You might also like
- (E.g. Plastic Surgery) (Important)Document4 pages(E.g. Plastic Surgery) (Important)Felix FwsNo ratings yet
- (Facility Name) SURVIVORSHIP CARE PLAN (Surgical, Medical, and Radiation Oncology) Section I - Treatment SummaryDocument4 pages(Facility Name) SURVIVORSHIP CARE PLAN (Surgical, Medical, and Radiation Oncology) Section I - Treatment SummaryMelanie Ingrid Laurente CciraNo ratings yet
- A Comprehensive Guide To Emergency and Trauma CareDocument3 pagesA Comprehensive Guide To Emergency and Trauma CareihealthmailboxNo ratings yet
- Navigating Public Health Emergencies - A Guide To Preparedness and ResilienceDocument3 pagesNavigating Public Health Emergencies - A Guide To Preparedness and ResilienceihealthmailboxNo ratings yet
- CHNN312 Prelim LectureDocument7 pagesCHNN312 Prelim Lecturereminder to be happyNo ratings yet
- Emergency Care Training Manual For CHO at AB-HWCDocument82 pagesEmergency Care Training Manual For CHO at AB-HWCmohammed raziNo ratings yet
- Unit 1.2 History, Determinants, Core Functions, Essentials, Uhc, and Health Delivery Systems Disease Control PhaseDocument1 pageUnit 1.2 History, Determinants, Core Functions, Essentials, Uhc, and Health Delivery Systems Disease Control PhaseREGINE COELI LANSANGANNo ratings yet
- CHN SeminarDocument6 pagesCHN SeminarReyza Marxel KennedyNo ratings yet
- PHC 1Document21 pagesPHC 1judahNo ratings yet
- Provider Burnout and Fatigue During The COVID-19 Pandemic Leasson Learned From A High Volume Intensive Care UnitDocument6 pagesProvider Burnout and Fatigue During The COVID-19 Pandemic Leasson Learned From A High Volume Intensive Care UnitSyifaa IrawanNo ratings yet
- Anesthesiologists' Role in Disaster ManagementDocument43 pagesAnesthesiologists' Role in Disaster ManagementHuzayval AchmadNo ratings yet
- Disaster Nursing: Presented By: Ms. Monika KanwarDocument23 pagesDisaster Nursing: Presented By: Ms. Monika KanwarMonika100% (1)
- Disaster Management CycleDocument10 pagesDisaster Management CycleRohit Singh nNo ratings yet
- How To Restart National Economies During The Coronavirus CrisisDocument16 pagesHow To Restart National Economies During The Coronavirus CrisisRodolfo RivadeneyraNo ratings yet
- Disaster Behavioral Health Response PlanDocument26 pagesDisaster Behavioral Health Response Planapi-438654076No ratings yet
- Toprank CHN NotesDocument4 pagesToprank CHN Notesdwlnuestro10No ratings yet
- Disaster ManagementDocument11 pagesDisaster ManagementLoma Waghmare (Jadhav)No ratings yet
- Out 9Document17 pagesOut 9hikmat pramajatiNo ratings yet
- CHN Review HandoutDocument18 pagesCHN Review HandoutJaropojop, JemykaNo ratings yet
- ADMINSTRATIVE ORDER No. 2020-0015 Guidelines On The Risk-Based Public Health Standards For COVID-19 Mitigation ScopeDocument13 pagesADMINSTRATIVE ORDER No. 2020-0015 Guidelines On The Risk-Based Public Health Standards For COVID-19 Mitigation ScopeMikee PortesNo ratings yet
- A1 Introduction To Health PromotionDocument17 pagesA1 Introduction To Health PromotionAfia SarpongNo ratings yet
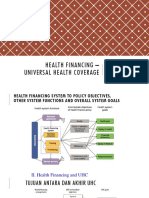
- Pembiayaan Kesehatan UHCDocument43 pagesPembiayaan Kesehatan UHCGenre PesselNo ratings yet
- Ao 2020-0016 Minimum Health System Capacity Standards For Covid-19 Preparedness and Response Strategies - 1588669431 - 1588983280 PDFDocument46 pagesAo 2020-0016 Minimum Health System Capacity Standards For Covid-19 Preparedness and Response Strategies - 1588669431 - 1588983280 PDFVeda MariaNo ratings yet
- Who Covid-19 Mass Gathering Risk Assessment TrainingDocument13 pagesWho Covid-19 Mass Gathering Risk Assessment TrainingfarikoNo ratings yet
- Disaster Rehabilitation Response Plan: Now or NeverDocument8 pagesDisaster Rehabilitation Response Plan: Now or NeverAgus SGNo ratings yet
- Community Health Nursing PDFDocument25 pagesCommunity Health Nursing PDFCharles J B. Visaya80% (5)
- Community Health Nursing PDFDocument25 pagesCommunity Health Nursing PDFCharles J B. Visaya100% (1)
- Community Health Nursing PDFDocument25 pagesCommunity Health Nursing PDFCharles J B. VisayaNo ratings yet
