You might also like
- Cleft Lip and Palate Treatment: A Comprehensive GuideFrom EverandCleft Lip and Palate Treatment: A Comprehensive GuideNivaldo AlonsoNo ratings yet
- Comparison of Efficiency of Electromyography and Nerve Conduction Velocity Studies in Diagnosis of Diabetic NeuropathyDocument5 pagesComparison of Efficiency of Electromyography and Nerve Conduction Velocity Studies in Diagnosis of Diabetic NeuropathyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- MCQ Cleft Lip and PalateDocument14 pagesMCQ Cleft Lip and Palatemarwa100% (1)
- The Permanent Mandibular IncisorsDocument23 pagesThe Permanent Mandibular IncisorsDina YasserNo ratings yet
- Classification Systems For Orofacial Clefts: 10.5005/jp-Journals-10037-1035Document5 pagesClassification Systems For Orofacial Clefts: 10.5005/jp-Journals-10037-1035assususuNo ratings yet
- JKCD 6Document5 pagesJKCD 6sulistyowati_rnNo ratings yet
- Crockett 2014Document14 pagesCrockett 2014JulioRoblesZanelliNo ratings yet
- Shaye CleftLipandPalateDocument17 pagesShaye CleftLipandPalatenurlatifahNo ratings yet
- Cleft Lip and Palate An Evidence Based Review PDFDocument16 pagesCleft Lip and Palate An Evidence Based Review PDFariskaNo ratings yet
- The Spectrum of Orofacial CleftingDocument14 pagesThe Spectrum of Orofacial CleftingJulián David Ríos ZuluagaNo ratings yet
- Seminar On Cleft Lip: Presented by DR - Cathrine Diana PG IIIDocument93 pagesSeminar On Cleft Lip: Presented by DR - Cathrine Diana PG IIIcareNo ratings yet
- Vocal Fold Scars - A Common Classifcation Proposal by The AmericanDocument4 pagesVocal Fold Scars - A Common Classifcation Proposal by The Americananitaabreu123No ratings yet
- Classification of Cleft Lip and Cleft PalateDocument14 pagesClassification of Cleft Lip and Cleft PalateRahul Kumar DiwakarNo ratings yet
- Maxillofacial Defects and Their Classification: A Review.: ArticleDocument7 pagesMaxillofacial Defects and Their Classification: A Review.: ArticleVivek ShankarNo ratings yet
- Evaluation of The Results of Cleft Lip and PalateDocument10 pagesEvaluation of The Results of Cleft Lip and PalateAnang AbdulfattahNo ratings yet
- Craniofacial Deformities Review of Etiologies Distribution and TDocument16 pagesCraniofacial Deformities Review of Etiologies Distribution and TambersNo ratings yet
- Maxillofacial Defects and Their Classification: A Review.: International Journal of Advanced Research June 2016Document7 pagesMaxillofacial Defects and Their Classification: A Review.: International Journal of Advanced Research June 2016botak berjamaahNo ratings yet
- Classification of malocclusions and dental relationshipsDocument7 pagesClassification of malocclusions and dental relationshipsWeiliem AbubakarNo ratings yet
- 2015 Cleft Lip and Palate An Evidence-Based ReviewDocument16 pages2015 Cleft Lip and Palate An Evidence-Based ReviewDimitris RodriguezNo ratings yet
- Dermatoglyphics in Dentistry: A Review: Int J Eth Trauma Victimology 2019 5 (1) :39Document6 pagesDermatoglyphics in Dentistry: A Review: Int J Eth Trauma Victimology 2019 5 (1) :39Rohini TondaNo ratings yet
- Cleft LipDocument37 pagesCleft Lip'Alivia Nabdakh ClocheNo ratings yet
- Management of Midline Facial CleftsDocument8 pagesManagement of Midline Facial CleftsBeatriz ChilenoNo ratings yet
- Cleft Lip and PalateDocument91 pagesCleft Lip and PalatedrgreeshmahariniNo ratings yet
- Final Year Clinicals: Malocclusions and Etiology (Graber)Document35 pagesFinal Year Clinicals: Malocclusions and Etiology (Graber)Sruthy NairNo ratings yet
- History and Examination For RPDDocument19 pagesHistory and Examination For RPDHiba SaadNo ratings yet
- Podj 19Document6 pagesPodj 19salma hasya rahmaniNo ratings yet
- Open Bite, A Review of Etiology and Manageme PDFDocument8 pagesOpen Bite, A Review of Etiology and Manageme PDFVieussens JoffreyNo ratings yet
