosNo ratings yet
- EHS-G-22 Guidelines On Confined Spaces - Procedure v.3Document13 pagesEHS-G-22 Guidelines On Confined Spaces - Procedure v.3Trebor SantosNo ratings yet
- Material Handling & Back Safety 26.09.2014Document28 pagesMaterial Handling & Back Safety 26.09.2014Trebor SantosNo ratings yet
- FMD-F-11-02.8.2.1 - List of Qualifications For Technical Maintenance PersonnelDocument2 pagesFMD-F-11-02.8.2.1 - List of Qualifications For Technical Maintenance PersonnelTrebor SantosNo ratings yet
- Hyundai Elevator Preventive Maintenance ProcedureDocument19 pagesHyundai Elevator Preventive Maintenance ProcedureTrebor Santos100% (2)
- Basic Theories of Electrical EstimatingDocument5 pagesBasic Theories of Electrical EstimatingMike AndayaNo ratings yet
- Scaffold Safety 2014Document88 pagesScaffold Safety 2014Trebor Santos100% (1)
- Hepatitis B BrochureDocument16 pagesHepatitis B BrochureTrebor SantosNo ratings yet
- FMD-F-11-02 12 2 3 - Generator - DailyDocument2 pagesFMD-F-11-02 12 2 3 - Generator - DailyTrebor SantosNo ratings yet
- FMD-F-11-02.12.2.2 Generator No LoadDocument1 pageFMD-F-11-02.12.2.2 Generator No LoadTrebor SantosNo ratings yet
- Compliance Process FlowDocument1 pageCompliance Process FlowTrebor SantosNo ratings yet
- Using Ultrasound For High Voltage Insulation Testing - Maintenance TechnologyDocument7 pagesUsing Ultrasound For High Voltage Insulation Testing - Maintenance TechnologyTrebor SantosNo ratings yet
- How To Protect Your Organization From Electrical Power OutagesDocument4 pagesHow To Protect Your Organization From Electrical Power OutagesTrebor SantosNo ratings yet
- Testing Switchgear Fro Partial Discharge ActivityDocument2 pagesTesting Switchgear Fro Partial Discharge ActivityTrebor SantosNo ratings yet
- Nonintrusive Partial Discharge Measurements On High Voltage SwitchgearDocument3 pagesNonintrusive Partial Discharge Measurements On High Voltage SwitchgearTrebor SantosNo ratings yet
- Early Signs of Equipment FailureDocument5 pagesEarly Signs of Equipment FailureTrebor SantosNo ratings yet
- Substation Online Partial Discharge Testing (OLPD) Testing Tech. Update and InfoDocument11 pagesSubstation Online Partial Discharge Testing (OLPD) Testing Tech. Update and InfoTrebor SantosNo ratings yet
- Dengue Fever in The Philippines1Document23 pagesDengue Fever in The Philippines1Nikko MelencionNo ratings yet
- WHO Dengue Guidelines 2013Document160 pagesWHO Dengue Guidelines 2013Jason MirasolNo ratings yet
- DiabetesDocument28 pagesDiabetesJohn Paulo Morales100% (1)
- La ThaliliaDocument1 pageLa ThaliliaTrebor SantosNo ratings yet
- Dengue FeverDocument44 pagesDengue FeverTrebor Santos100% (2)
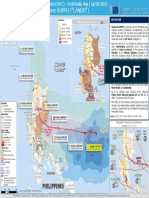
- PHILIPPINES - Tropical Cyclone KOPPU ("LANDO") : LuzonDocument1 pagePHILIPPINES - Tropical Cyclone KOPPU ("LANDO") : LuzonTrebor SantosNo ratings yet