- The Evolution of Public Health Emergency Ajph.2017.303947Document8 pagesThe Evolution of Public Health Emergency Ajph.2017.303947Jack Yu-Tung ChangNo ratings yet
- CA NursingDocument5 pagesCA NursingMary Angel Nicka LuayonNo ratings yet
- Community Health Nursing - RefresherDocument13 pagesCommunity Health Nursing - Refresherkaty loNo ratings yet
- (แปล) Check-list Assess Vunerability-engDocument55 pages(แปล) Check-list Assess Vunerability-engMizuno MichiruNo ratings yet
- Trauma Care ChecklistDocument2 pagesTrauma Care ChecklistSYIFANo ratings yet
- 19th PHEMAP - Development of Preparedness Plan - MDADocument77 pages19th PHEMAP - Development of Preparedness Plan - MDAAngkol TuyorNo ratings yet
- Has Epidemiology Become Infatuated With Methods ? A Historical Perspective On The Place of Methods During The Classical (1945-1965) Phase of EpidemiologyDocument25 pagesHas Epidemiology Become Infatuated With Methods ? A Historical Perspective On The Place of Methods During The Classical (1945-1965) Phase of EpidemiologyAndre LanzerNo ratings yet
- 01 Defenition and Disaster CycleDocument18 pages01 Defenition and Disaster CycleIrendawati DoeNo ratings yet
- UNDRR - Public Health Scorecard Addendum v2.0 - English-Jan2021Document20 pagesUNDRR - Public Health Scorecard Addendum v2.0 - English-Jan2021Shereen RodrigoNo ratings yet
- Risk Assessment Guidance: Field Title Required InformationDocument14 pagesRisk Assessment Guidance: Field Title Required InformationMohd AimanNo ratings yet
- Early Rehabilitation: in Conflicts and DisastersDocument220 pagesEarly Rehabilitation: in Conflicts and DisastersRita MoreiraNo ratings yet
- WHO MOOC RCCE Behavior ChangeDocument28 pagesWHO MOOC RCCE Behavior Changetiana raditaNo ratings yet
- Disaster Nursing PrefinalsDocument6 pagesDisaster Nursing PrefinalsZarida ArabainNo ratings yet
- Who Mooc Rcce Behavior ChangeDocument28 pagesWho Mooc Rcce Behavior Changetiana raditaNo ratings yet
- RCCE COVID-19 Module 1 Part ADocument13 pagesRCCE COVID-19 Module 1 Part Atiana raditaNo ratings yet
- Notes CommedDocument3 pagesNotes CommedRomeo GianNo ratings yet
- Management of Disasters: Shrawan Kumar Mandal MBBS 2014 Resource Faculty: Dr. Bijaya AryalDocument24 pagesManagement of Disasters: Shrawan Kumar Mandal MBBS 2014 Resource Faculty: Dr. Bijaya AryalSantosh ThapaNo ratings yet
- Project Basics of Health Care Management: Subject Code: Bne1D Semester - 1Document9 pagesProject Basics of Health Care Management: Subject Code: Bne1D Semester - 1The Pursuit of HappinessNo ratings yet
- 2022 DRRM-H PlanDocument24 pages2022 DRRM-H PlanRHU ALCALANo ratings yet
- DisasterDocument6 pagesDisasterSakthi DeviNo ratings yet
- 4.nursing Management in DisasterDocument15 pages4.nursing Management in Disastersari arie lestariNo ratings yet
- The Intersection of Technology and HealthDocument3 pagesThe Intersection of Technology and HealthihealthmailboxNo ratings yet
- Chinese Nursing Research: Research Progress in Disaster Nursing Competency Framework of Nurses in ChinaDocument4 pagesChinese Nursing Research: Research Progress in Disaster Nursing Competency Framework of Nurses in ChinaSyahrizal FahmiantoNo ratings yet
- CHNDocument19 pagesCHNShai EstrellerNo ratings yet
- Chapter 3 - DisasterNursing - GilbertFernandoDocument50 pagesChapter 3 - DisasterNursing - GilbertFernandoGilbert FernandoNo ratings yet
- Epidemiology of Tropical DiseasesDocument3 pagesEpidemiology of Tropical DiseasesHendraNo ratings yet
- Rha - Car SurDocument5 pagesRha - Car Suraron carlo calubNo ratings yet
- The Influence of The Economic Crisis On The Association Between Unemployment and Health An Empirical Analysis For SpainDocument11 pagesThe Influence of The Economic Crisis On The Association Between Unemployment and Health An Empirical Analysis For SpainJohn AcevedoNo ratings yet
- CHN NotesDocument5 pagesCHN NotesVinceNo ratings yet
- Transforming Society: A Comprehensive Introduction to Understanding Trauma, Adversity, & Becoming a Trauma-Informed OrganisationFrom EverandTransforming Society: A Comprehensive Introduction to Understanding Trauma, Adversity, & Becoming a Trauma-Informed OrganisationNo ratings yet