- Huellas Labiales Unicas Variables y PermanentesDocument5 pagesHuellas Labiales Unicas Variables y PermanentesOscar EmilioNo ratings yet
- Maxillofacial Prosthetics (MFP) : Section FourDocument11 pagesMaxillofacial Prosthetics (MFP) : Section FourRidhoNo ratings yet
- Cl. PLTDocument14 pagesCl. PLTNaveed KhanNo ratings yet
- Cleft PalateDocument22 pagesCleft PalateAmit GaurNo ratings yet
- Clinical Journal. Developing Class IIIDocument18 pagesClinical Journal. Developing Class IIIELIAS DAVID NOBMAN ALVARADONo ratings yet
- Cleft Lip and Cleft PalateDocument54 pagesCleft Lip and Cleft Palatedr parveen bathla100% (3)
- OSMFDocument20 pagesOSMFAl RawdhaNo ratings yet
- Cleft Palate Repair, Gingivoperiosteoplasty and Alveolar Bone GraftingDocument10 pagesCleft Palate Repair, Gingivoperiosteoplasty and Alveolar Bone GraftingAndrés Faúndez TeránNo ratings yet
- Deboutray 2016Document8 pagesDeboutray 2016Fitriani MadiNo ratings yet
- Cleft Lip & PalateDocument52 pagesCleft Lip & PalateShameena KnNo ratings yet
- Prevalence of malocclusion in Chinese youthDocument8 pagesPrevalence of malocclusion in Chinese youthLuis SarmientoNo ratings yet
- Rehabilitation of maxillary defectsDocument67 pagesRehabilitation of maxillary defectspriyaNo ratings yet
- LabiopalatoschisisDocument21 pagesLabiopalatoschisisOna AkyuwenNo ratings yet
- Lipoma of The Oral and Maxillofacial RegionDocument10 pagesLipoma of The Oral and Maxillofacial RegionLaila FortunatoNo ratings yet
- Shear's Cysts of The Oral and Maxillofacial Regions-10-14Document5 pagesShear's Cysts of The Oral and Maxillofacial Regions-10-14muhammad arif100% (1)
- Classification of Cleft Lip or PalateDocument15 pagesClassification of Cleft Lip or PalatecempapiNo ratings yet
- CLEFT LIP AND PALATE SURGICAL REPAIR AND MANAGEMENTDocument76 pagesCLEFT LIP AND PALATE SURGICAL REPAIR AND MANAGEMENTSorinNo ratings yet
- 21LipPrintPatterns With Saggital MalocclusionsVol4issue1pp75-81.20180214071634Document7 pages21LipPrintPatterns With Saggital MalocclusionsVol4issue1pp75-81.20180214071634Abirami MadeshwaranNo ratings yet
- Cleft Lip and Palate: Diagnosis and Management: EviewDocument6 pagesCleft Lip and Palate: Diagnosis and Management: EviewJustin KimberlakeNo ratings yet
- International Caries Detection and Assessment System (ICDAS) PDFDocument4 pagesInternational Caries Detection and Assessment System (ICDAS) PDFEduard ButuzaNo ratings yet
- Classification of MalocclusionDocument69 pagesClassification of MalocclusionBatman 02053No ratings yet
- Classification of Tongue Cancer Resection and Treatment AlgorithmDocument8 pagesClassification of Tongue Cancer Resection and Treatment AlgorithmRahma WatiNo ratings yet
- 41 220 1 PBDocument8 pages41 220 1 PBTejas KhaireNo ratings yet
- Manna 2009Document5 pagesManna 2009ErnestoNo ratings yet
- Cleft LectDocument76 pagesCleft LectDiandra Puspa WidyasariNo ratings yet
- Ankyloglossia Case Report: Tongue-Tie SurgeryDocument4 pagesAnkyloglossia Case Report: Tongue-Tie SurgeryDeasireeNo ratings yet
- Stewart 1982Document38 pagesStewart 1982KharismaNisaNo ratings yet
- IJMRP Lip PrintsDocument10 pagesIJMRP Lip PrintsRohin GargNo ratings yet
- D I D C A I V S: Ermatoglyphics Nterpretation of Ental Aries: N N TudyDocument3 pagesD I D C A I V S: Ermatoglyphics Nterpretation of Ental Aries: N N TudyShahanaaz ShaikNo ratings yet
- Radiology of Cleft Lip and Palate: Imaging For The Prenatal Period and Throughout LifeDocument12 pagesRadiology of Cleft Lip and Palate: Imaging For The Prenatal Period and Throughout LifeAmeria Briliana ShoumiNo ratings yet
- Anatomical Classification of Facial, Cranio-Facial and Latero-Facial CleftsDocument24 pagesAnatomical Classification of Facial, Cranio-Facial and Latero-Facial CleftsAlvaro Jose Uribe TamaraNo ratings yet
- Cl&Palate 22Document72 pagesCl&Palate 22Dr.Naqeeb KakarNo ratings yet
- Cleft Lip, Cleft Palate, and Velopharyngeal.36Document19 pagesCleft Lip, Cleft Palate, and Velopharyngeal.36Jimmy Mejía Cirujano PlásticoNo ratings yet
- Cleft Lip and PalateDocument115 pagesCleft Lip and PalateDavid OdhiamboNo ratings yet
- chapter38Document25 pageschapter38Mai ThúyNo ratings yet
- Influence of Parent-Child Communication on Premarital SexDocument1 pageInfluence of Parent-Child Communication on Premarital SexnskhldNo ratings yet
- Word Dari PDFDocument7 pagesWord Dari PDFnskhldNo ratings yet
- UnknownDocument3 pagesUnknownnskhldNo ratings yet
- S0020729210003772Document1 pageS0020729210003772nskhldNo ratings yet
- List Harga Per Agustus 2022Document21 pagesList Harga Per Agustus 2022nskhldNo ratings yet
- The Number of Female Patients Accessing Our Outpatient Service Was Three Times Higher Than The Number of Male PatientsDocument1 pageThe Number of Female Patients Accessing Our Outpatient Service Was Three Times Higher Than The Number of Male PatientsnskhldNo ratings yet
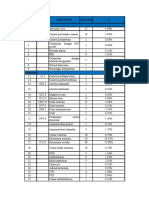
- Top ICD Diagnoses and Patient CountDocument12 pagesTop ICD Diagnoses and Patient CountnskhldNo ratings yet
- Management of Fluid in Critically Ill Obstetric PatientsDocument1 pageManagement of Fluid in Critically Ill Obstetric PatientsnskhldNo ratings yet
- Hydrocephalus DLLDocument18 pagesHydrocephalus DLLnskhldNo ratings yet
- Dataset Age-Sex (Cases)Document76 pagesDataset Age-Sex (Cases)nskhldNo ratings yet
- Epidemiologic and Genetic Associations of Endometriosis With DepressionDocument13 pagesEpidemiologic and Genetic Associations of Endometriosis With DepressionnskhldNo ratings yet
- Determinants of Induced Abortion Among Women of Reproductive AgeDocument10 pagesDeterminants of Induced Abortion Among Women of Reproductive AgenskhldNo ratings yet
- Correlates of Early Initiation of Breast Feeding and Prelacteal FeedingDocument9 pagesCorrelates of Early Initiation of Breast Feeding and Prelacteal FeedingnskhldNo ratings yet
- Correlation Between Pregnancy Outcome and PlacentalDocument5 pagesCorrelation Between Pregnancy Outcome and PlacentalnskhldNo ratings yet
- Changes in Pregnancy-Associated Deaths in The US During Covid-19Document3 pagesChanges in Pregnancy-Associated Deaths in The US During Covid-19nskhldNo ratings yet
- Challenges and Outcomes of Implementing A National Shypilis Follow-Up SystemDocument12 pagesChallenges and Outcomes of Implementing A National Shypilis Follow-Up SystemnskhldNo ratings yet
- Ppi h2 - Audit Hand HygieneDocument5 pagesPpi h2 - Audit Hand HygienenskhldNo ratings yet
- Antenatal Diagnosis ofDocument6 pagesAntenatal Diagnosis ofnskhldNo ratings yet
- 1597-Article Text-4345-5-10-20220901Document7 pages1597-Article Text-4345-5-10-20220901nskhldNo ratings yet
- Abnormality in A Fetus On UltrasoundDocument2 pagesAbnormality in A Fetus On UltrasoundnskhldNo ratings yet
- HoloprosencephalyDocument4 pagesHoloprosencephalynskhldNo ratings yet
- SKDDocument18 pagesSKDnskhldNo ratings yet
- 1Document1 page1nskhldNo ratings yet
- Dapus MGDocument3 pagesDapus MGnskhldNo ratings yet
- Jdwal Dinas Rs Abunjani AprDocument2 pagesJdwal Dinas Rs Abunjani AprnskhldNo ratings yet
- Med Case Rep. 2020 14 (1) :181. Published 2020 Oct 8Document3 pagesMed Case Rep. 2020 14 (1) :181. Published 2020 Oct 8nskhldNo ratings yet
- Dapus Anemia AplastikDocument2 pagesDapus Anemia AplastiknskhldNo ratings yet
- Nama BannerDocument5 pagesNama BannernskhldNo ratings yet
- Pediatric Cemento Ossifying Fibroma of The Anterior Mandible A Case ReportDocument6 pagesPediatric Cemento Ossifying Fibroma of The Anterior Mandible A Case ReportDessy Dwi UtamiNo ratings yet