- Denatured Fuel Ethanol: Material Safety Data SheetDocument14 pagesDenatured Fuel Ethanol: Material Safety Data SheetElder Andrades MartinezNo ratings yet
- Articles of PartnershipDocument3 pagesArticles of Partnershipjonel sembranaNo ratings yet
- Jas08 4Document3 pagesJas08 4krishna saiNo ratings yet
- Hopes For Speedy Rebound Dim: For Personal, Non-Commercial Use OnlyDocument32 pagesHopes For Speedy Rebound Dim: For Personal, Non-Commercial Use OnlyMiguel DiazNo ratings yet
- Health Insurance COMPANYDocument6 pagesHealth Insurance COMPANYWajid MalikNo ratings yet
- Test Bank For Drugs Society and Human Behavior 17th EditionDocument7 pagesTest Bank For Drugs Society and Human Behavior 17th EditionHarry Seldon100% (29)
- 4.iJGP - Case ReportDocument4 pages4.iJGP - Case Reportpalak GandhiNo ratings yet
- Strauman BLX Product Catalog - 450.012-A-En - LowDocument22 pagesStrauman BLX Product Catalog - 450.012-A-En - LowDiyaa SakrNo ratings yet
- Lumbopelvic Stabilization Exercises and Mckenzie Method in Low Back Pain Due To Disc Protrusion: A Blind Randomized Clinical TrialDocument12 pagesLumbopelvic Stabilization Exercises and Mckenzie Method in Low Back Pain Due To Disc Protrusion: A Blind Randomized Clinical TrialZahra SativaniNo ratings yet
- Waste Management Problem in Raghumanda Village: Department of Civil EngineeringDocument14 pagesWaste Management Problem in Raghumanda Village: Department of Civil EngineeringHémáñth RájNo ratings yet
- The Radiology Specialty Is Constantly ChangingDocument3 pagesThe Radiology Specialty Is Constantly ChangingLiora SochenNo ratings yet
- PsychosocialSupport2023 2024Document5 pagesPsychosocialSupport2023 2024Jasmin LicudineNo ratings yet
- Sample Paper English - 6Document8 pagesSample Paper English - 6Gurukul PatnaNo ratings yet
- Staff Nurses, Lab-Technicians& Pharmacists: WWW - Vizianagaram.nic - inDocument6 pagesStaff Nurses, Lab-Technicians& Pharmacists: WWW - Vizianagaram.nic - inSATYAM NAIDUNo ratings yet
- The Problem and Background of The StudyDocument6 pagesThe Problem and Background of The StudyAileen ElegadoNo ratings yet
- Peronsal Construct TheoryDocument7 pagesPeronsal Construct TheoryToby PearceNo ratings yet
- HDFC ERGO General Insurance Company Limited: Claim Form - Part ADocument7 pagesHDFC ERGO General Insurance Company Limited: Claim Form - Part AchakshuNo ratings yet
- Assignment - 4: The Saying Goes 'He/ She Who Knows Occlusion Knows Dentistry 'Document19 pagesAssignment - 4: The Saying Goes 'He/ She Who Knows Occlusion Knows Dentistry 'nivitha naidu100% (1)
- Nyvad 1999Document9 pagesNyvad 1999Felipe Maldonado ArayaNo ratings yet
- General Survey - Nursing AssessmentDocument2 pagesGeneral Survey - Nursing AssessmentDanielle TorresNo ratings yet
- Differences in Tear Secretion Before and After Phacoemulsification Surgery Using Schirmer I TestsDocument4 pagesDifferences in Tear Secretion Before and After Phacoemulsification Surgery Using Schirmer I TestsKris AdinataNo ratings yet
- PCR My - Wan Nur Afiyah - 8mayDocument1 pagePCR My - Wan Nur Afiyah - 8mayEvie SuriNo ratings yet
- Sysmex XW - 100: Instructions For Use ManualDocument32 pagesSysmex XW - 100: Instructions For Use ManualNahom BalchaNo ratings yet
- Changes of Vitamin D Levels in Parkinson's Disease in LibyaDocument1 pageChanges of Vitamin D Levels in Parkinson's Disease in LibyaJagannadh peelaNo ratings yet
- Pengisian Tanggal3Document32 pagesPengisian Tanggal3gusrina simamoraNo ratings yet
- Maxillary LandmarksDocument30 pagesMaxillary LandmarksRajsandeep Singh86% (14)
- Psychological ScalesDocument6 pagesPsychological ScalesMorris BeneboNo ratings yet
- Personal Development: Quarter 2 - Module 6: Persons and Careers (Career Basic Concepts)Document3 pagesPersonal Development: Quarter 2 - Module 6: Persons and Careers (Career Basic Concepts)Lovely Joy ValdezNo ratings yet
- Neumann 1990Document13 pagesNeumann 1990Hai My NguyenNo ratings yet
- DigitalDiagnost C50 CSV2 High Performance - 0.1 - TXT - TypicalDocument23 pagesDigitalDiagnost C50 CSV2 High Performance - 0.1 - TXT - Typicalemilio paredesNo ratings yet