- Ergonomics in Dental Practice: January 2014Document12 pagesErgonomics in Dental Practice: January 2014mk78_inNo ratings yet
- Eminectomia Undt PDFDocument18 pagesEminectomia Undt PDFGustavo SierraNo ratings yet
- Oral Disorders of Exotic Ungulates: Felicia Knightly, DVM, Peter Emily, DDS, AVDCDocument6 pagesOral Disorders of Exotic Ungulates: Felicia Knightly, DVM, Peter Emily, DDS, AVDCLeo AriasNo ratings yet
- TREATMENT Algorithm For Bilateral Alveolarcleft Based On The Position of The Premaxillaand The Width of The Alveolar GapDocument7 pagesTREATMENT Algorithm For Bilateral Alveolarcleft Based On The Position of The Premaxillaand The Width of The Alveolar GapFranklin HaroNo ratings yet
- Assessing Coronal Microleakage of Temporary Restorative MaterialsDocument4 pagesAssessing Coronal Microleakage of Temporary Restorative MaterialsIzumi Jugha JavieraNo ratings yet
- Failures in Fixed Partial Dentures: Dr. Rohit FernandezDocument89 pagesFailures in Fixed Partial Dentures: Dr. Rohit FernandezPriyanka GandhiNo ratings yet
- CerkamedDocument4 pagesCerkamedDragana CurcicNo ratings yet
- Etiology of MalocclusionDocument48 pagesEtiology of MalocclusionGilani Syed Sohaib100% (1)
- The Effect of A Lip Bumper On Lower Dental Arch Dimensions and Tooth PositionsDocument6 pagesThe Effect of A Lip Bumper On Lower Dental Arch Dimensions and Tooth PositionsFrancisco Isaí ArciniegaNo ratings yet
- An Overview of Frenal AttachmentsDocument4 pagesAn Overview of Frenal AttachmentsTrần ThưNo ratings yet
- Jpts 195 PDFDocument4 pagesJpts 195 PDFHarshit SinghNo ratings yet
- Tests For Biocompatibility of Dental MaterialsDocument151 pagesTests For Biocompatibility of Dental MaterialsDevanshi SharmaNo ratings yet
- Periodontal ExodontiaDocument5 pagesPeriodontal ExodontiaDARKS_EDSNo ratings yet
- Cap. 10 - RatsDocument17 pagesCap. 10 - RatsNailson JúniorNo ratings yet
- Alpha-Caine Topical Anesthetic-Benzocaine Gel Dental Technologies, IncDocument5 pagesAlpha-Caine Topical Anesthetic-Benzocaine Gel Dental Technologies, Incmathieu motardNo ratings yet
- Apically Extruded Sealers - Fate and Influence On Treatment Outcome 2016Document7 pagesApically Extruded Sealers - Fate and Influence On Treatment Outcome 2016Lorena CândidoNo ratings yet
- Short Assay and MCQ in OperativeDocument65 pagesShort Assay and MCQ in OperativeAli AssimNo ratings yet
- Gingival Overgrowth and Altered Passive Eruption in Adolescents Literature Review and Case ReportDocument8 pagesGingival Overgrowth and Altered Passive Eruption in Adolescents Literature Review and Case ReportAulia ElnisaNo ratings yet
- 2 CLCC 2018 Loading ProtocolsDocument64 pages2 CLCC 2018 Loading ProtocolsAbdul Rahman SalehNo ratings yet
- Clinical EndoDocument16 pagesClinical EndoabdallahNo ratings yet
- Colgate vs. Close-Up: A Comparative Study On The Best Brand of Toothpaste in The PhilippinesDocument4 pagesColgate vs. Close-Up: A Comparative Study On The Best Brand of Toothpaste in The PhilippinesJocelNo ratings yet
- Endodontic Complications Associated With Orthodontic Temporary Anchorage DevicesDocument8 pagesEndodontic Complications Associated With Orthodontic Temporary Anchorage DevicesAlfonso SernaNo ratings yet
- Listerine Segmentation AnalysisDocument24 pagesListerine Segmentation AnalysisVan DatNo ratings yet
- Grammatical Sketch For Readers of AlbanianDocument133 pagesGrammatical Sketch For Readers of AlbanianAna B. AdamsNo ratings yet
- MCQ FOR Dental AmalgamDocument34 pagesMCQ FOR Dental AmalgamZaara RashéidNo ratings yet
- A Conservative Approach ToDocument6 pagesA Conservative Approach ToOdonto Uninassau 4p NoiteNo ratings yet
- No No. RM NIK Nama TGL Lahir Umur JK No Peserta Alamat Kunjungan Unit Baru Lama B L Cara BayarDocument6 pagesNo No. RM NIK Nama TGL Lahir Umur JK No Peserta Alamat Kunjungan Unit Baru Lama B L Cara BayarHappy Septianto SNo ratings yet